Vitamin D interactions with poor gut (Celiac, IBD, and Bariatric surgery) – several studies
IBD best practice advice includes Vitamin D - Jan 2024
AGA Clinical Practice Update on Diet and Nutritional Therapies in Patients With Inflammatory Bowel Disease: Expert Review
Gastroenterology. 2024 Jan 23:S0016-5085(23)05597-X. doi: 10.1053/j.gastro.2023.11.303
Jana G Hashash 1, Jaclyn Elkins 2, James D Lewis 3, David G Binion 4
Description: Diet plays a critical role in human health, but especially for patients with inflammatory bowel disease (IBD). Guidance about diet for patients with IBD are often controversial and a source of uncertainty for many physicians and patients. The role of diet has been investigated as a risk factor for IBD etiopathogenesis and as a therapy for active disease. Dietary restrictions, along with the clinical complications of IBD, can result in malnutrition, an underrecognized condition among this patient population. The aim of this American Gastroenterological Association (AGA) Clinical Practice Update (CPU) is to provide best practice advice statements, primarily to clinical gastroenterologists, covering the topics of diet and nutritional therapies in the management of IBD, while emphasizing identification and treatment of malnutrition in these patients. We provide guidance for tailored dietary approaches during IBD remission, active disease, and intestinal failure. A healthy Mediterranean diet will benefit patients with IBD, but may require accommodations for food texture in the setting of intestinal strictures or obstructions. New data in Crohn's disease supports the use of enteral liquid nutrition to help induce remission and correct malnutrition in patients heading for surgery. Parenteral nutrition plays a critical role in patients with IBD facing acute and/or chronic intestinal failure. Registered dietitians are an essential part of the interdisciplinary team approach for optimal nutrition assessment and management in the patient population with IBD.
Methods: This expert review was commissioned and approved by the AGA Clinical Practice Updates Committee and the AGA Governing Board to provide timely guidance on a topic of high clinical importance to the AGA membership and underwent internal peer review by the CPU Committee and external peer review through standard procedures of Gastroenterology. The best practice advice statements were drawn from reviewing existing literature combined with expert opinion to provide practical advice on the role of diet and nutritional therapies in patients with IBD. Because this was not a systematic review, formal rating of the quality of evidence or strength of the presented considerations was not performed. Best Practice Advice Statements
BEST PRACTICE ADVICE 1: Unless there is a contraindication, all patients with IBD should be advised to follow a Mediterranean diet rich in a variety of fresh fruits and vegetables, monounsaturated fats, complex carbohydrates, and lean proteins and low in ultraprocessed foods, added sugar, and salt for their overall health and general well-being. No diet has consistently been found to decrease the rate of flares in adults with IBD. A diet low in red and processed meat may reduce ulcerative colitis flares, but has not been found to reduce relapse in Crohn's disease.
BEST PRACTICE ADVICE 2: Patients with IBD who have symptomatic intestinal strictures may not tolerate fibrous, plant-based foods (ie, raw fruits and vegetables) due to their texture. An emphasis on careful chewing and cooking and processing of fruits and vegetables to a soft, less fibrinous consistency may help patients with IBD who have concomitant intestinal strictures incorporate a wider variety of plant-based foods and fiber in their diets.
BEST PRACTICE ADVICE 3: Exclusive enteral nutrition using liquid nutrition formulations is an effective therapy for induction of clinical remission and endoscopic response in Crohn's disease, with stronger evidence in children than adults. Exclusive enteral nutrition may be considered as a steroid-sparing bridge therapy for patients with Crohn's disease.
BEST PRACTICE ADVICE 4: Crohn's disease exclusion diet, a type of partial enteral nutrition therapy, may be an effective therapy for induction of clinical remission and endoscopic response in mild to moderate Crohn's disease of relatively short duration.
BEST PRACTICE ADVICE 5: Exclusive enteral nutrition may be an effective therapy in malnourished patients before undergoing elective surgery for Crohn's disease to optimize nutritional status and reduce postoperative complications.
BEST PRACTICE ADVICE 6: In patients with IBD who have an intra-abdominal abscess and/or phlegmonous inflammation that limits ability to achieve optimal nutrition via the digestive tract, short-term parenteral nutrition may be used to provide bowel rest in the preoperative phase to decrease infection and inflammation as a bridge to definitive surgical management and to optimize surgical outcomes.
BEST PRACTICE ADVICE 7: We suggest the use of parenteral nutrition for high-output gastrointestinal fistula, prolonged ileus, short bowel syndrome, and for patients with IBD with severe malnutrition when oral and enteral nutrition has been trialed and failed or when enteral access is not feasible or contraindicated.
BEST PRACTICE ADVICE 8: In patients with IBD and short bowel syndrome, long-term parenteral nutrition should be transitioned to customized hydration management (ie, intravenous electrolyte support and/or oral rehydration solutions) and oral intake whenever possible to decrease the risk of developing long-term complications. Treatment with glucagon-like peptide-2 agonists can facilitate this transition.
BEST PRACTICE ADVICE 9: All patients with IBD warrant regular screening for malnutrition by their provider by means of assessing signs and symptoms, including unintended weight loss, edema and fluid retention, and fat and muscle mass loss. When observed, more complete evaluation for malnutrition by a registered dietitian is indicated. Serum proteins are no longer recommended for the identification and diagnosis of malnutrition due to their lack of specificity for nutritional status and high sensitivity to inflammation.
BEST PRACTICE ADVICE 10: All patients with IBD should be monitored for vitamin D and iron deficiency. Patients with extensive ileal disease or prior ileal surgery (resection or ileal pouch) should be monitored for vitamin B12 deficiency.
BEST PRACTICE ADVICE 11: All outpatients and inpatients with complicated IBD warrant co-management with a registered dietitian, especially those who have malnutrition, short bowel syndrome, enterocutaneous fistula, and/or are requiring more complex nutrition therapies (eg, parenteral nutrition, enteral nutrition, or exclusive enteral nutrition), or those on a Crohn's disease exclusion diet. We suggest that all newly diagnosed patients with IBD have access to a registered dietitian.
BEST PRACTICE ADVICE 12: Breastfeeding is associated with a lower risk for diagnosis of IBD during childhood. A healthy, balanced, Mediterranean diet rich in a variety of fruits and vegetables and decreased intake of ultraprocessed foods have been associated with a lower risk of developing IBD.
Vitamin D and malabsorptive gastrointestinal conditions: A bidirectional relationship? Feb 2023
Reviews in Endocrine and Metabolic Disorders https://doi.org/10.1007/s11154-023-09792-7
Andrea Giustina1,2 • Luigi di Filippo1 • Agnese Allora1 • Daniel D. Bikle3 • Giulia Martina Cavestro4 •
David Feldman5 • Giovanni Latella6 • Salvatore Minisola7 • Nicola Napoli8 • Silvia Trasciatti9 • Melin Uygur1,10 •
PDF Table of Contents
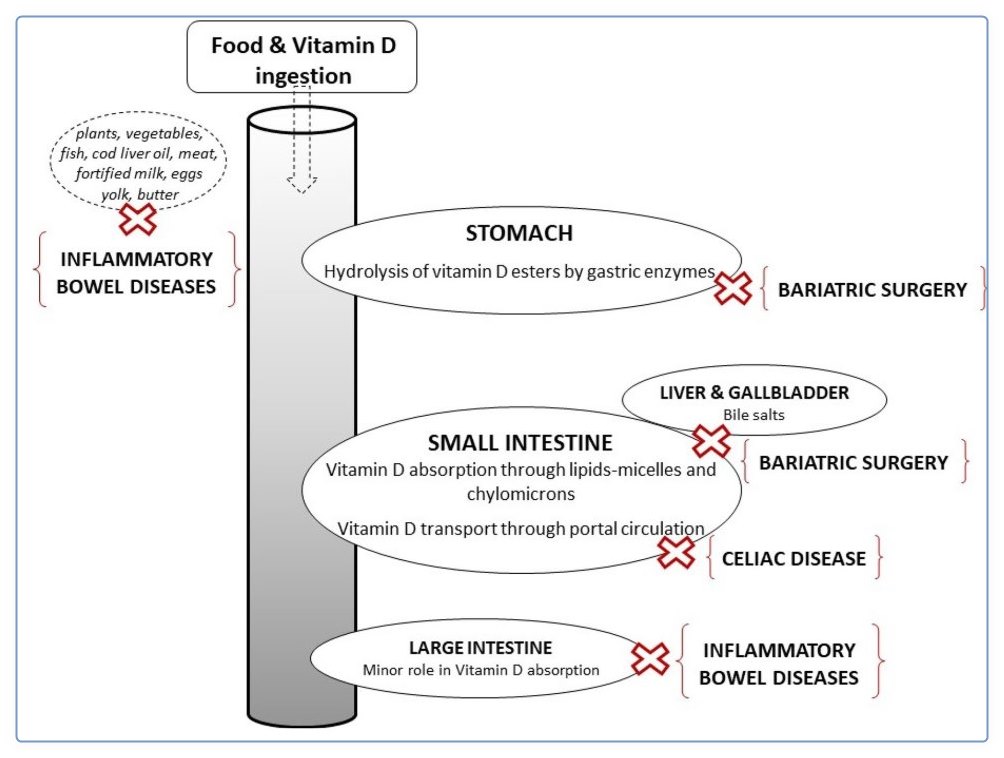

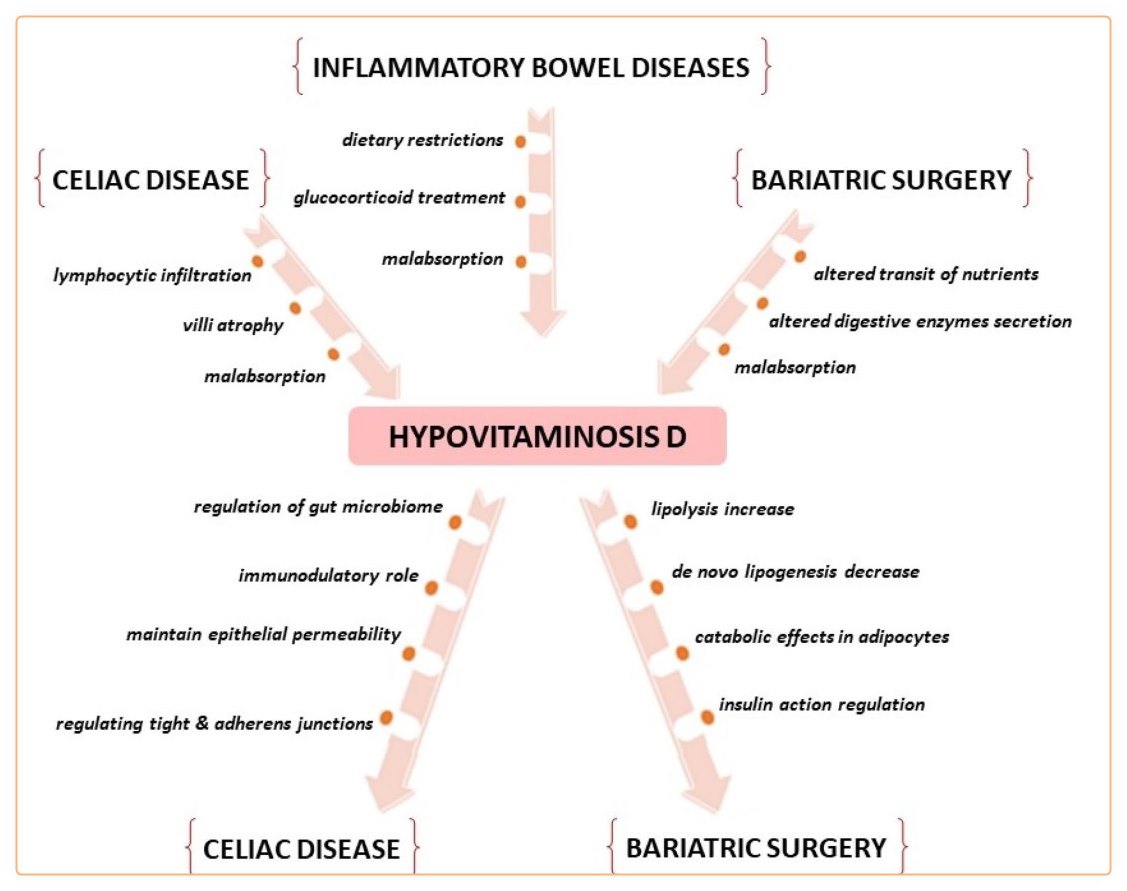
This paper is one of the outcomes of the 5 th International Conference "Controversies in Vitamin D" held in Stresa, Italy from 15 to 18 September 2021 as part of a series of annual meetings which was started in 2017. The scope of these meetings is to discuss controversial issues about vitamin D. Publication of the outcomes of the meeting in international journals allows a wide sharing of the most recent data with the medical and academic community. Vitamin D and malabsorptive gastrointestinal conditions was one of the topics discussed at the meeting and focus of this paper. Participants to the meeting were invited to review available literature on selected issues related to vitamin D and gastrointestinal system and to present their topic to all participants with the aim to initiate a discussion on the main outcomes of which are reported in this document. The presentations were focused on the possible bidirectional relationship between vitamin D and gastrointestinal malabsorptive conditions such as celiac disease, inflammatory bowel diseases (IBDs) and bariatric surgery. In fact, on one hand the impact of these conditions on vitamin D status was examined and on the other hand the possible role of hypovitaminosis D on pathophysiology and clinical course of these conditions was also evaluated. All examined malabsorptive conditions severely impair vitamin D status. Since vitamin D has known positive effects on bone this in turn may contribute to negative skeletal outcomes including reduced bone mineral density, and increased risk of fracture which may be mitigated by vitamin D supplementation. Due to the immune and metabolic extra-skeletal effects there is the possibility that low levels of vitamin D may negatively impact on the underlying gastrointestinal conditions worsening its clinical course or counteracting the effect of treatment. Therefore, vitamin D status assessment and supplementation should be routinely considered in all patients affected by these conditions. This concept is strengthened by the existence of a possible bidirectional relationship through which poor vitamin D status may negatively impact on clinical course of underlying disease. Sufficient elements are available to estimate the desired threshold vitamin D level above which a favourable impact on the skeleton in these conditions may be obtained. On the other hand, ad hoc controlled clinical trials are needed to better define this threshold for obtaining a positive effect of vitamin D supplementation on occurrence and clinical course of malabsorptive gastrointestinal diseases.
📄 Download the PDF from VitaminDWiki
8+ VitaminDWiki pages with CELIAC in title
This list is automatically updated
{LIST()}
About 1% of the population has Celiac Disease
30+ VitaminDWiki pages with IBD in title
This list is automatically updated
{LIST()}
IBD risk reduced 16% if had been taking fish oil (Omega-3) supplements - Oct 2023
https://doi.org/10.1093/ibd/izad262
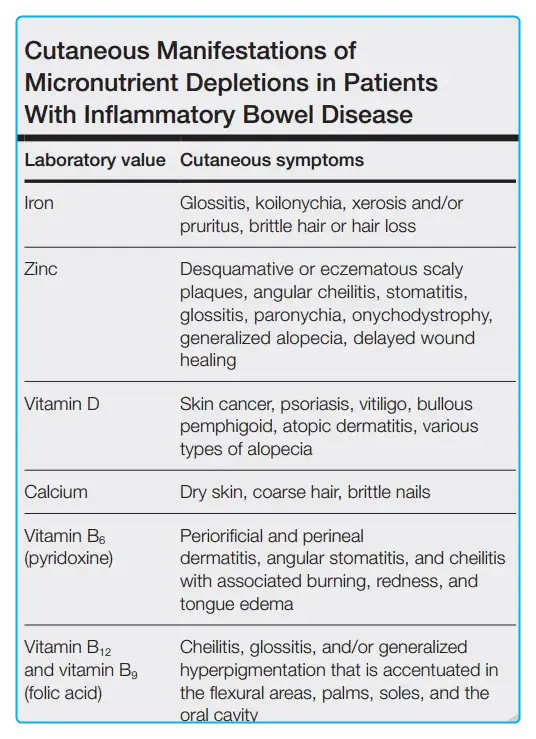
Reduced Nutrients due to IBD causes various skin problems - April 2024
Micronutrient Deficiencies in Patients With Inflammatory Bowel Disease
📄 Download the PDF from VitaminDWiki
See also Bariatric Surgery and Vitamin D - many studies
15+ VitaminDWiki pages with BARIATRIC in title
This list is automatically updated
{LIST()}
~200,000 Baritatric Surgeries in the US in 2020
Most of which significantly reduce the time to adsorb nutrients such as Vitamin D
solutions 1) Increase Vitamin D supplementation, 2) Use a non-oral form of Vitamin D
VitaminDWiki – Overview Gut and vitamin D has
{include}
VitaminDWiki – Overview Gut and vitamin D contains gut-friendly information__
{include}
VitaminDWiki – Gut category contains
{include}
VitaminDWiki – Irritable Bowel Syndrome and Vitamin D - many studies 19 as of June 2023
Asked Chat-GPT to compare IBS with IBD
Irritable Bowel Syndrome ( IBS ) and Inflammatory Bowel Disease ( IBD ) are both chronic conditions that affect the digestive system, but they are distinct in their underlying causes, symptoms, and treatments. Here’s a comparison:
Nature of the Condition:
IBS : It is a functional disorder, which means the symptoms are not associated with any visible signs of damage or disease in the digestive tract. It affects how the bowel functions.
IBD : It is an autoimmune disease that involves chronic inflammation of the digestive tract. There is visible inflammation and damage to the digestive tract.
Common Forms:
IBS : It doesn't have different forms but can be classified based on the predominant symptom ( IBS -D for diarrhea predominant, IBS -C for constipation predominant, IBS -M for mixed).
IBD : Common forms are Crohn's disease and ulcerative colitis.
Symptoms:
IBS : Abdominal pain, bloating, gas, diarrhea, constipation, mucus in the stool. The pain is often relieved by a bowel movement.
IBD : Abdominal pain, cramping, diarrhea, weight loss, fatigue, reduced appetite, blood in the stool, joint pain, and fevers.
Cause:
IBS : The exact cause is not known but it is thought to be related to a combination of abnormal gastrointestinal tract movements, increased sensitivity to pain, and possibly an imbalance of gut bacteria.
IBD : It is believed to be caused by an abnormal immune response, where the immune system attacks the cells of the digestive tract. Genetics, environmental factors, and an imbalance of gut bacteria are also thought to play a role.
Diagnosis:
IBS : Usually diagnosed based on symptoms and exclusion of other diseases. There are no specific laboratory tests to diagnose IBS .
IBD : Can be diagnosed through blood tests, stool tests, endoscopy, and imaging studies which show inflammation and damage in the digestive tract.
Treatment:
IBS : Treatment focuses on relieving symptoms. This may include changes in diet, medications to treat diarrhea or constipation, and stress reduction.
IBD : Treatment aims to reduce inflammation. This often involves medications such as anti-inflammatory drugs, immune system suppressors, and sometimes surgery to remove damaged portions of the digestive tract.
Complications:
IBS : It generally doesn’t cause complications but can significantly impact quality of life.
IBD : Can lead to serious complications such as strictures, abscesses, malnutrition, and increased risk of colon cancer.
Prevalence:
IBS : Is more common compared to IBD .
IBD : Less common but tends to be more severe.
It's important to note that although they have similarities in symptoms, IBS and IBD are fundamentally different. Proper diagnosis and management are crucial for both conditions. Always consult a healthcare provider for advice and information regarding diagnosis and treatment.