Hypertension treatment needs at least 600 mg of Magnesium (49 trials)
Effectively Prescribing Oral Magnesium Therapy for Hypertension: A Categorized Systematic Review of 49 Clinical Trials
Nutrients 2021, 13(1), 195; https://doi.org/10.3390/nu13010195
Andrea Rosanoff 1,* , Rebecca B. Costello 1 and Guy H. Johnson 2
1 CMER Center for Magnesium Education &Research;, Pahoa, HI 96778, USA
2 Johnson Nutrition Solutions LLC, Minneapolis, MN 55416, USA
Trials and meta-analyses of oral magnesium for hypertension show promising but conflicting results. An inclusive collection of 49 oral magnesium for blood pressure (BP) trials were categorized into four groups: (1) Untreated Hypertensives; (2) Uncontrolled Hypertensives; (3) Controlled Hypertensives; (4) Normotensive subjects. Each group was tabulated by ascending magnesium dose. Studies reporting statistically significant (p < 0.05) decreases in both systolic BP (SBP) and diastolic BP (DBP) from both baseline and placebo (if reported) were labeled “Decrease”; all others were deemed “No Change.” Results: Studies of Untreated Hypertensives (20 studies) showed BP “Decrease” only when Mg dose was >600 mg/day; <50% of the studies at 120–486 mg Mg/day showed SBP or DBP decreases but not both while others at this Mg dosage showed no change in either BP measure. In contrast, all magnesium doses (240–607 mg/day) showed “Decrease” in 10 studies on Uncontrolled Hypertensives. Controlled Hypertensives, Normotensives and “magnesium-replete” studies showed “No Change” even at high magnesium doses (>600 mg/day). Where magnesium did not lower BP, other cardiovascular risk factors showed improvement. Conclusion: Controlled Hypertensives and Normotensives do not show a BP-lowering effect with oral Mg therapy, but oral magnesium (≥240 mg/day) safely lowers BP in Uncontrolled Hypertensive patients taking antihypertensive medications, while >600 mg/day magnesium is required to safely lower BP in Untreated Hypertensives; <600 mg/day for non-medicated hypertensives may not lower both SBP and DBP but may safely achieve other risk factor improvements without antihypertensive medication side effects.
📄 Download the PDF from VitaminDWiki
Clipped from PDF
Form of Magnesium
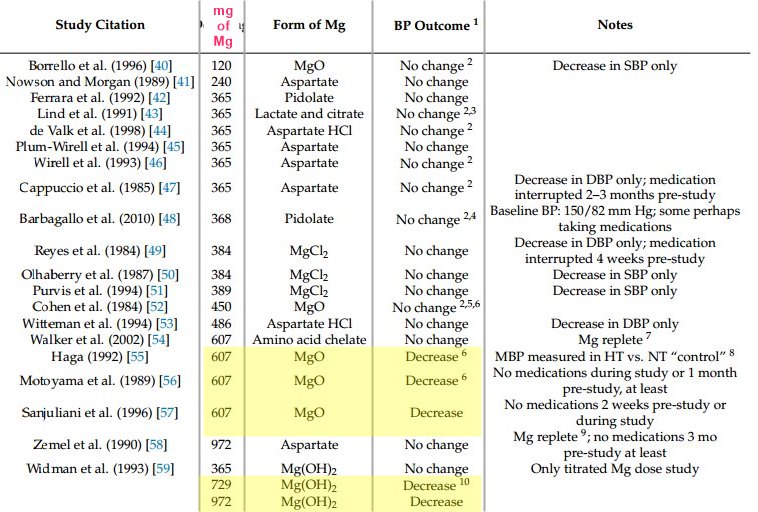
Several forms of magnesium, both organic and inorganic, were used in these studies, and it is interesting to note that the only effective doses of >600 mg/day in Untreated Hypertensives were in studies using MgO , often noted in advertising as being poorly absorbed.
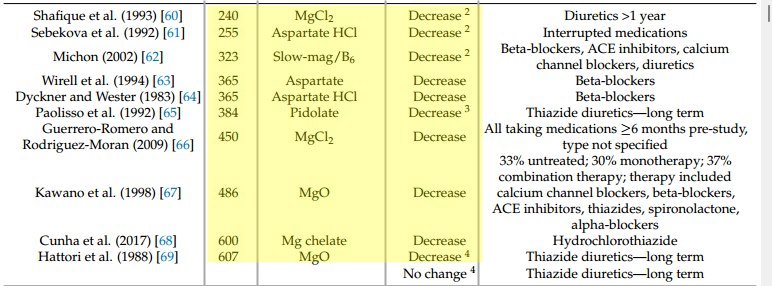
Magnesium given as aspartate, chloride, oxide, pidolate, lactate, citrate, amino- acid chelate at doses below 600 mg/day were not effective in this category . It was Mg dose, not form of Mg, that made the difference. Likewise, the several forms of magnesium showing BP-lowering effects in Uncontrolled Hypertensives (Table 2) included six forms of magnesium, both organic and inorganic, including MgO, and all were effective in lowering BP by the criteria of this analysis.
Safety of Magnesium Doses in Effective Range
Effective magnesium doses in this analysis ranged from 240 to 972 mg/day. For Untreated Hypertensives, the minimum effective dose was >600 mg/day. The tolerable upper intake level (UL) of magnesium for non-food sources is 350 mg/day for adults [15,89]. However, this UL was based on limited data and “although a few studies have noted mild diarrhea and other mild gastrointestinal complaints in a small percentage of patients at levels of 360 to 380 mg per day, it is noteworthy that many other individuals have not encountered such effects even when receiving substantially more than this UL of supplementary magnesium" [18].
Very high intakes of magnesium supplements can be dangerous, even to people without renal or intestinal disease, but such concentrations of magnesium supplement intake are in the range of >5000 mg magnesium/d , i.e., >10-fold higher than the additional amounts discussed in this article [15,90].
Discussion
This categorization clearly shows that NT study subjects, both Controlled Hypertensives and Normotensive (i.e., those with an untreated healthy BP), will not show lower BP with oral magnesium therapy, even at high doses. However, several studies in these normotensive categories reported significant improvement in blood magnesium, lipoproteins, C-reactive protein, fasting glucose and insulin resistance, reversal of retinal vasospasm and increased sodium excretion, all of cardiovascular risk factor benefit. Oral magnesium therapy in NT patients, treated with antihypertensive medications or not, may not show improved BP readings, but these individuals may benefit from improved cardiovascular risk factors.
Among subjects who are hypertensive (>140/90 mm Hg; MBP > 106 mm Hg) at baseline, both low and high doses of oral magnesium therapy show significant decreases in both SBP and DBP only if the subjects are concurrently taking antihypertensive medications, i.e., partially or Uncontrolled Hypertensives. In the studies of Untreated Hypertensive subjects taking no antihypertensive medications, only the studies with Mg supplement doses >600 mg/day demonstrated statistically significant improvements in blood pressure by the criteria of this analysis. Subjects on lower magnesium doses showed other improvements in measures important to cardiovascular health such as serum magnesium, endothelial function and sodium excretion.
Magnesium-replete subjects, even those who are hypertensive, did not show a decrease in BP with oral magnesium therapy, even at doses as high as 972 mg/day [58]. This finding indicates that a person can have adequate magnesium status and still have high BP. Other essential electrolytes besides magnesium can impact BP. For these patients, potassium could be low, especially when concurrent with a high sodium and/or low calcium intake.
The main limitation to this study is the lack of quantification of the BP changes, instead using the statistics and conclusions from each individual study, which varied widely. This study is not a precise meta-analysis and makes no attempt to fully quantify the impact of the categories derived from this analysis. This, rather, is the job of future meta-analyses, and we see this categorization as a preliminary study to guide future meta-analysis that may provide enhanced information about oral Mg therapy for BP while hopefully achieving lower heterogeneity than existing meta-analyses without losing precision. Nonetheless, this categorization of studies by hypertensive as well as medication status plus magnesium dose yields an informative framework for the prescription of oral magnesium therapy for high BP. It well accommodates large and small studies (n = 7-227 receiving magnesium therapy), short-term and long-term studies (2-26 weeks), 11 different forms of magnesium preparations (four inorganic and seven organic), parallel as well as crossover study designs, and placebo control or not (see Michon et al. [62], Sebekova et al. [61], Shafique et al. [60], Motoyama et al. [56], Cohen et al. [52], and Haga [55], which are studies not included in most meta-analyses due to no true placebo group).
Over 30 years ago, magnesium was shown to alter vascular constriction [91] and several studies have since shown that the physiology and cellular biochemistry of magnesium is important to the functionality of endothelial and smooth muscle cells and regulation of vascular tone [92]. Decreased magnesium concentrations have been implicated in altered vascular reactivity, endothelial dysfunction, vascular inflammation, and structural remodeling [93]. Low dietary magnesium has been associated with a higher risk of hypertension [94]. In the United States, 67% of the population aged >51 years is low in dietary magnesium [95] and 55% of adults aged 19 to 50 years, 60% aged 51 to 70 years, and 78% aged >71 years do not consume their estimated average requirement for magnesium [96]. Therefore, it is not surprising that prescribing oral magnesium therapy can lower a high BP. However, this categorized review of clinical trials shows that medication status, hypertensive status, and magnesium dose all must be considered in the use of this inexpensive, non-invasive, safe, readily available, "lifestyle" therapy to prevent and treat high BP as well as other conditions for which high BP is a risk factor. Pervasive low dietary magnesium status affects the health and health care systems of national and global populations [39,97]. Chronic low dietary magnesium quite likely constitutes one of the "lifestyle" components in the high risk of cardiovascular disease of our time [39,98,99].
Conclusions
This categorization study shows that oral magnesium therapy added to treatment regimens of patients with partially controlled hypertension holds promise as a way of safely achieving lower BP without increasing antihypertensive medications. Prescribing magnesium supplements to hypertensive but untreated patients may not lower BP unless the daily magnesium dose meets or exceeds 600 mg/day, which can be safely and economically accomplished, but magnesium doses below this level can achieve other cardiovascular risk factor improvements without the side effects of antihypertensive medications [99].
VitaminDWiki - studies in both categories Magnesium and Hypertension
This list is automatically updated
{category}
VitaminDWiki - Magnesium and Vitamin D category contains
{include}
10 most-recently changed items in Magnesium Category
This list is automatically updated
{LISTPAGES}
Title change made June 2022 caused the visitor count to reset.
There have actually been visitors to this page since it was originally made