Chronic Widespread Pain associated with Vitamin D under 10 ng – meta-analysis
Is Serum Hypovitaminosis D Associated with Chronic Widespread Pain Including Fibromyalgia? A Meta-analysis of Observational Studies
Pain Physician 2015; 18:E877-E887
Ming-Yen Hsiao, MD1, Chen-Yu Hung, MD2, Ke-Vin Chang, MD, PhD1, Der-Sheng Han MD, PhD1, and Tyng-Guey Wang, MD3
Background: Chronic widespread pain (CWP) is a global musculoskeletal disorder leading to disability and a reduced quality of life. Low levels of serum vitamin D has long been proposed to be associated with CWP, but previous research remains inconclusive.
Objectives: To determine whether hypovitaminosis D was independently associated with CWP.
Study Design: Meta-analysis of observational study.
Methods: Electronic databases were searched for studies published up to November 2014 comparing the prevalence of hypovitaminosis D and serum vitamin D levels between participants with and without CWP. The crude and adjusted odds ratios (ORs) of hypovitaminosis D with CWP were calculated. Subgroup analysis according to gender, threshold of hypovitaminosis, and definition of patients was performed, as well as meta-regression to test the linear relationship between crude ORs and the latitude of study locations.
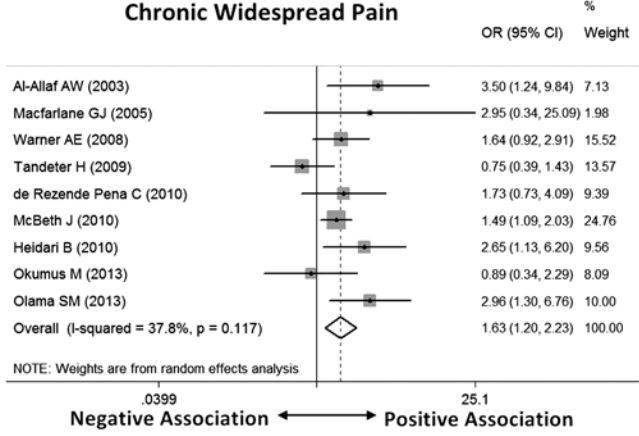
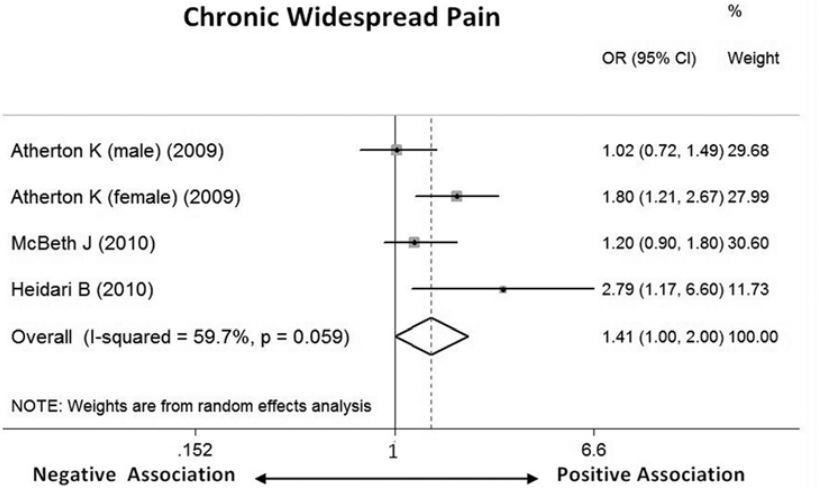
Results: Twelve studies were included, comprising 1,854 patients with CWP. The patient group showed a significantly higher risk of hypovitaminosis D than the control group (crude OR, 1.63; 95% CI, 1.20 - 2.23). The association was slightly attenuated after adjusting confounders, with a pooled adjusted OR of 1.41 (95% CI, 1.00 - 2.00). There was an increase in ORs of hypovitaminosis D using a lower diagnostic value of serum vitamin D (8 and 10 ng/mL) . The subgroup analysis according to gender and definition of CWP did not reveal significant between-group differences. The meta-regression showed no linear relationship between latitude and the crude ORs.
Conclusions: There was a positive crude association between hypovitaminosis D and CWP, and the association was likely to remain after adjusting confounding factors. Use of a cut-off value of hypovitaminosis D (8 - 10 ng/mL) could better define the population with and without CWP. Further prospective follow-up studies are warranted to clarify the causal relationship between hypovitaminosis D and CWP.
Odds Ratio - Crude
Odds Ratio - Adjusted
See also VitaminDWiki
Overview Fibromyalgia or Chronic Fatigue and vitamin D
📄 Download the PDF from VitaminDWiki
Sections extracted from the PDF
Introduction
Chronic widespread pain (CWP), including fibromyalgia, is a global musculoskeletal disorder leading to disability and a reduced quality of life, and has a prevalence ranging from 10% to 18% in the general population (1,2). Concomitant somatic symptoms may present as complaints of circulatory, respiratory, and neurological system problems and impose a tremendous burden on psychosocial and medical care resources (3). The exact pathophysiology remains unclear and possible causal mechanisms include central sensitization of pain perception and reduced levels of antiinflammatory cytokines (4,5). Vitamin D, a hormone precursor essential for maintaining homeostasis of the musculoskeletal system, has long been proposed as an associated factor in CWP. The most severe type of hypovitaminosis D, osteomalacia, features generalized body pain, especially in the shoulder, rib cage, and lumbar and pelvic regions. The biological relationship between CWP and vitamin D deficiency is still under investigation, and may be mediated through vitamin D receptors on muscle tissues and vitamin D's regulatory role in autoimmune responses (6). A number of studies have been conducted to explore the association of low levels of serum vitamin D with diffuse musculoskeletal pain, including fibromyalgia, but the results appear inconclusive. The potential causes of the controversial outcomes were heterogeneity in the study and reference population, different thresholds of defining hypovitaminosis D, and the presence of confounding factors. Therefore, the present meta-analysis aimed to determine whether hypovitaminosis D was associated with CWP syndrome and also investigate whether the association was independent of confounders known to affect vitamin D metabolism.
Discussion
Our meta-analysis, employing data from 12 studies involving 1,854 patients and 7,850 controls, found that participants with CWP were associated with serum hypovitaminosis D and the association was likely to exist after adjusting potential confounding factors. The differences in gender and geographical latitude in which the research was conducted did not pose a significant influence on the association, whereas the studies using a lower serum vitamin D level as the diagnostic threshold of hypovitaminosis D tended to have a higher magnitude of associations.
For decades, there have been debates about whether hypovitaminosis D was related to CWP. A brief review by Heath and Elovic (25) had noted a correlation between vitamin D deficiency and musculoskeletal pain but the evidence was based on several case series and single-arm observational studies. Two systematic reviews in 2009 and 2011 addressed this issue and their results were inconclusive (26,27). The main reasons included heterogeneity in study designs and limited numbers of enrolled trials. In addition, both reviews included participants with rheumatologic conditions like rheumatoid arthritis or localized musculoskeletal pain syndrome along with CWP. None of them proceeded to quantitative analysis. To our knowledge, this is the first meta-analysis providing integrated data regarding the comparison of serum hypovitaminosis D between participants with and without CWP.
Our meta-analysis found a positive crude association between CWP and hypovitaminosis D. The results came from observational studies, which could not infer any causal relationship. Among the 9 studies in which crude ORs were available (13,14,16,1820,22-24), the point estimates of the ORs were found positive in 7 studies (14,16,18,20,22-24), only 4 of which claimed a significant association between CWP and hypovitaminosis D (14,18,22,24). Possible reasons for the lack of statistical significance in the remaining 5 studies (13,16,19,20,23) included small numbers of participants, various definitions of the patient population, heterogeneity of the control participants, and lack of a standardized cut-off value for hypovitaminosis D. Besides, numerous factors are known to affect the serum vitamin D level, including age, gender, and latitudes of study location (28,29).
Our results indicated no significant differences in the crude ORs between the patient populations using patients with defined fibromyalgia syndrome and those without, as well as between the reference groups recruiting asymptomatic participants and patients with localized pain (Table 2). Furthermore, female gender is well recognized for having a higher prevalence of fibromyalgia syndrome (30), but our study did not identify a difference in crude ORs between distinct gender groups. Although vitamin D is produced from sunlight substantially dependent on the latitude of study locations, our meta-regression failed to show a linear relationship between the crude ORs and latitudes.
Another important finding was that lower values (8 - 10 ng/mL) of serum vitamin D as the hypovitamino- sis threshold tended to have higher crude ORs. This was consistent with the research conducted by Atherton et al (21), in which participants were stratified according to different hypovitaminosis thresholds ranging from 10 to 40ng/mL, and demonstrated higher adjusted ORs in the subgroups with a lower range of serum vitamin D. Of note, our data revealed that the pooled mean serum vitamin D levels in the patient and reference groups were 15.48 and 16.02ng/mL, respectively, both lower than the commonly used diagnostic threshold of 20ng/mL. Several reports indicated that 20ng/mL of serum vitamin D was the minimal level to achieve a normal serum parathyroid hormone concentration (31,32). Our analysis revealed that even in the asymptomatic population, physiological vitamin D insufficiency was also prevalent, and a value less than 10ng/mL might be a better diagnostic threshold of hypovitaminosis D to discriminate between participants with and without CWP.
Three of our retrieved citations reported adjusted ORs (21,22,24), the pooled value of which was slightly lower than the crude OR, but borderline statistical significance remained. Multiple known causes such as age, gender, body composition, sun exposure, skin pigmentation, smoking and alcohol consumption, medications, and cultural factors such as veiling can affect the intake or skin production of vitamin D. Of the 3 studies, Heidari et al (22) adjusted the influence of gender difference, and McBeth et al (24) and Atherton et al (21) dealt with seasonal variations, body mass index, physical activity, smoking, and alcohol consumption. If the associations between hypovitaminosis D and CWP all resulted from the above-mentioned confounders, the adjusted OR would be shifted toward the value of one and become insignificant. Therefore, our results implied hypovitaminosis D in patients with CWP might be partly mediated through certain pathways other than well-known confounders, and future cohort studies are warranted to investigate potential causal factors leading to hypovitaminosis in patients with CWP.
There are several limitations in our meta-analysis. First, all retrieved citations employed a cross-sectional observational design and none of them were able to elucidate the causal relationship between hypovitaminosis D and CWP. Although some claimed theirs as prospective cohort studies, their patient and control groups were defined at the same time as serum vitamin D levels were obtained. Second, the literature search also identified some randomized control trials which mainly explored the effect of vitamin D supplement on pain reduction in patients with CWP or fibromyalgia, and therefore were not included in the present metaanalysis. Third, limited numbers of included studies provided adjusted ORs, and substantial differences existed in the items constituting measured confounders. Finally, we noticed significant publication bias in the reporting of mean serum vitamin D levels in both patient and control groups. This could be due to heterogeneity in the observed population, the season and location at which the study was conducted, and the methods of vitamin D measurement. However, we speculated that the publication bias had limited influence on the interpretation of our results since the ORs in the patient and reference groups were similarly distributed in the funnel plot.
In conclusion, our meta-analysis indicated a positive crude association between hypovitaminosis D and CWP, and the association was likely to remain after the adjustment of potential confounding factors. Using a lower value of serum vitamin D (8 - 10 ng/mL) as the diagnostic threshold appeared to be better than the physiological cut-off level (20 ng/mL) in differentiating the population with and without CWP. Further prospective longitudinal follow-up studies are warranted to clarify the causal relationship between CWP and serum hypovitaminosis D.