Spinal Surgery patients – almost all have low vitamin D
> 30 ng of Vitamin D needed for spinal fusion – Sept 2017
Vitamin D: Should we be checking levels before spine fusion?
Seminars in Spine Surgery. online 12 September 2017, https://doi.org/10.1053/j.semss.2017.09.003
Owoicho Adogwa, M.D., M.P.H, Jacob M. Buchowski, M.D., M.S.,
Vitamin D is a prohormone that regulates calcium absorption from the gastrointestinal tract. It plays an important role in calcium homeostasis and Calcium has several important roles in transmission of nerve impulses, muscle contraction and proper mineralization of bone. An alarmingly high prevalence of vitamin D deficiency has been described in numerous segments of the U.S population, with recent studies estimating a prevalence rate of approximately 70%.
Several epidemiological studies have reported direct relationships between low vitamin D levels and multiple disease states. hypovitaminosis D is particularly worrisome in patients undergoing spinal surgery given the high incidence of pseudoarthrosis in this patient cohort. When considering treatment of vitamin D deficiency, it is important to take into account the recommended concentrations and the recommended dietary allowance. Considering the adverse effects of hypovitaminosis D in patients undergoing spine surgery, routine pre-operative screening should be undertaken to identify at-risk patients. In addition, it is important for patients undergoing spinal fusion procedures to maintain a sufficient serum vitamin D concentration(>30ng/mL).
Publisher wants $32 for the PDF
Vitamin D and spine surgery - Nov 2016
World J Orthop 2016 November 18; 7(11): 726-730, DOI: 10.5312/wjo.v7.i11.726
📄 Download the PDF from VitaminDWiki
Thomas Mabey, Weerasak Singhatanadgige, Wicharn Yingsakmongkol, Worawat Limthongkul, Sittisak Honsawek
Thomas Mabey, Sittisak Honsawek, Department of Biochemistry, Faculty of Medicine, Chulalongkorn University, Bangkok 10330, Thailand
Weerasak Singhatanadgige, Wicharn Yingsakmongkol, Worawat Limthongkul, Sittisak Honsawek, Vinai Parkpian Orthopaedic Research Center, Department of Orthopaedics, Faculty of Medicine, Chulalongkorn University, Bangkok 10330, Thailand
Thomas Mabey, Weerasak Singhatanadgige, Wicharn Yingsakmongkol, Worawat Limthongkul, Sittisak Honsawek,
King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok 10330, Thailand
Author contributions: Mabey T collected, analyzed, and drafted the manuscript; Singhatanadgige W, Yingsakmongkol W, Limthongkul W provided the technical support; Honsawek S provided administrative support, the input in writing the paper and coordinated the writing of the paper.
Manuscript source: Invited manuscript
Correspondence to: Sittisak Honsawek, MD, PhD, Vinai Parkpian Orthopaedic Research Center, Department of Orthopaedics, Faculty of Medicine, Chulalongkorn University, Rama IV road, Patumwan, Bangkok 10330,
Thailand. sittisak.h@chula.ac.th Telephone: +66-2-2564482 Fax: +66-2-2564482
Received: May 5, 2016
Peer-review started: May 9, 2016 First decision: July 14, 2016 Revised: August 9, 2016 Accepted: August 30, 2016 Article in press: August 31, 2016 Published online: November 18, 2016
Vitamin D is crucial for musculoskeletal health, maintenance, and function. Vitamin D insufficiency is common among patients undergoing spine surgery and the ideal vitamin D level for spine surgery has yet to be investigated. There is a high prevalence of hypo- vitaminosis D in patients with musculoskeletal pain regardless of surgical intervention. With the frequency and costs of spine surgery increasing, it is imperative that efforts are continued to reduce the impact on patients and healthcare services. Studies into vitamin D and its associations with orthopaedic surgery have yielded alarming findings with regards to the prevalence of vitamin D deficiency. Importantly, altered vitamin D status also contributes to a wide range of disease conditions. Therefore, future investigations are still essential for better understanding the relationship between vitamin D and spine surgery outcomes. Whilst further research is required to fully elucidate the extent of the effects of hypovitaminosis D has on surgical outcomes, it is strongly advisable to reduce the impacts by appropriate vitamin D supplementation of deficient and at-risk patients.
Core tip:
A growing body of evidence suggests that vitamin D plays an essential role in skeletal development, bone remodeling, fracture repair, and muscle strength. Vitamin D deficiency is highly prevalent in the elderly and underestimated by spine surgeons. Studies into vitamin D and its associations with orthopaedic surgery have yielded alarming findings with regards to the prevalence of vitamin D deficiency. Importantly, altered vitamin D status also contributes to a wide range of disease conditions and surgical outcome. Therefore, further investigations are still essential for better understanding paradoxical relationship between vitamin D status and spine surgery outcome.
Mabey T, Singhatanadgige W, Yingsakmongkol W, Limthongkul W, Honsawek S. Vitamin D and spine surgery. World J Orthop 2016; 7(11): 726-730 Available from: http://www.wjgnet.com/2218-5836/full/v7/in/726.htm DOI: http://dx.doi.org/10.5312/wjo.v7.i11.726
INTRODUCTION
A growing body of evidence suggests that vitamin D plays an essential role in skeletal development, bone remodeling, fracture repair, and muscle strength. Vitamin D deficiency is highly prevalent in the elderly and underestimated by spine surgeons. With the frequency and costs of spine surgery increasing, it is imperative that efforts are continued to reduce the impact on patients and healthcare services. Studies into vitamin D and its associations with orthopaedic surgery have yielded alarming results with regards to the prevalence of vitamin D deficiency. Generally speaking, serum 25-hydroxyvitamin D [25(OH)D] concentrations of less than 20 ng/mL are considered insufficient and below 10 ng/mL are deficient. However, there is still no standardised definition of where hypovitaminosis D starts, in part because of the conflicting data. What is largely agreed on though is that alarming numbers of the global population have insufficient vitamin D levels.
Vitamin D acts via the vitamin D receptor (VDR) on a range of tissues where it has multiple effects (reviewed in detail by Hossein-nezhad et a/1]). Perhaps most well- known is the way in which activated vitamin D acts on the kidneys and intestines to regulate calcium and phosphorus concentrations in the blood. In addition to this vital function, vitamin D is well known for its involvement in bone metabolism[2]. The induction of both bone formation and remodelling seems at first glance to be somewhat paradoxical. However, there exists strong links between bone mineral density (BMD) and vitamin D levels.
As we explore below, surgical outcomes are hindered by low vitamin D levels. Complications including recurrent fractures, insufficient tissue repair, and loosening of surgical hardware often require further surgeries and therapeutic intervention to ameliorate. Using simple and reasonable measures through the administration of vitamin D supplementation to reduce these effects would be a logical step in the continued effort to improve patient care and minimise financial expenditures.
VITAMIN D IN SPINE SURGERY
Despite the frequency of spinal surgery, particularly in elderly patients, there is a scarcity of research on vitamin D levels and surgical outcomes. However, a number of case studies have indicated the importance of healthy vitamin D levels. In two cases of severe hypovitaminosis D unsuccessful outcomes of spinal fusion surgery were observed, but following high vitamin D supplementation patients improved[3]. Likewise, a 76-year-old female with osteoporosis and circulating 25(OH)D levels of 9 ng/mL suffered compression fractures in thoracic and lumbar vertebrae. Following kyphoplasty, the patient reported no improvement in pain and suffered a further lumbar compression fracture, whereafter she received 2200 IU/d of vitamin D supplementation. Impressive clinical improvements were noted in muscle strength and a decrease in back pain[4]. This is supported by a study of 40 patients with acute symptomatic vertebral compression fractures who underwent kyphoplasty surgery[5]. When investigating the recurrence rate of fractures, serum 25(OH)D concentrations were higher in patients with no new fractures post-operatively compared with those who had suffered additional fractures, but lumbar BMD scores showed no significant difference. Schwalfenberg[6] reported 6 cases of improvements in back pain and failed back surgery patients through vitamin D supplementation. Patients respond over a range of time frames from 3 to 6 wk and whilst all patients showed improvements in pain, some responded better to treatment. It is suggested that 4000-5000 IU/d of vitamin D supplements may be required to improve the patients' conditions. An interesting observation was the improvement in mood noted in some cases, whether through direct psychoactive effects of vitamin D or as a result of decreased pain; it is another aspect to consider when evaluating vitamin D.
Moreover, Waikakul[7] investigated the association of serum 25(OH)D levels with pain and low back function in patients with failed back surgery syndrome. Of the nine cases, an initial 20000 IU loading dose of ergocalciferol, followed by daily doses of 600 IU of cholecalciferol showed improvements in all but one patient for pain and Japanese Orthopaedic Association (JOA) back scores. At 6 mo follow-up, patients continued to improve with just 2 experiencing only slight improvements. It suggests that high loading doses followed by prolonged use of maintenance doses can improve the functional scores of patients. Supporting this, a longitudinal study of 360 idiopathic low back pain patients in Saudi Arabia found that, at baseline, only 17% had normal vitamin D levels[8]. Patients were given high doses of vitamin D (5000-10000 IU/d) for 3 mo. At follow up 95% of patients reported the disappearance of low back pain and all patients had gained normal serum 25(OH)D levels. Finally, in a prospective follow-up study of 31 females undergoing posterior decompression surgery and instrumented posterolateral fusion for lumbar spinal stenosis, post-operative (1 year follow-up) vitamin D levels were positively correlated with surgery outcome scores. The authors also remark the high prevalence of deficient vitamin D levels in lumbar spinal stenosis patients[9]. These reports showcase the risks to surgical outcomes of hypovitaminosis D, but also the possible benefits of vitamin D supplementation. High and maintained vitamin D treatment appears to be effective at both ameliorating surgical procedures, for example bone grafts and hardware fusion, and patients' symptoms including pain, function, and mood, which in turn often alleviates the need for analgesics.
A number of studies have reported alarmingly high prevalences of insufficient or deficient vitamin D levels in orthopaedic spine patients. A retrospective study of 313 adults undergoing spinal fusion by Stoker et a/10] found circulating 25(OH)D concentrations in nearly 90% of patients were insufficient or deficient (< 30 ng/mL); 3.5% were classified as severely deficient (< 10 ng/mL). Whilst females are often regarded as being at higher risk of hypovitaminosis D; no difference was observed between male and female patients, though vitamin D deficient patients tended to have higher pain and worse disability scores. Similarly, when Kim et a/11] examined vitamin D levels in 350 lumbar spinal stenosis patients with chronic low back pain and leg pain, they found that there was a high prevalence of hypovitaminosis D, only 2.9% of participants being vitamin D sufficient (> 30 ng/mL). Vitamin D deficiency was associated with both low back pain and leg pain in addition to sun light exposure. Furthermore, in Norway, a study of 572 patients complaining of headaches, fatigue, and musculoskeletal pain observed a high prevalence of vitamin D deficiency. The prevalence was affected by ethnicity; 83% of South Asian and African patients, but only 35% of native Norwegian patients were hypovitaminosis D sufferers[12].
In a cross sectional study of 400 individuals, there was a positive association between vitamin D levels and low BMD in both males and females that was independent of age, although vitamin D deficient participants were older than those with normal levels. Of the deficient participants, 100% had lumbar and hip BMD scores in the range of osteopenia or consistent with osteoporosis[13]. Whilst age is a recognised risk factor of vitamin D deficiency, younger patients should not be assumed to have healthy levels as shown by a study of the 70 paediatric orthopaedic patients undergoing long bone osteotomies, hip osteotomies, and spinal fusions studied by Parry et a/14], 90% of whom had subnormal vitamin D concentrations with 16% being severely deficient (< 12 ng/mL). Cholecystectomy put spine patients at an increased risk of vitamin D deficiency[15]. When classified into two groups - those who had previously undergone a cholecystectomy and those who had not - 40.8% of previous cholecystectomy patients were vitamin D deficient (< 20 ng/mL) compared to 25% of non-cholecystectomy patients. The aforementioned studies suggest the need to identify at-risk patients, particularly older patients and those who have histories of low bone density or medical conditions affecting bone metabolism.
Lumbar spine BMD has been shown to be decreased in low vitamin D patients as shown by the lumbar BMD scores of physically active and normal adolescent females in Israel which showed all participants were vitamin D insufficient (< 30 ng/mL) with 64% being defined as deficient (< 14 ng/mL). Furthermore, activity is associated with lumbar BMD and BMD scores are most strongly associated with the lowest tertile of 25(OH)D levels[16]. However, in Swiss teenagers with appendicular fractures, there was no difference between healthy individuals and those with fractures in vitamin D levels or lumbar or heel BMD, nor was there a difference between fracture sites. Despite a high prevalence of hypovitaminosis D, there was no association between vitamin D levels and spinal BMD[17]. Low BMD increases the risk of failure in surgical procedures, especially the application of hardware, for instance in spinal fusion. The vitamin D levels of patients, principally the elderly, should be maintained at satisfactory levels prior to and proceeding surgeries. Equally important is the activity of patients. Excessive and unnecessary use of back support braces can lead to weakening of the supportive muscles in the back, which in turn can lead to pain and less successful surgical outcomes. It should also be noted that genetic factors may contribute to the outcome of spine surgery. VDR gene polymorphisms where investigated by in a cross-sectional study of 318 postmenopausal females in Japan indicated that a VDR haplotype was associated with the severity of spondylosis in lumbar spine[18].
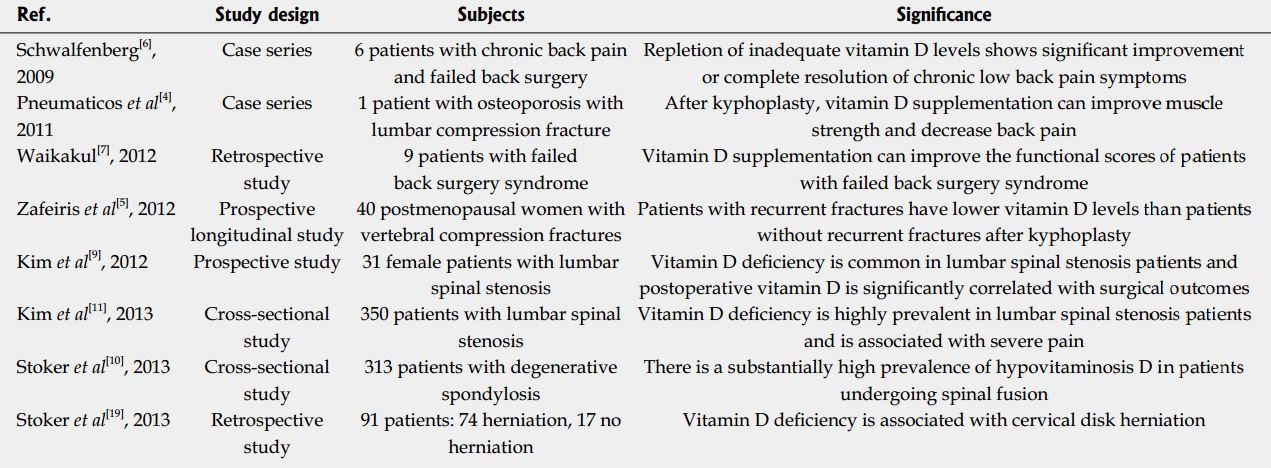
A retrospective investigation of orthopaedic patients undergoing cervical, thoracic, and lumbar disk replacements, decompressions, and arthroplasty revealed vitamin D deficiency (< 20 ng/mL) to be associated with cervical disk herniation, in particular, the number of herniations. The likelihood of disc herniation was higher in patients with lower vitamin D levels[19]. Research has been focused on investigating possible relationships between vitamin D status and clinical outcome in patients with spine surgery, as summarized in Table 1.
Table 1
There is a disturbingly high prevalence of hypovita- minosis D in orthopaedic patients around the world. Low vitamin D levels appear to be the cause of many failed spinal surgeries, but despite the importance, and apparent severity, little research has been performed on the associations with surgical outcomes. With the relative inexpensiveness and safety of vitamin D supplementation, it would be prudent to screen for low circulating 25(OH)D concentrations and treat those found to be insufficient in an attempt to increase the chances of successful procedural outcomes.
Low vitamin D status is associated with a variety of studies of vitamin status in patients with spine surgery of adverse outcomes following surgical procedures. In recent years, previous investigation has documented that serum 25(OH)D level at the time of operation is highly predictive of long term surgical outcomes compared to postoperative vitamin D status, and that benefits can be attained by vitamin D supplementation at the time of surgical procedures or thereafter[20].
Vitamin D status is a prognosticator of extraskeletal abnormalities for which predispositions could be detected and deficiencies should be corrected before surgical treatments. Our recommendation for patients with vitamin D deficiency prior to elective spine surgery is as follows. In patients whose 25(OH)D is less than 20 ng/ mL, treatment generally includes initial 50000 IU loading dose of vitamin D orally once weekly for two to three months , and then 1000 or more IU of vitamin D daily thereafter. After three months, serum 25(OH)D should be reassessed. In patients whose 25(OH)D is 20-30 ng/ mL, treatment includes 1000 IU of vitamin D by mouth daily, commonly for a three-month period. However, some patients may require higher doses. The ideal dose of vitamin D is determined by measuring serum 25(OH)D, and increasing the dose if serum vitamin D level is not within the normal range. Once a normal level is achieved, continued therapy with 800 IU of vitamin D daily is generally suggested. Although various strategies could be used in treating vitamin D deficiency, a common overlooking in management is to discontinue treatment or administer inadequate vitamin D maintenance dosing when the serum 25(OH)D level reaches the optimal range. It is, therefore, reasonable to routinely screen all patients undergoing spine fusion surgery for serum 25(OH)D levels, and those with vitamin D deficiency should be given vitamin D supplements.
CONCLUSION
Heretofore, limited research has been conducted into the associations of vitamin D and spine surgical outcomes. However, the existing evidence shows a need to improve vitamin D levels in patients with unsatisfactory results. There is an alarmingly high prevalence of subnormal vitamin D levels among orthopaedic patients reported in the literature. Considering the detrimental impact of hypovitaminosis D in patients undergoing spine surgery, preoperative vitamin D screening may be needed for those at high risk of deficiency. Whilst further research is required to fully elucidate the extent of the effects of hypovitaminosis D on clinical outcomes, it is strongly advisable to reduce the impacts by appropriate supplementation of deficient and at-risk patients to adequate levels.
ACKNOWLEDGEMENTS:The authors thank the National Research University Project, Office of the Higher Education Commission through the Ageing Cluster (NRU59-056-AS), Chulalong- korn University.