Magnesium Role in Health and Longevity - many studies
Chapter 9 in Trace Elements and Minerals in Health and Longevity - 2018
https://doi.org/10.1007/978-3-030-03742-0_9
Mario Barbagallo and Ligia J. Dominguez
Geriatric Unit, Department of Internal Medicine and Geriatrics,
University of Palermo, Via del Vespro 141, 90127 Palermo, Italy e-mail: mario.barbagatlo@unipa.it
J. Dominguez e-mail: ligia.dominguez@unipa.it
Abstract
Reduced Magnesium (Mg) intake is a frequent cause of Mg deficit with age. A decreased intestinal Mg absorption and an increased Mg loss may also contribute, as well as the use of medicaments. Furthermore, Mg requirements may be higher with aging. Alterations of Mg metabolism with age, cellular Mg transport systems and problems with measurement methods are discussed. Mg contained in water is more bio-available than Mg in food and it is a possible alternative to Mg supplementation in the correction of Mg deficiencies. Mild to moderate Mg deficits are generally asymptomatic and clinical signs are usually absent or non-specific. Hyperemotionality, tremor, asthenia, sleep disorders, and amnesic and cognitive disturbances are frequent in older adults, and may be often overlooked or confused with age-related symptoms. Chronic Mg deficiency results in oxidative stress and chronic, low-grade inflammation, which may be linked to several age-related diseases, and to the aging process itself. Mg deficit-related conditions may involve different tissues and organs, including hypertension and cardiovascular diseases, diabetes mellitus and metabolic syndrome, asthma and airways constrictive syndromes, depression and psychiatric disorders, Alzheimer’s disease and neuromuscular diseases (chronic fatigue, muscle pain, fibromyalgia), fragility fractures, and cancer. Keeping an optimal Mg balance throughout life might help to prevent some chronic disease associated to aging, and to extend healthy life. This needs to be proven by future studies.
📄 Download the PDF from Sci-Hub via VitaminDWiki
Chart: Low Mg ==> Inflamm-aging
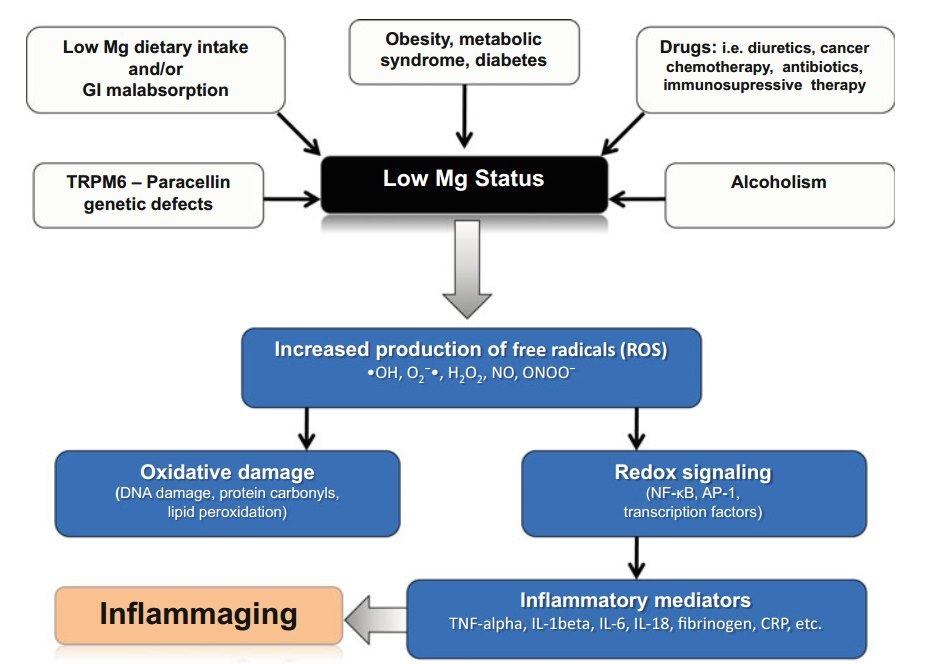
Chart: Low Mg ==> Aging

Introduction
Magnesium ion (Mg) is the second most abundant cation after potassium (K) in the intracellular compartment and the fourth most common mineral in the human body after calcium (Ca), sodium (Na) and K; Mg atomic weight is 24.305 g/mol, and its atomic number is 12 (Table 9.1). Mg is a member of Group IIA in the periodic table and thus an alkaline-earth element; it forms most stable complexes with phosphate and carboxylate anions or with nitrogen base. Mg is an essential cofactor for numerous biological processes, and it is required for energy production, oxidative phosphorylation, glycolysis, protein synthesis, and nucleic acid synthesis and stability (Saris et al. 2000). Mg plays a role in the active transport of other ions across cell membranes, such as Ca and K, modulating neuron excitability, muscle contraction, and normal heart rhythm. Mg has a key role in the adenosine triphosphate (ATP) synthesis in mitochondria, to create a complex with Mg (MgATP) (Barbagallo and Dominguez 2007). Cell signaling requires MgATP for protein phosphorylation and for the synthesis and activation of cell-signaling molecule cyclic adenosine monophosphate (cAMP) involved in a myriad of biochemical processes (Reinhart 1988).
Mg has critical role in modulating a wide variety of critical cellular activities and metabolic pathways. Mg is cofactor in over three hundred enzymatic reactions, and in particular is required for the activity of all rate-limiting glycolytic enzymes, protein kinases, and in all phosphorylation processes and in all reactions that involve ATP utilization and transfer (Barbagallo and Dominguez 2007). Mg has a weak calcium antagonist action and has many structural functions (multi-enzyme complexes, i.e., G-proteins, N-methyl-D-aspartic acid [NMDA] receptors, mitochondria, polyribosomes, proteins and nucleic acids synthesis, etc.).
Therefore, Mg is a critical factor for normal cellular and body homeostasis (Table 9.2). Over the past decades, the clinical relevance and biological significance of Mg have been documented, as well as the impact of Mg on molecular and physiological processes of aging, and on health and age-related clinical diseases.
Table 9.1 Characteristics of ionic magnesium
Table 9.2 Physiological roles of magnesium
Magnesium Metabolism and Requirement
In the human body, approximately 24 g (1 mol) of Mg are present, of which about 65% are stored in bone and 34% in the intracellular space. Less than 1% of total Mg is contained in blood serum; normal serum Mg concentrations range between 0.75 and 0.95 mmol/L (1.7-2.5 mg/dL or 1.5-1.9 meq/L). The levels of Mg in the plasma of healthy people are extremely constant and are tightly controlled and maintained within this narrow range by the small intestine and the kidney; both increase their fractional Mg absorption under conditions of Mg deprivation. If Mg depletion continues, the bone store helps to maintain serum Mg concentration by exchanging part of its content with extracellular fluid (Fig. 9.1) (Barbagallo et al. 2003).
In the serum, Mg exists in three forms: a protein-bound fraction (25% bound to albumin and 8% bound to globulins), a chelated fraction (12%), and the metabolically active ionized fraction (Mg-ion: 55%). Hypomagnesemia is defined as a serum Mg level less than 0.75 mmol/L (Barbagallo et al. 2003). Intracellular Mg concentrations are highly regulated and Mg itself acts as an intracellular regulator of cell cycle control and apoptosis. Intracellular Mg exists mainly in a bound form. Plasma Mg levels do not always reflect intracellular or total Mg.
Mg balance is controlled by Mg intake, by its absorption through intestine, by the renal excretion, and by the Mg requirement of different tissues (e.g., skeletal and cardiac muscle uptake and usage) (Quamme 2008). Daily Mg requirement is calculated to be around 300-400 mg in healthy adults (5-6 mg/kg/day) but may be
Fig. 9.1 Magnesium homeostasis and age (arrows indicate possible sites of alterations with aging)
Table 9.3 Determinants of magnesium equilibrium
Gastrointestinal absorption and renal excretion are the main determinants of Mg equilibrium
Healthy individuals need to consume 0.2-0.4 mmol/kg of body weight/day to stay in balance
Extracellular Mg is in equilibrium with that in the bone, kidneys, intestine, and other soft tissues
Bone is the main reservoir of Mg
Primary renal disorders cause hypomagnesemia by decreased tubular reabsorption of Mg
Osmotic diuresis results in magnesium loss
Drugs may cause magnesium wasting
higher in several physiological conditions (i.e. pregnancy, aging, exercise, etc.) and diseases (type 2 diabetes, infections, etc.).
The main site for Mg absorption is the small intestine. Healthy persons need to consume 0.2-0.4 mmol/kg/day to maintain the balance (Table 9.3). Since the Mg stored in the bone cannot quickly exchange with the Mg in extracellular fluids, the quick Mg needs are provided by the Mg stored in the intracellular compartment. Kidney also has a key role in Mg homeostasis and about 120 mg of Mg are excreted into the urine each day (Saris et al. 2000). Renal Mg handling is tightly dependent on Mg body status, since Mg deficiency increases renal Mg reabsorption across all nephron segments. In fact, urinary excretion is reduced when Mg is depleted (Shils 1969). Diuretic drugs may also modify renal Mg handling by reducing Mg reabsorption (Quamme 1997).
Although no known hormonal factor is specifically involved in the regulation of Mg metabolism, many hormones are recognized to have an effect on Mg balance and transport. Among them, parathyroid hormone (PTH), calcitonin, catecholamines, and insulin have a major role (Barbagallo et al. 2003, 2007).
Magnesium Measurements Methods
Measurements of total serum Mg concentrations (MgT) are not an accurate measure of the body Mg status; MgT measurements are useful in epidemiological studies, but do not detect subclinical Mg deficit in an individual basis (Elin 2010). Others, more precise and expensive techniques, such as 31P-NMR spectroscopy, still remain mainly a research tool. The development of Mg-specific ion-selective electrodes, that measure the active ionized fraction of Mg, has been more appropriate, allowing measuring extracellular free levels of Mg with a higher sensitivity than MgT in order to detect subclinical Mg deficits in several medical conditions (Barbagallo et al. 2014; Resnick et al. 1997).
Cellular Magnesium Transport System
Transient receptor potential (TRP) is a family of protein containing both, a cationpermeable ion channel and a kinase domain (Clapham et al. 2001). TRPM7 is a divalent cation-selective ion channel that is permeable to Ca2+ and Mg2+. The channel is downregulated by intracellular levels of Mg2+, MgATP, and other Mg-nucleotides (Penner and Fleig 2007). The channel plays a key role in Mg homeostasis due to its preference for divalent ions (Romani 2011). TRPM7 represents a ubiquitous homeostatic mechanism that regulates Ca2+ and Mg2+ fluxes. Reducing the cellular levels of Mg stimulates the activation of TRPM7-mediated currents (Faouzi et al. 2017).
Magnesium Deficiency with Aging: Causes and Mechanisms
Mg deficits are common in old age (Barbagallo and Dominguez 2010). Total plasma Mg concentrations do not change with age (Yang et al. 1990). Differences in Mg levels are generally related to the presence of age-related diseases and alterations in renal function. Studies using 24-h Mg retention showed an increased Mg retention in old age, suggesting a significant subclinical Mg deficit, not detected by total serum Mg (Gullestad et al. 1994). In healthy persons, we showed that intracellular free
Table 9.4 Main mechanisms of magnesium deficit with aging Primary Mg deficit
Inadequate Mg dietary intake
Reduced efficiency of Mg absorption (associated with reduced vitamin D levels)?
Increased urinary excretion of Mg (Mg) (associated with age-dependent reduction of kidney function and of Mg tubular reabsorption)
Secondary Mg deficiency
Associated with age-related diseases and comorbidities
Increased urinary Mg loss secondary to drugs (i.e. diuretics) frequently used in the older persons
Mg decreases with age;
we have specifically studied the behavior of intracellular Mg content with age, using the gold standard method (31P-NMR spectroscopy) in healthy young and older persons and have shown a continuous age-dependent fall of intracellular Mg levels in red blood cells of healthy older adults (Barbagallo et al. 2000), while total serum Mg was not significantly altered with age. It has been shown that many older adults are prone to chronic latent Mg deficiency (Table 9.4), and epidemiological data from US and Europe have confirmed that low Mg intake is a common condition in older persons (Ford and Mokdad 2003; Galan et al. 1997).
However, it has been suggested that Mg requirement do not change with age (Hunt and Johnson 2006). Data from the National Health and Nutrition Examination Survey (NHANES) III showed that Mg intake tend to decrease with age (Ford and Mokdad 2003). In addition, older adults affected by chronic conditions and on chronic drug treatment have an additional risk of being Mg deficient. The recommended Mg intake in the US population is 420 and 320 mg/day for men and women, respectively, but Mg intake in the US older population is far below (225 and 166 mg/day for men and women, respectively) (Table 9.5) (Ford and Mokdad 2003). Sixty eight per cent of US adults consume less than the recommended daily allowance (RDA) of Mg, Forty- five per cent consume less than 75% of the RDA, and nineteen per cent consume less than 50% of the RDA (King et al. 2005). The “Suppléments en Vitamines et Minéraux AntioXydants” (SU.VI.MAX) study showed that seventy-seven per cent of women and seventy-two per cent of men have dietary Mg intakes lower than RDA; twenty three per cent of women and eighteen per cent of men consumed less than 2/3 of these RDA (Galan et al. 1997).
Decreased intestinal Mg absorption may further contribute to Mg deficiency in the elderly (Coudray et al. 2006). Mg absorption tends to decrease with age. Duodenum and ileum are mainly involved in Mg absorption and both passive and active transport processes are involved. The alterations of the intestinal absorption of Mg in old age may be also aggravated by the frequent age-related impairment of vitamin D homeostasis. Kidney active reabsorption of Mg takes place in the loop of Henle and in the proximal convoluted tubule. A latent primary renal disorder may also be associated to an increased Mg loss linked to a reduced tubular reabsorption.
Table 9.5 Recommended dietary allowance (RDA) for magnesium (AI: adequate intake when RDA cannot be determined)
Secondary Mg deficiencies may also be associated with drug use or with pathological conditions (i.e., type 2 diabetes mellitus, insulin resistance, alcoholism, hyperadrenoglucocorticism, HIV/AIDS, acute myocardial infarction, stroke, etc.). Mg depletion due to an excess urinary loss may be related to treatment with loop diuretics. Patients receiving long-term treatment with thiazide diuretics are also at risk, especially in old age. Hypokalemia is often associated with diuretic-induced Mg depletion. It has been reported the finding of hypomagnesemia in 38-42% of hypokalemic patients. The correction of a K deficit may be difficult to achieve unless the Mg deficit is also corrected, hence patients with hypokalemia should be evaluated for Mg deficiency. Other commonly used medications may diminish Mg absorption and/or reduce Mg levels (e.g., H2 blockers, proton pump inhibitors, antacids, antibiotics, antihistamines, antivirals, and antiepileptic drugs, among others).
Western diets, generally very low in whole grains and green vegetables, and high in refined foods, are often severely deficient in Mg (Table 9.6). Food processing may significantly lower Mg content. Because most of the Mg present in food is lost in cooking or refining procedures, diets that provide a high proportion of daily calorie requirements from refined or processed foods are likely to be low in Mg (Durlach et al. 1985). Cooking, especially boiling of foods may cause a significant loss of Mg. Processed food accounts for a substantial portion of the diet in western countries, which makes more probable the establishment of a state of true or relative Mg deficiency (Barbagallo and Dominguez 2010). Furthermore, phytic acid found in certain foods lowers the absorption of Mg. Some pesticide agents, commonly used in the crops, such as glyphosate, may chelate minerals including Mg (Cakmak et al. 2009), further decreasing the content of Mg in soil and in some crops. Organic food,
Table 9.6 Some food sources of magnesium
from pesticide-free soils, was found to have significantly more Mg than non-organic control food (Griffiths et al. 2012).
Because of this substandard dietary content of Mg in developed countries, Mg intake is often significantly reduced. In this context, Mg intake derived from drinking water rich in Mg may represent a possible alternative to supplements in Mg deficits (Galan et al. 2002).
In the SU.VI.MAX cohort, drinking water contributed 6-17% of total daily Mg intake depending on the Mg concentration of the mineral water used. Drinkers of mineral water rich in Mg and water with a moderate mineral content had Mg intakes significantly higher than those of drinkers on low mineralized or tap water. Therefore, mineral-rich water may provide an important supplementary contribution to total Mg intake (Galan et al. 2002). In addition, bio-availability of Mg in water is higher when compared to Mg in food and it is easy to add Mg to water, but virtually impossible to add Mg to foods. Mg content may be important not only in drinking water, but also in water used for cooking, since the concentration of Mg in water may interfere with the leakage of Mg in food during cooking, and may reduce the loss of Mg in the cooked/boiled food.
Magnesium, Inflammation and Oxidative Stress
Hypomagnesaemia has been shown to cause increased production of oxygen free radicals. Poor Mg diets are associated with a low-grade chronic inflammatory state, both, by initiating an excessive production and release of interleukin (IL)-tp and tumor necrosis factor (TNF)-alfa, and by stimulating the synthesis of nitric oxide and some inflammatory markers (Kramer et al. 2003; Mazur et al. 2007). Mg deficiency also increases the aggregation and adhesiveness of platelets, and inhibits growth and migration of endothelial cell, potentially modulating microvascular functions (Mazur et al. 2007).
In animals, several studies have shown that Mg deprivation causes: (i) marked elevation of proinflammatory molecules TNF-alfa, IL-1-beta, IL-6, vascular cell adhesion molecule (VCAM)-1, and plasminogen activator inhibitor (PAI)-1 (Malpuech- Brugere et al. 2000; Mazur et al. 2007); (ii) increased circulating inflammatory cells (Galland 1988), and (iii) increased hepatic production and release of acute phase proteins (i.e., complement, alfa2-macroblobulin, fibrinogen) (Bussiere et al. 2003; Mazur et al. 2007).
In humans, clinical data have shown that low serum Mg levels as well as inadequate dietary Mg are strongly related to low-grade systemic inflammation (King et al. 2005; Guerrero-Romero et al. 2011; Song et al. 2007). Several other studies have confirmed an inverse relationship among Mg intake, serum Mg and inflammation markers. Data from the Women’s Health Study have shown that Mg intake is inversely related to systemic inflammation, measured by serum C-reactive protein (CRP) concentrations, and with the prevalence of the metabolic syndrome in adult women (Song et al. 2005). Using the 1999-2002 NHANES databases, King et al. found that dietary Mg intake was inversely related to CRP levels. Among 70% of the population not taking supplements, Mg intake below the RDA was significantly associated with a higher risk of having elevated CRP (King et al. 2005).
Mg deficiency has been associated with increased oxidative stress and decreased antioxidant defense competence. Previous studies have shown compellingly that Mg deficiency results in an increased production of oxygen-derived free radicals in various tissues, increased free radical-elicited oxidative tissue damage, increased production of superoxide anion by inflammatory cells, decreased antioxidant enzyme expression and activity, decreased cellular and tissue antioxidant levels, and increased oxygen peroxide production (Weglicki et al. 1996; Mazur et al. 2007)
In rats, Mg deficiency has been shown to increase lipid peroxidation and malon- dialdehyde and to decrease hepatic glutathione, superoxide dismutase, and vitamin E (Calviello et al. 1994). We have suggested a link between the action of Mg in altering the antioxidant capacity and in activating oxidative stress, inflammation, and lipid oxidation with insulin resistance, diabetes, and cardio-metabolic syndrome (Barbagallo and Dominguez 2007).
Aging is characterized by a chronic, low-grade inflammatory state that involves several tissues and organs, and that has been named “inflammaging” (Franceschi et al. 2017).
We have suggested that the Mg deficiency through its role in facilitating an impairment of the redox status and a low-grade inflammation may be a link to several age-related diseases and/or to accelerated aging (Fig. 9.2) (Barbagallo et al. 2009; Barbagallo and Dominguez 2010). Mg itself possesses antioxidant properties scavenging oxygen radicals possibly by affecting the rate of spontaneous dismutation of the superoxide ion (Weglicki et al. 1992).
Mg and the Immune Responses
There is evidence that Mg may play a role in the immune response as a cofactor for immunoglobulin (Ig) synthesis, C3 convertase, immune cell adherence, antibody-dependent cytolysis, IgM lymphocyte binding, macrophage response to lymphokines, and T helper- cell adherence (Tam et al. 2003; Galland 1988). In addition, Mg deficiency seems to accelerate thymus involution. One of the most remarkable results regarding effects of Mg deficiency on the organism is the higher level of apoptosis shown in thymuses from Mg-deficient rats as compared with controls (Malpuech-Brugere et al. 1999). Mg-deficient diet has been shown to alter polymorphonuclear cell number and function, together with an increased number of neutrophils, related to an increased activity of phagocytosis (Bussiere et al. 2003). Mg is also involved in human cell apoptosis. Fas-induced P-cell apoptosis is Mg- dependent. Elevation of intracellular free Mg levels is needed for Fas molecule binding expression on the P-cell surface to trigger signaling pathways that cause apoptosis and cellular death (Chien et al. 1999).
Magnesium Deficits and Aging Related Diseases
Clinical Signs and Symptoms
Severe Mg deficit may be associated with neuromuscular symptoms, such as weakness, tremor, muscle fasciculation, dysphagia, positive Chvostek’s sign (facial twitching as a reaction to the tapping of the facial nerve), and positive Trousseau’s sign (spasm of muscles of the hand and forearm following the application of a pressure cuff, transiently occluding the brachial artery). Neurologic disturbances may involve both, the sympathetic and parasympathetic nervous systems, causing orthostatic hypotension or borderline hypertension.
Mild to moderate Mg deficits are generally asymptomatic and clinical signs are usually absent and/or non-specific. Subjective symptomatology may include nonspecific manifestations, such as anxiety, hyperemotionality, fatigue, depressive symptoms to major depression, headache, insomnia, light-headedness, dizziness, and nervous fits. Peripheral signs are commonly present such as myalgias, acroparesthesias, and cramps. Functional complains may be present and are non-specific and may include chest pain, sine materia dyspnea, precordialgia, palpitations, extrasystoles and other arrhythmias, etc. Hyperemotionality, tremor, asthenia, sleep disorders and amnesic and cognitive disturbances are particularly important in elderly patients, and may be often overlooked or confused with age-related symptoms.
Elin suggested to name this common condition of persons with mild, chronic, negative Mg balance, associated with a non-specific symptomatology, as a syndrome of “Chronic Latent Magnesium Deficiency” (CLMD) (Elin 2010). Persons affected of CLMD have a total serum Mg concentration still within the lower part of the reference interval (latent), and from a clinical standpoint are generally undiagnosed being considered as having normal Mg status.
However, a chronic low Mg status has been associated with numerous pathological conditions characterized by a chronic inflammatory stress component. In humans, Mg deficiency through exacerbating chronic inflammatory stress may contribute significantly to the occurrence of several chronic age-related diseases.
Magnesium, Hypertension and Cardiovascular Diseases
Chronic Mg deficits have been linked to an increased risk of numerous preclinical and clinical cardiovascular outcomes, mostly observed in older populations, including hypertension, ischemic heart disease, cardiac failure and cardiovascular mortality, stroke, cardiac arrhythmias, atherosclerosis, endothelial dysfunction, alterations in lipid metabolism, platelet aggregation/thrombosis, inflammation, oxidative stress (Paolisso and Barbagallo 1997; Barbagallo et al. 2007).
Kobayashi in 1957 first noted that the nature of drinking water might influence death rates from cardiovascular disease; the incidence of stroke was significantly lower in areas with hard water (mainly linked to Mg and calcium content) (Kobayashi 1957). Schroeder surveyed the hardness of drinking water in the US, analyzing the relationship between the death rates and the water hardness found that death rates from cardiovascular diseases (particularly from coronary heart attacks in white men 45-64 years old) was significantly higher in states with soft water than in states with hard water (Schroeder 1966).
Mg has a crucial role in cardiovascular homeostasis. Although not directly involved in the biochemical process of contraction, Mg modulates vascular smooth muscle tone and contractility by affecting calcium ion concentrations and its availability at critical sites (Altura and Altura 1981; Altura et al. 1984). Consistent with the above, not only calcium-induced contraction in vascular smooth muscle is sensitive to changes in Mg concentration, but direct reduction of extracellular Mg raises smooth muscle Ca content, while conversely, elevations in Mg concentrations reciprocally lower calcium content in smooth muscle (Turlapaty and Altura 1980). Moreover, Mg directly affect uptake, distribution, and content of calcium in vascular smooth muscle cells, and can itself function as a nature’s weak physiologic calcium channel blocker (Iseri and French 1984), modulating calcium-channel activity in heart cells (Agus et al. 1989). In view of such direct and indirect actions of Mg on cardiac and vascular smooth muscle cells, it is reasonable to suggest that Mg deficiency might be relevant to disorders of blood pressure homeostasis, such as hypertension. Indeed, vascular hyperreactivity and frank hypertension can be induced by depleting of Mg both the in vitro environment, or in the organism as a whole (Altura and Altura 1991). Measurements of serum Mg levels are not useful, since no distinct alterations of circulating total Mg levels have been identified in essential hypertension. However, several abnormalities of Mg metabolism have long been recognized in hypertensive subjects. Epidemiologic studies have suggested an inverse relationship between Mg dietary intake and hypertension, lower dietary Mg intake being associated with higher blood pressure (Joffres et al. 1987). In aging populations, a gradual rise in blood pressure, a gradual fall in total serum Mg levels with age (Petersen et al. 1977), and an age-related suppression of intracellular free Mg (Barbagallo et al. 2000) have been observed, suggesting a possible role for Mg deficit in hypertensive states. Fasting levels of intracellular free Mg were found significantly suppressed in hypertensive patients as compared with normotensive controls (Resnick et al. 1984). Moreover, in different experimental rat models of hypertension, diets that raised or lowered intracellular free Mg, consistently lowered and raised blood pressure, respectively. Abnormalities of Mg urinary excretion in hypertensive experimental models have also been described (Barbagallo et al. 1992). Similarly, the ability of a high salt diet to elevate blood pressure was shown to be related to intracellular free Mg in humans (Resnick et al. 1994).
Mg was first recommended to lower blood pressure in patients with malignant hypertension as early as 1925 (Blackfan and Hamilton 1925). Therapeutical use of Mg has consistently been found beneficial in preeclampsia and eclampsia (Chien et al. 1996) and in patients with malignant hypertension (Winkler et al. 1942), while the response to Mg in essential hypertensives is heterogeneous (Resnick and Laragh 1985). In some studies, Mg supplementation may have significant hypotensive effects, while in others blood pressure may not change or may worsen. A Cochrane review suggested that there was not yet enough information to suggest the use of Mg in hypertension despite a small statistical reduction in diastolic blood pressure (Dickinson et al. 2006). Thus, even if a role for decreased Mg levels in the pathophysiology of hypertension appears likely, a consistent, reproducible effect of Mg supplementation on blood pressure has not yet been confirmed in hypertension and further data are needed to consider Mg as a non-pharmacological tool for treating hypertension. Among the reasons for this are the virtual absence of adequately designed clinical trials of Mg therapy in hypertension, the differing treatment schedules used in a number of smaller clinical reports, and a failure to appreciate the heterogeneity of the underlying mechanisms contributing to hypertension. Thus, long-term prospective therapeutic trials of Mg in hypertension are clearly needed in the near future.
Mg deficiency may also have a role in the development of atherosclerosis. Contrasting results have been reported on the relationship between serum lipids and total and ionized serum Mg concentrations. Serum Mg has been found to be positively (Randell et al. 2008) or negatively (Corsonello et al. 2007) associated with serum lipid levels. Binding interactions between Mg and lipoproteins may, at least partially, account for these contrasting results, although it is also possible that the relationship between Mg status and lipids in healthy persons may be different from that in patients with chronic conditions, such as obesity, diabetes, and hypertension (Corsonello et al. 2007). Low Mg status has been suggested to contribute to vascular calcification, altered lipid accumulation, and reduced cholesterol transport by high density lipoprotein (HDL) (Rayssiguier 1984). Mg has been suggested to have role in preventing atherosclerotic plaque formation, and to have a positive effect on metabolic lipid profiles.
Rosanoff and Seelig proposed that Mg may act as a weak inhibitor and a modulator of 3-hydroxy-3-methylglutaryl-CoA-reductase activity. Mg is also essential for the activity of other enzymes of the lipid metabolism such as lecithin cholesterol acyl transferase (LCAT), which regulates low density lipoprotein-cholesterol, HDL-cholesterol, and triglyceride levels, and thus may modestly help to raise HDL- cholesterol and lower triglycerides (Rosanoff and Seelig 2004).
Mg may be beneficial as a support in the treatment of atrial and/or ventricular arrhythmias, in particular when there is co-existent hypokalemia (McLean 1994). Indeed, Mg plays a role in the heart’s electrical conduction and Mg deficiencies have been linked to many cardiovascular conditions. Mg deprivation has been suggested to compromise cardiovascular health and favor the occurrence of heart arrhythmias. Hypomagnesemia is relatively common in patients presenting with atrial fibrillation (AF) (Singh et al. 1976) and low serumMg was suggested to be moderately associated with the development of AF (Khan et al. 2013).
Dietary Mg restriction to about one third (33%) of the RDA induced heart rhythm changes including AF and flutter that responded quickly to Mg supplementation (Nielsen et al. 2007). A meta-analysis conducted in Canada has suggested that intravenous Mg administration is an effective and safe strategy for the acute management of AF. An overall favorable response was achieved in 86 and 56% of patients in the Mg and control groups, respectively (OR 4.61; 95% CI 2.67-7.96) (Onalan et al. 2007). Intravenous administration has been proposed as a very effective and safe treatment for torsade de pointes, because its application is rapid and simple (Tzivoni et al. 1988; Gupta et al. 2007).
Major cardiac effects of Mg are prolongation of atrial and atrioventricular nodal refractory periods, which may facilitate rate and rhythm control in AF (DiCarlo et al. 1986). These antiarrhythmic actions of Mg may, at least in part, help to explain the possibility that a high Mg dietary intake may reduce the risk of sudden death. Women in the highest quartile of Mg intake were found to have a reduced risk of sudden cardiac death (Chiuve et al. 2013).
In patients with severe congestive heart failure (New York Heart Association functional classification IV), under optimal medical cardiovascular treatment, oral Mg supplementation improved clinical symptoms and survival outcomes as compared to placebo (Stepura and Martynow 2009).
Magnesium and Type 2 Diabetes
The link between Mg deficiency and type 2 diabetes mellitus (DM2) is well known. DM2 is frequently associated with both extracellular and intracellular Mg depletion, in particular in those patients with poorly controlled glycemic profiles, with longer duration of the disease, and with the presence of micro- and macrovascular chronic complications (Mather and Levin 1979; Schnack et al. 1992; Barbagallo and Dominguez 2007, 2015). Depletion in intracellular and/or ionized plasma Mg can be found in individuals with normal total serum Mg (Resnick et al. 1993; Barbagallo et al. 2014). Among the mechanisms that may favor Mg depletion in diabetes, the most important are a low Mg dietary intake and an increased Mg urinary loss, while absorption and retention of dietary Mg seems to be unchanged in patients with DM2 (Walti et al. 2003). An inverse association between dietary Mg and the incidence of DM2 has been reported. A diet deficient in Mg is associated with a significant impairment of insulin-mediated glucose uptake and with a considerable increased risk of developing glucose intolerance and diabetes (Barbagallo and Dominguez 2007). Mg depletion in DM2 is associated with renal Mg and calcium wasting. Hyperglycemia and hyperinsulinemia may both have a role in the increased urinary Mg excretion contributing to Mg depletion (McNair et al. 1982). Hyperglycemia, which is a hallmark of lack of good metabolic control, may have a role in urinary Mg wasting. Hyperinsulinemia, present in insulin resistant states, may contribute per se to the urinary Mg depletion and the reduced insulin sensitivity, and may itself affects Mg transport (Djurhuus et al. 1995). Lower Mg levels may not only be a consequence, but may also predispose to the development of DM2.
Mg deficits have been associated with an increased risk for the development of glucose intolerance, cardiometabolic syndrome, and DM2 (He et al. 2006; Lopez- Ridaura et al. 2004; Song et al. 2004). Intracellular Mg depletion, causing a defective activity of the tyrosine kinase insulin receptor, as well as other Mg-dependent kinases of the insulin signaling, impairs insulin sensitivity and may contribute to the development of clinical conditions associated with insulin resistance, such as glucose intolerance and DM2. Inflammation and oxidative stress have been proposed as additional mechanisms by which Mg is linked to insulin resistance/metabolic syndrome. More generally, chronic hypomagnesemia and conditions commonly associated with Mg deficiency, such as DM2 and aging, are all associated with an increase in free radical formation with subsequent damage to cellular processes (Barbagallo and Dominguez 2007). The hypothesis that a dietary Mg deficit would induce and/or exacerbate insulin resistance is confirmed by data, both in experimental animals and in humans, showing that dietary-induced Mg deficiency is associated with insulin resistance (Schnack et al. 1992). A Mg-deficient diet in sheep caused a significant impairment of insulin-mediated glucose uptake (Matsunobu et al. 1990), while Mg supplementation delayed the development of diabetes in a rat model of diabetes (Balon et al. 1995). Higher Mg intake is associated with lower fasting insulin concentrations among women without diabetes (Fung et al. 2003), and a significant negative correlation is present between total dietary Mg intake and the insulin responses to an oral glucose tolerance test (Humphries et al. 1999). The increased risk for developing glucose intolerance and DM2 in persons with dietary and/or serum Mg deficits have suggested potential benefits of Mg supplementation in persons with DM2 or with risk factors for diabetes. The use of Mg supplements has been proposed as a potential tool for the prevention and the metabolic control of DM2. Benefits of Mg supplements on glycemic profile in most, but not all, studies does not explain whether according to meta-analysis a net beneficial effect is to be expected. While the body of evidence from epidemiological studies consistently shows a strong inverse relationship between dietary Mg intake and the risk of developing DM2, research concerning Mg supplementation in people with or at risk of diabetes is limited (Rodriguez-Moran et al. 2011; Von Ehrlich et al. 2014). A recent systematic review and meta-analysis including eighteen double-blind randomized controlled trials (12 in people with diabetes and 6 in people at high risk of diabetes) showed that Mg supplementation appears to have a beneficial role improving glucose parameters in people with DM2 and also improving insulin-sensitivity parameters in those at high risk of diabetes (Veronese et al. 2016).
Magnesium in Asthma and Airway Constriction
The first suggestion of a role for Mg in asthma was proposed in 1940 by an anecdotal report of Haury in two hospitalized patients having acute exacerbations of asthma who had a favorable clinical response after intravenous Mg sulfate administration. Haury reported that both patients were relieved immediately and remained free from symptoms for eighteen and twenty-four hours, respectively (Haury 1940).
Afterwards, the possible role of Mg in the pathogenesis of bronchial constriction as well as in its treatment regained considerable attention, particularly because of several reports confirming positive results of Mg administration in acute airway constriction (Okayama et al. 1987; Bloch et al. 1995) although some studies reported negative results (Tiffany et al. 1993; Bernstein et al. 1995). Even in the absence of an acute exacerbation, the functional pulmonary tests have been shown to improve with the administration of intravenous Mg and the action of Mg appears to be additive to the bronchodilating effect of the anti-asthmatic medicaments terbutaline (Skorodin et al. 1994) and salbutamol (Rolla et al. 1994).
Mg has modulatory effects on the contractile state of smooth muscle cells in various tissues: hypomagnesemia leads to contraction and hypermagnesemia leads to relaxation. Potential mechanisms for the direct relaxing effects of Mg on bronchial smooth muscle include calcium channel blocking properties (Iseri and French 1984), inhibition of cholinergic neuromuscular transmission with decreased sensibility to the depolarizing action of acetylcholine (McLean 1994), stabilization of mast cells and T-lymphocytes (Chyrek-Borowska et al. 1978), and stimulation of nitric oxide (Kemp et al. 1994) and prostacyclin (Nadler et al. 1987). In accordance with this hypothesis, Britton et al. showed that dietary Mg intake was independently related to lung function and to the occurrence of airway hyperreactivity, suggesting that a low Mg intake may be involved in the etiology of asthma (Britton et al. 1994). Significant positive independent associations of dietary Mg intake and lung function, airway reactivity to inhaled methacholine, and respiratory symptoms (wheezing) in the general population were reported (Britton et al. 1994).
Serum Mg measurements are not clinically useful for predicting the severity of the asthmatic attack, nor are they predictive of the response to Mg infusion, and no differences were present in serum Mg in asthmatic patients during acute exacerbation compared to a non-asthmatic population (Falkner et al. 1992). Conversely, cellular skeletal muscle Mg was found to be lower in the asthmatic patients when compared to non-asthmatic controls (Gustafson et al. 1996). We have shown a strong and direct relationship between the intracellular Mg levels and the methacholine bronchial reactivity in asthmatic patients suggesting a key role of intracellular Mg alterations and favorable effects of Mg administration in these patients (Dominguez et al. 1998).
Altogether the data are in agreement for a role of a deficit in cellular and body Mg as a relevant contributor to an increased reactivity and contractility of smooth muscle in the vascular and bronchial tissues, causing both vasoconstriction and bron- choconstriction (Seelig 1994).
Magnesium, Depression, Other Psychiatric Disorders, and Neuromuscular Symptoms
Mg deficits have been associated with numerous acute and/or chronic psychiatric disorders including depression, hypochondriasis, generalized anxiety, behavioral alterations, panic attacks, hyperexcitability, cephalalgias, as well as focal seizures, ataxia, anxiety, dizziness, tremor, irritability, insomnia, and psychotic behavior. Neuromuscular symptoms may include age-related muscular weakness, asthenia and myalgias (e.g., fibromyalgia and chronic fatigue syndrome). These conditions are generally, at least in part, reversible (Durlach et al. 2000).
As regards the central nervous system, Mg deprivation has been suggested to cause electrophysiological signs of hyperexcitability. In Mg deficient rats, changes in the electroencephalogram (EEG) were studied during auditory stimulation and correlated with behavioral alterations. The EEGs showed consistent changes with spike activity, initiating in the hippocampus and then spreading to the neocortices bilaterally, suggesting that behavioral changes induced by auditory stimulation in Mg-deficient rats are due to a Mg-related increased excitability of the central nervous system, resulting in seizures in deeper brain structures, particularly in the limbic system, later developing secondary generalization and projecting secondarily to the neocortices (Goto et al. 1993).
In humans, many characteristic signs and symptoms of Mg deficiency have been associated with neural and neuromuscular hyperexcitability (Galland 1991). Durlach have reviewed a number of possible mechanisms of Mg deficiency, which may induce depolarization and mediate central nervous hyperexcitability (Durlach et al. 2000). These include the previously described effects of Mg affecting cellular calcium homeostasis, increased susceptibility to peroxidation, increased activity of excitatory neurotransmitters, such as acetylcholine, catecholamines, N-methyl-D-aspartate (NMDA) and non-NMDA receptors of excitatory aminoacids, decreased activity of inhibitory neurotransmitters, such as gamma-aminobutyric acid (GABA), taurine, glutaurine, adenosine and K receptors of opioids. Systemic effects that may also be involved include increased production of inflammatory mediators: neuropeptides, prostanoids, cytokines and decreased activity of anti-oxidant defenses.
Because of these important connections with the biological and transduction pathways implicated in the pathophysiology of depression, and in particular its role on the ion channel of the NMDA-receptor complex that is subject to voltage-dependent regulation by Mg ions (Decollogne et al. 1997), Mg supplementation has been suggested to be useful for the treatment of depression (Eby and Eby 2010; Derom et al. 2013). No significant correlation between total plasma Mg levels, severity of depression, and anxiety were observed (Barra et al. 2007; Kirov et al. 1994), although antidepressant drugs sertraline and amitriptyline have been shown to increase intracellular Mg levels (Nechifor 2009).
A systematic review including twenty-one cross-sectional studies, three intervention trials, one prospective study, one case only study, and one case series study, concluded that a higher intake of dietary Mg was associated with lower depression symptoms (Derom et al. 2013).
Mg appears to be effective to some extent in the treatment of depression but data are scarce and incongruous. Oral Mg supplementation may help in the prevention of depression and might be used as an adjunctive therapy. However, more interventional and prospective studies are needed in order to further evaluate the benefits of Mg supplementation for the treatment of depression.
Mg has also been used as an adjuvant in the treatment of insomnia. Thus, Mg as a natural NMDA antagonist and a GABA agonist, may have a relaxant effect, may increasing melatonin levels, and may facilitate sleeping well (Abbasi et al. 2012).
Mg and Alzheimer’s Disease
The role of Mg in dementia and other degenerative disorders has been the focus of increased attention (Glick 1990). Some epidemiological, experimental and clinical data have linked Mg depletion to dementia and Alzheimer’s disease (AD) although the mechanisms of this association have not been clearly defined yet. Mg insufficiency and its altered concentrations in the brain, as well as the effects of Mg supplementation in AD, have been investigated. Total serum Mg levels, ionized plasma Mg levels, and Mg content in various tissues of patients with Alzheimer’s disease in clinical, experimental and autopsy studies have consistently shown to be reduced (Vural et al. 2010; Cilliler et al. 2007; Barbagallo et al. 2011; Andrasi et al. 2005). Mg concentration affects multiple biochemical mechanisms in the brain, which are involved in the cognitive process, including NMDA-receptor response to excitatory amino acids, cell membrane fluidity and stability, and toxic effects of calcium (Barbagallo and Dominguez 2010). In addition, high intake of a neurotoxic metal, such as aluminum, which inhibits activity of Mg-requiring enzymes, impairs transport of Mg and/or enhances transport of the neurotoxic metal into brain tissue, has been hypothesized to have a role to alter incorporation of Mg into brain neurons (Glick 1990).
Magnesium and Bone Disease
Mg deficiency has been proposed as a potential risk factor for developing osteoporosis and fragility fractures. Insufficient dietary Mg intake has been associated in humans with low bone mass and postmenopausal osteoporosis. Epidemiologic studies have demonstrated a positive significant correlation between dietary Mg intake and bone density and/or an increased rate of bone loss with low dietary Mg intake (Tucker et al. 1999; New et al. 2000). In two thousand thirty-eight older black and white men and women aged 70-79 at baseline enrolled in the Health, Aging and Body Composition Study, higher Mg intake, assessed using a semiquantitative food frequency questionnaire, was found to be associated with higher bone mineral density in healthy older white (but not in black) participants (Ryder et al. 2005). The effect of selective dietary Mg depletion has been extensively studied in experimental rat model. Preclinical studies have shown that Mg-depleted mice with frank hypomagnesemia had impaired bone growth, decreased bone formation, increased bone resorption, osteoporosis, and increased skeletal fragility (Kenney et al. 1994; Rude etal. 1999).
The pathophysiologic basis for this effect of Mg on bone, however, remains unknown, although elevated serum concentrations of inflammatory cytokines may play a role. The possible role of Mg deficiency in determining bone loss is confirmed by data from Rude and Gruber showing an increased osteoclastic bone resorption associated with an increased concentration of substance P and TNF-alfa in bone from Mg-deficient rats (Rude and Gruber 2004).
Mg is required for activation of vitamin D and Mg deprivation is associated with hypoparathyroidism, low production of 1,25-OH2 D3, and resistance to PTH and vitamin D actions (Medalle et al. 1976). The combined effects of Mg deficiency and low PTH and 1,25-OH2 D3 synthesis and secretion may also contribute to impair bone growth and mineralization and to reduce bone quality, strength, and bone mineral density. Oral Mg supplementation suppresses bone turnover and may help to prevent osteoporotic disease (Aydin et al. 2010; Dimai et al. 1998).
A recent report in a large cohort of American men and women involved in the Osteoarthritis Initiative followed over a period of 8 years showed that women meeting the recommended Mg intake were at a 27% lower risk for future fractures, suggesting a protective effect of Mg on the risk of incident fragility fractures (Veronese et al. 2017).
Mg and Muscular Disease (Chronic Fatigue, Muscle Pain, and Fibromyalgia)
Muscle pain may be associated with Mg deficiency. The original symptoms, which may have been due to Mg deficiency, include weakness and night cramps. Fibromyalgia is a rheumatic disease characterized by muscular pain and tenderness associated with a non-specific general symptomatology that includes fatigue, sleep disorders, bowel dysfunction, and headache, among others. The etiology is still unknown, although it has been suggested that deficiency in trace elements may contribute to the development of fibromyalgia (Sendur et al. 2008).
There are limited data about the effects of Mg treatment on fibromyalgia symptoms, although it has been suggested that Mg supplementation may have a role in reducing pain, tenderness, and symptom severity in patients with fibromyalgia (Bagis etal. 2013).
Table 9.7 Mechanisms by which low magnesium status may affect muscle, increasing oxidative stress
Energetic metabolism (oxygen uptake and energy production)
Transmembrane transport
Muscle contraction and relaxation (by means of MgATP and the release of Ca)
Mg and Muscle Performance
Mg status is crucial to muscle ATP concentration, muscle energetic metabolism, transmembrane transport, and muscle contraction and relaxation, while Mg deficiency is associated with poor physical performance. In agreement with the role of Mg deficiency in increasing oxidative stress and inflammation (Weglicki et al. 1996), Mg depletion is also associated with impaired intracellular calcium levels and muscle cells structural damage, affecting energetic metabolism (oxygen uptake and energy production), transmembrane transport, and muscle contraction and relaxation (Table 9.7) (Rock et al. 1995). A significant, independent and strong relationship was found between circulating Mg and muscle performance, which was consistent across several muscle parameters for both men and women (Dominguez et al. 2006).
Mg supplementation (up to 8 mg/kg daily) enhanced muscle strength, enhanced endurance performance, and decreased oxygen use in young volunteers (Brilla and Haley 1992). In older persons, oral Mg supplementation (300 mg per day) improved physical performance, in particular in those participants with a low Mg dietary intake, suggesting a role for Mg supplementation in preventing or delaying the age-related decline in physical performance (Veronese et al. 2014).
Magnesium and Cancer
A complex relationship links Mg and cancer. In animal model, Mg may exert a protective effect in the early phases of chemical carcinogenesis. It has been reported that Mg inhibits nickel-induced carcinogenesis in the rat kidney (Kasprzak et al. 1994), and protects against 3-methyl-cholantrene-induced fibrosarcomas in rats (Patiroglu et al. 1997). Mg acts as a protective agent in colorectal cancer in experimental models by inhibiting c-myc expression and ornithine decarboxylase activity in the mucosal epithelium of the intestine (Mori et al. 1997). It has been suggested that a decrease in Mg intake may increase cell proliferation by activating Ca channels (TRPM7), which can provide the milieu for the development of cancer (Hanano et al. 2004). A higher serum Ca/Mg ratio has been shown to be associated with an increased risk of postmenopausal breast cancer (Sahmoun and Singh 2010). Likewise, an increase in dietary Mg consumption has been reported to be inversely related to the risk of developing colorectal adenomas and colorectal cancer (Wark et al. 2012).
The relationship of cancer protection and Mg intake is not clear because Mg content in the diet is closely related to fiber and largely obtained from green vegetables. There is general agreement about the inverse significant correlation between the risk of cancer and the regular consumption of fruit, whole cereals and vegetables, rich sources of fiber, micronutrients, vitamins and minerals, including Mg.
Role of Magnesium in the Aging Process and Longevity
In cellular systems, Mg is highly required to maintain genomic stability. Mg has stabilizing effects on DNA and chromatin structures and is an essential cofactor in almost all enzymatic systems involved in DNA processing. Furthermore, as essential cofactor in nucleotide excision repair, base excision repair, and mismatch repair, Mg is required for the removal of DNA damage generated by environmental mutagens, endogenous processes, and DNA replication (Hartwig 2001). Thus, Mg deficiency increases the susceptibility to oxidative stress and immune dysfunction, which may decrease membrane integrity and function and contribute to several mitochondrial alterations with age (decreased number, morphology modifications, increased DNA mutations, decreased biogenesis, decreased autophagy, increased apoptosis) (Table 9.8) (Barbagallo and Dominguez 2010).
Mg has a central role in direct regulation of protein synthesis and in ancillary processes as a response to membrane perturbation and repair (Hartwig 2001; Rubin 2005). DNA is continuously damaged by environmental mutagens and by endogenous processes. Intracellular free Mg increases in cells facing apoptosis. Mg raise is an early event in apoptosis, possibly linked to a mobilization of Mg from the mitochondria, and appears to be a “second messenger” for downstream events in apoptosis (Chien et al. 1999).
There is increasing evidence from animal experiments and epidemiological studies, that Mg deficiency may decrease membrane integrity and membrane function, increasing the susceptibility to oxidative stress, cardiovascular heart diseases, as well as accelerated aging. The aging process is associated with a shortening of telomeres, repetitive DNA sequences, and associated proteins that cap and protect the ends of
__Table 9.8 Effects of aging on the mitochondria by which oxidative stress may be increased • Decreased number
Morphology modifications
Increased DNA mutations
Decreased biogenesis
Decreased autophagy
Increased apoptosischromosomes.
Low telomerase activity is associated with increased catecholamines while the sensitivity of telomere synthesis to Mg ions is primarily seen for the longer elongation products (Blackburn 2000). Several studies have reported alterations in cell physiology with senescence features during Mg deficiency in different cell types. Mg-related alterations may include reduced oxidative stress defense, cell cycle progression, culture growth, and cellular viability and activation of the expression of proto-oncogene and of transcription factors (Sgambato et al. 1999). Culture of primary fibroblasts in Mg-deficient media caused a loss of replicative capacity and an acceleration of the expression of biomarkers associated with senescence and in telomere attrition. In addition, a significant decrease in the replicative lifespan was seen compared to fibroblast populations cultured in normal Mg media conditions (Killilea and Ames 2008).
lune
s
Reduced Immune Responses
Because of the crucial role of Mg in stabilizing DNA, reducing the potential for oxidative stress and promoting DNA replication and transcription, a Mg deficiency might lead to an increased genomic instability, inhibited DNA repair, and altered function of mitochondria, thus contributing to cellular senescence and accelerated aging (Killilea and Maier 2008; Hartwig 2001). Mg protects against these effects and against the shortening of telomeres seen with lower Mg, associated with a reduction in life expectancy. It has been hypothesized that because of the effects of Mg supple-mentation in maintaining telomere length, it may also have a role in extending the life span (Rowe 2012).
Conclusions
Aging is frequently associated with chronic Mg deficiency. Several age-related chronic conditions have been linked to a low-grade chronic inflammation and/or to an excessive production of oxygen-derived free radicals. Since Mg deficits trigger both these conditions, we have previously hypothesized that a chronic Mg insufficiency may help to explain the interactions between low grade chronic inflammation and oxidative stress with the aging process and/or age-related diseases (Fig. 9.3) (Barbagallo et al. 2009; Barbagallo and Dominguez 2010).
It is thus possible to postulate that preserving an optimal Mg homeostasis throughout life might help to prevent some aging-related conditions, associated with Mg inadequacy, and may lengthen healthy life. In this context, also the possible role of Mg supplementation remains unclear. Very few prospective blind studies on the effects of Mg deficiency treatment in older adults have been performed. The possibility that Mg may supplementation may become a safe and economic health strategy in the aging population is a suggestive hypothesis that needs to be proven by future prospective studies.
References
AbbasiB, KimiagarM, Sadeghniiat K, ShiraziMM,HedayatiM,RashidkhaniB (2012) The effect of magnesium supplementation on primary insomnia in elderly: a double-blind placebo-controlled clinical trial. J Res Med Sci 17:1161-1169
Agus ZS, Kelepouris E, Dukes I, Morad M (1989) Cytosolic magnesium modulates calcium channel activity in mammalian ventricular cells. Am J Physiol 256:C452-C455
Altura BM, Altura BT (1981) Magnesium ions and contraction of vascular smooth muscles: relationship to some vascular diseases. Fed Proc 40:2672-2679 Altura BM, Altura BT (1991) Cardiovascular risk factors and magnesium: relationships to atherosclerosis, ischemic heart disease and hypertension. Magnes Trace Elem 10:182-192
Altura BM, Altura BT, Gebrewold A, Ising H, Günther T (1984) Magnesium deficiency and hypertension: correlation between magnesium-deficient diets and microcirculatory changes in situ. Science 223:1315-1317
Andrâsi E, Pâli N, Molnâr Z, Kosel S (2005) Brain aluminum, magnesium and phosphorus contents of control and Alzheimer-diseased patients. J Alzheimers Dis 7:273-284
Aydin H, Deyneli O, Yavuz D, Gozü H, Mutlu N, Kaygusuz I, Akalin S (2010) Short-term oral magnesium supplementation suppresses bone turnover in postmenopausal osteoporotic women. Biol Trace Elem Res 133:136-143
Bagis S, Karabiber M, As I, Tamer L, Erdogan C, Atalay A (2013) Is magnesium citrate treatment effective on pain, clinical parameters and functional status in patients with fibromyalgia? Rheumatol Int 33:167-172
Balon TW, Gu JL, Tokuyama Y, Jasman AP, Nadler JL (1995) Magnesium supplementation reduces development of diabetes in a rat model of spontaneous NIDDM. Am J Physiol 269:E745-E752
Barbagallo M, Dominguez LJ (2007) Magnesium metabolism in type 2 diabetes mellitus, metabolic syndrome and insulin resistance. Arch Biochem Biophys 458:40-47
Barbagallo M, Dominguez LJ (2010) Magnesium and aging. Curr Pharm Des 16:832-839
Barbagallo M, Dominguez LJ (2015) Magnesium and type 2 diabetes. World J Diabetes 6:1152-1157
Barbagallo M, Resnick LM, Sosa RE, Corbett ML, Laragh JH (1992) Renal divalent cation excretion in secondary hypertension. Clin Sci 83:561-565
Barbagallo M, Gupta RK, Dominguez LJ, Resnick LM (2000) Cellular ionic alterations with age: relation to hypertension and diabetes. J Am Geriatr Soc 48:1111-1116
Barbagallo M, Dominguez LJ, Galioto A, Ferlisi A, Cani C, Malfa L, Pineo A, Busardo’ A, Paolisso G (2003) Role of magnesium in insulin action, diabetes and cardio-metabolic syndrome X. Mol Aspects Med 24:39-52
Barbagallo M, Dominguez LJ, Resnick LM (2007) Magnesium metabolism in hypertension and type 2 diabetes mellitus. Am J Ther 14:375-385
Barbagallo M, Belvedere M, Dominguez LJ (2009) Magnesium homeostasis and aging. Magnes Res 22:235-246
Barbagallo M, Belvedere M, Di Bella G, Dominguez LJ (2011) Altered ionized magnesium levels in mild-to-moderate alzheimer’s disease. Magnes Res 24(3):S115-S121
Barbagallo M, di Bella G, Brucato V, D’Angelo D, Damiani P, Monteverde A, Belvedere M, Dominguez LJ (2014) Serum ionized magnesium in diabetic older persons. Metab Clin Exp 63:502-509
Barra A, Camardese G, Tonioni F, Sgambato A, Picello A, Autullo G, Silvia D, Bria P, Cittadini A (2007) Plasma magnesium level and psychomotor retardation in major depressed patients. Magnes Res 20:245-249
Bernstein WK, Khastgir T, Khastgir A, Hernandez E, Miller J, Schonfeld SA, Nissim JE, Chernow B (1995) Lack of effectiveness of magnesium in chronic stable asthma. A prospective, randomized, double-blind, placebo-controlled, crossover trial in normal subjects and in patients with chronic stable asthma. Arch Intern Med 155:271-276
Blackburn EH (2000) Telomere states and cell fates. Nature 408:53-56
Blackfan K, Hamilton B (1925) Uremia in acute glomerular nephritis: the cause and treatment in children. Med Surg J 193:617-628
Bloch H, Silverman R, Mancherje N, Grant S, Jagminas L, Scharf SM (1995) Intravenous magnesium sulfate as an adjunct in the treatment of acute asthma. Chest 107:1576-1581
Brilla LR, Haley TF (1992) Effect of magnesium supplementation on strength training in humans. JAm Coll Nutr 11:326-329
Britton J, Pavord I, Richards K, Wisniewski A, Knox A, Lewis S, Tattersfield A, Weiss S (1994) Dietary magnesium, lung function, wheezing, and airway hyperreactivity in a random adult population sample. Lancet 344:357-362
Bussière FI, Tridon A, Zimowska W, Mazur A, Rayssiguier Y (2003) Increase in complement component C3 is an early response to experimental magnesium deficiency in rats. Life Sci 73:499-507
Cakmak I, Yazici A, Tutus Y, Ozturk L (2009) Glyphosate reduced seed and leaf concentrations of calcium, manganese, magnesium, and iron in non-glyphosate resistant soybean. Europ J Agron 31:114-119
Calviello G, Ricci P, Lauro L, Palozza P, Cittadini A (1994) Mg deficiency induces mineral content changes and oxidative stress in rats. Biochem Mol Biol Int 32:903-911 Chien PF, Khan KS, Arnott N (1996) Magnesium sulphate in the treatment of eclampsia and pre-eclampsia: an overview of the evidence from randomised trials. Br J Obstet Gynaecol 103:1085-1091
Chien MM, Zahradka KE, Newell MK, Freed JH (1999) Fas-induced B cell apoptosis requires an increase in free cytosolic magnesium as an early event. J Biol Chem 274:7059-7066
Chiuve SE, Sun Q, Curhan GC, Taylor EN, Spiegelman D, Willett WC, Manson JE, Rexrode KM, Albert CM (2013) Dietary and plasma magnesium and risk of coronary heart disease among women. J Am Heart Assoc 2:e000114
Chyrek-Borowska S, Obrzut D, Hofman J (1978) The relation between magnesium, blood histamine level and eosinophilia in the acute stage of the allergic reactions in humans. Arch Immunol Ther Exp (Warsz) 26:709-712
Cilliler AE, Ozturk S, Ozbakir S (2007) Serum magnesium level and clinical deterioration in Alzheimer’s disease. Gerontology 53:419-422
Clapham DE, Runnels LW, Strübing C (2001) The TRP ion channel family. Nat Rev Neurosci 2:387-396
Corsonello A, Perticone F, Ientile R, Barbagallo M, Corica F (2007) Serum magnesium and lipids: more clarity is needed. Atherosclerosis 192:233-234
Coudray C, Feillet-Coudray C, Rambeau M, Tressol JC, Gueux E, Mazur A, Rayssiguier Y (2006) The effect of aging on intestinal absorption and status of calcium, magnesium, zinc, and copper in rats: a stable isotope study. J Trace Elem Med Biol 20:73-81
Decollogne S, Tomas A, Lecerf C, Adamowicz E, Seman M (1997) NMDA receptor complex blockade by oral administration of magnesium: comparison with MK-801. Pharmacol Biochem Behav 58:261-268
Derom ML, Sayón-Orea C, Martínez-Ortega JM, Martínez-González MA (2013) Magnesium and depression: a systematic review. Nutr Neurosci 16:191-206
Dicarlo LA, Morady F, de Buitleir M, Krol RB, Schurig L, Annesley TM (1986) Effects of magnesium sulfate on cardiac conduction and refractoriness in humans. J Am Coll Cardiol 7:1356-1362
Dickinson HO, Nicolson DJ, Campbell F, Cook JV, Beyer FR, Ford GA, Mason J (2006) Magnesium supplementation for the management of essential hypertension in adults. Cochrane Database Syst Rev 3:CD004640
Dimai HP, Porta S, Wirnsberger G, Lindschinger M, Pamperl I, Dobnig H, Wilders-Truschnig M, Lau KH (1998) Daily oral magnesium supplementation suppresses bone turnover in young adult males. J Clin Endocrinol Metab 83:2742-2748
Djurhuus MS, Sk0tt P, Hother-Nielson O, Klitgaard NA, Beck-Nielsen H (1995) Insulin increases renal magnesium excretion: a possible cause of magnesium depletion in hyperinsulinaemic states. Diabet Med 12:664-669
Dominguez LJ, Barbagallo M, di Lorenzo G, Drago A, Scola S, Morici G, Caruso C (1998) Bronchial reactivity and intracellular magnesium: A possible mechanism for the bronchodilating effects of magnesium in asthma. Clin Sci 95:137-142
Dominguez LJ, Barbagallo M, Lauretani F, Bandinelli S, Bos A, Corsi AM, Simonsick EM, Ferrucci L (2006) Magnesium and muscle performance in older persons: the InCHIANTI study. Am J Clin Nutr 84:419-426
Durlach J, Bara M, Guiet-Bara A (1985) Magnesium level in drinking water and cardiovascular risk factor: a hypothesis. Magnesium 4:5-15
Durlach J, Bac P, Bara M, Guiet-Bara A (2000) Physiopathology of symptomatic and latent forms of central nervous hyperexcitability due to magnesium deficiency: a current general scheme. Magnes Res 13:293-302
Eby GA, Eby KL (2010) Magnesium for treatment-resistant depression: a review and hypothesis. Med Hypotheses 74:649-660
Elin RJ (2010) Assessment of magnesium status for diagnosis and therapy. Magnes Res 23:S194-S198
Falkner D, Glauser J, Allen M (1992) Serum magnesium levels in asthmatic patients during acute exacerbations of asthma. Am J Emerg Med 10:1-3
Faouzi M, Kilch T, Horgen FD, Fleig A, Penner R (2017) The TRPM7 channel kinase regulates store-operated calcium entry. J Physiol 595:3165-3180
Ford ES, Mokdad AH (2003) Dietary magnesium intake in a national sample of US adults. J Nutr 133:2879-2882
Franceschi C, Garagnani P, Vitale G, Capri M, Salvioli S (2017) Inflammaging and ‘Garb-aging’. Trends Endocrinol Metab 28:199-212
Fung TT, Manson JE, Solomon CG, Liu S, Willett WC, Hu FB (2003) The association between magnesium intake and fasting insulin concentration in healthy middle-aged women. J Am Coll Nutr 22:533-538
Galan P, Preziosi P, Durlach V, Valeix P, Ribas L, Bouzid D, Favier A, Hercberg S (1997) Dietary magnesium intake in a French adult population. Magnes Res 10:321-328
Galan P, Arnaud MJ, Czernichow S, Delabroise AM, Preziosi P, Bertrais S, Franchisseur C, Maurel M, Favier A, Hercberg S (2002) Contribution of mineral waters to dietary calcium and magnesium intake in a French adult population. J Am Diet Assoc 102:1658-1662
Galland L (1988) Magnesium and immune function: an overview. Magnesium 7:290-299 Galland L (1991) Magnesium, stress and neuropsychiatric disorders. Magnes Trace Elem 10:287-301
Glick JL (1990) Dementias: the role of magnesium deficiency and an hypothesis concerning the pathogenesis of Alzheimer’s disease. Med Hypotheses 31:211-225
Goto Y, Nakamura M, Abe S, Kato M, Fukui M (1993) Physiological correlates of abnormal behaviors in magnesium-deficient rats. Epilepsy Res 15:81-89 Griffiths AM, Cook DM, Eggett DL, Christensen MJ (2012) A retail market study of organic and conventional potatoes (Solanum tuberosum): mineral content and nutritional implications. Int J Food Sci Nutr 63:393-401
Guerrero-Romero F, Bermudez-Peña C, Rodríguez-Morán M (2011) Severe hypomagnesemia and low-grade inflammation in metabolic syndrome. Magnes Res 24:45-53
Gullestad L, Midtvedt K, Dolva LO, Norseth J, Kjekshus J (1994) The magnesium loading test: reference values in healthy subjects. Scand J Clin Lab Invest 54:23-31
Gupta A, Lawrence AT, Krishnan K, Kavinsky CJ, Trohman RG (2007) Current concepts in the mechanisms and management of drug-induced QT prolongation and torsade de pointes. Am Heart J153:891-899
Gustafson T, Boman K, Rosenhall L, Sandstrom T, Wester PO (1996) Skeletal muscle magnesium and potassium in asthmatics treated with oral beta 2-agonists. Eur Respir J 9:237-240
Hanano T, Hara Y, Shi J, Morita H, Umebayashi C, Mori E, Sumimoto H, Ito Y, Mori Y, Inoue R (2004) Involvement of TRPM7 in cell growth as a spontaneously activated Ca2+ entry pathway in human retinoblastoma cells. J Pharmacol Sci 95:403-419
Hartwig A (2001) Role of magnesium in genomic stability. Mutat Res 475:113-121 Haury VG (1940) Blood serum magnesium in bronchial asthma and its treatment by the administration of magnesium sulfate. J Lab Clin Med 26:340-344
He K, Liu K, Daviglus ML, Morris SJ, Loria CM, van Horn L, Jacobs DR, Savage PJ (2006) Magnesium intake and incidence of metabolic syndrome among young adults. Circulation 113:1675-1682
Humphries S, Kushner H, Falkner B (1999) Low dietary magnesium is associated with insulin resistance in a sample of young, nondiabetic Black Americans. Am J Hypertens 12:747-756 Hunt CD, Johnson LK (2006) Magnesium requirements: new estimations for men and women by cross-sectional statistical analyses of metabolic magnesium balance data. Am J Clin Nutr 84:843-852
Iseri LT, French JH (1984) Magnesium: nature’s physiologic calcium blocker. Am Heart J 108:188-193
Joffres MR, Reed DM, Yano K (1987) Relationship of magnesium intake and other dietary factors to blood pressure: the Honolulu heart study. Am J Clin Nutr 45:469-475
Kasprzak KS, Diwan BA, Rice JM (1994) Iron accelerates while magnesium inhibits nickel-induced carcinogenesis in the rat kidney. Toxicology 90:129-140
Kemp PA, Gardiner SM, March JE, Bennett T, Rubin PC (1994) Effects of NG-nitro-L-arginine methyl ester on regional haemodynamic responses to MgSO4 in conscious rats. Br J Pharmacol 111:325-331
Kenney MA, McCoy H, Williams L (1994) Effects of magnesium deficiency on strength, mass, and composition of rat femur. Calcif Tissue Int 54:44-49 Khan AM, Lubitz SA, Sullivan LM, Sun JX, Levy D, Vasan RS, Magnani JW, Ellinor PT, Benjamin EJ, Wang TJ (2013) Low serum magnesium and the development of atrial fibrillation in the community: the Framingham heart study. Circulation 127:33-38
Killilea DW, Ames BN (2008) Magnesium deficiency accelerates cellular senescence in cultured human fibroblasts. Proc Natl Acad Sci USA 105:5768-5773
Killilea DW, Maier JA (2008) A connection between magnesium deficiency and aging: new insights from cellular studies. Magnes Res 21:77-82
King DE, Mainous AG, Geesey ME, Woolson RF (2005) Dietary magnesium and C-reactive protein levels. J Am Coll Nutr 24:166-171
Kirov GK, Birch NJ, Steadman P, Ramsey RG (1994) Plasma magnesium levels in a population of psychiatric patients: correlations with symptoms. Neuropsychobiology 30:73-78
Kobayashi J (1957) On geographical relationship between the chemical nature of river water and death rate from apoplexy. Ber Ohara Inst 11:12-21 Kramer JH, Mak IT, Phillips TM, Weglicki WB (2003) Dietary magnesium intake influences circulating pro-inflammatory neuropeptide levels and loss of myocardial tolerance to postischemic stress. Exp Biol Med (Maywood) 228:665-673
Lopez-Ridaura R, Willett WC, Rimm EB, Liu S, Stampfer MJ, Manson JE, Hu FB (2004) Magnesium intake and risk of type 2 diabetes in men and women. Diabetes Care 27:134-140
Malpuech-Brugère C, Nowacki W, Gueux E, Kuryszko J, Rock E, Rayssiguier Y, Mazur A (1999) Accelerated thymus involution in magnesium-deficient rats is related to enhanced apoptosis and sensitivity to oxidative stress. Br J Nutr 81:405-411
Malpuech-Brugère C, Nowacki W, Daveau M, Gueux E, Linard C, Rock E, Lebreton J, Mazur A, Rayssiguier Y (2000) Inflammatory response following acute magnesium deficiency in the rat. Biochim Biophys Acta 1501:91-98
Mather HM, Levin GE (1979) Magnesium status in diabetes. Lancet 1:924 Matsunobu S, Terashima Y, Senshu T, Sano H, Itoh H (1990) Insulin secretion and glucose uptake in hypomagnesemic sheep fed alow magnesium, high potassium diet. J NutrBiochem 1:167-171
Mazur A, Maier JA, Rock E, Gueux E, Nowacki W, Rayssiguier Y (2007) Magnesium and the inflammatory response: potential physiopathological implications. Arch Biochem Biophys 458:48-56
McLean RM (1994) Magnesium and its therapeutic uses: a review. Am J Med 96:63-76
McNair P, Christensen MS, Christiansen C, Madsbad S, Transbpl I (1982) Renal hypomagnesaemia in human diabetes mellitus: its relation to glucose homeostasis. Eur J Clin Invest 12:81-85
Medalle R, Waterhouse C, Hahn TJ (1976) Vitamin D resistance in magnesium deficiency. Am J Clin Nutr 29:854-858
MoriH, Tanaka T, Sugie S, Yoshimi N, KawamoriT, Hirose Y, OhnishiM (1997) Chemoprevention by naturally occurring and synthetic agents in oral, liver, and large bowel carcinogenesis. J Cell Biochem Suppl 27:35-41
Nadler JL, Goodson S, Rude RK (1987) Evidence that prostacyclin mediates the vascular action of magnesium in humans. Hypertension 9:379-383 Nechifor M (2009) Magnesium in major depression. Magnes Res 22:163S-166S
New SA, Robins SP, Campbell MK, Martin JC, Garton MJ, Bolton-Smith C, Grubb DA, Lee SJ, Reid DM (2000) Dietary influences on bone mass and bone metabolism: further evidence of a positive link between fruit and vegetable consumption and bone health? Am J Clin Nutr 71:142-151
Nielsen FH, Milne DB, Klevay LM, Gallagher S, Johnson L (2007) Dietary magnesium deficiency induces heart rhythm changes, impairs glucose tolerance, and decreases serum cholesterol in post menopausal women. J Am Coll Nutr 26:121-132
Okayama H, Aikawa T, Okayama M, Sasaki H, Mue S, Takishima T (1987) Bronchodilating effect of intravenous magnesium sulfate in bronchial asthma. JAMA 257:1076-1078
Onalan O, Crystal E, Daoulah A, Lau C, Crystal A, Lashevsky I (2007) Meta-analysis of magnesium therapy for the acute management of rapid atrial fibrillation. Am J Cardiol 99:1726-1732
Paolisso G, Barbagallo M (1997) Hypertension, diabetes mellitus, and insulin resistance. The role of intracellular magnesium. Am J Hypertens 10:346-355 Patiroglu T, Sahin G, Kontag O, Uzüm K, Saraymen R (1997) Protective effect of magnesium supplementation on experimental 3-methyl cholanthrene-induced fibrosarcoma and changes in tissue magnesium distribution during carcinogenesis in rats. Biol Trace Elem Res 56:179-185
Penner R, Fleig A (2007) The Mg2+ and Mg(2+)-nucleotide-regulated channel-kinase TRPM7. Handb Exp Pharmacol 179:313-328
Petersen B, Schroll M, Christiansen C, Transbol I (1977) Serum and erythrocyte magnesium in normal elderly danish people. Relationship to blood pressure and serum lipids. Acta Med Scand 201:31-34
Quamme GA (1997) Renal magnesium handling: new insights in understanding old problems. Kidney Int 52:1180-1195
Quamme GA (2008) Recent developments in intestinal magnesium absorption. Curr Opin Gastroenterol 24:230-235
Randell EW, Mathews M, Gadag V, Zhang H, Sun G (2008) Relationship between serum magnesium values, lipids and anthropometric risk factors. Atherosclerosis 196:413-419
Rayssiguier Y (1984) Role of magnesium and potassium in the pathogenesis of arteriosclerosis. Magnesium 3:226-238
Reinhart RA (1988) Magnesium metabolism. A review with special reference to the relationship between intracellular content and serum levels. Arch Intern Med 148:2415-2420
Resnick LM, Laragh JH (1985) Renin, calcium metabolism and the pathophysiologic basis of antihypertensive therapy. Am J Cardiol 56:68H-74H
Resnick LM, Gupta RK, Laragh JH (1984) Intracellular free magnesium in erythrocytes of essential hypertension: relation to blood pressure and serum divalent cations. Proc Natl Acad Sci USA 81:6511-6515
Resnick LM, Altura BT, Gupta RK, Laragh JH, Alderman MH, Altura BM (1993) Intracellular and extracellular magnesium depletion in type 2 (non-insulin-dependent) diabetes mellitus. Dia- betologia 36:767-770
Resnick LM, Gupta RK, Difabio B, Barbagallo M, Mann S, Marion R, Laragh JH (1994) Intracellular ionic consequences of dietary salt loading in essential hypertension. Relation to blood pressure and effects of calcium channel blockade. J Clin Invest 94:1269-1276
Resnick LM, Bardicef O, Altura BT, Alderman MH, Altura BM (1997) Serum ionized magnesium: relation to blood pressure and racial factors. Am J Hypertens 10:1420-1424
Rock E, Astier C, Lab C, Vignon X, Gueux E, Motta C, Rayssiguier Y (1995) Dietary magnesium deficiency in rats enhances free radical production in skeletal muscle. J Nutr 125:1205-1210
Rodríguez-Morán M, Simental Mendia LE, Zambrano Galván G, Guerrero-Romero F (2011) The role of magnesium in type 2 diabetes: a brief based-clinical review. Magnes Res 24:156-162
Rolla G, Bucca C, Brussino L, Colagrande P (1994) Effect of intravenous magnesium infusion on salbutamol-induced bronchodilatation in patients with asthma. Magnes Res 7:129-133
Romani AM (2011) Cellular magnesium homeostasis. Arch Biochem Biophys 512:1-23
Rosanoff A, Seelig MS (2004) Comparison of mechanism and functional effects of magnesium and statin pharmaceuticals. J Am Coll Nutr 23:501S-505S
Rowe WJ (2012) Correcting magnesium deficiencies may prolong life. Clin Interv Aging 7:51-54 Rubin H (2005) Magnesium: The missing element in molecular views of cell proliferation control. BioEssays 27:311-320
Rude RK, Gruber HE (2004) Magnesium deficiency and osteoporosis: animal and human observations. J Nutr Biochem 15:710-716
Rude RK, Kirchen ME, Gruber HE, Meyer MH, Luck JS, Crawford DL (1999) Magnesium deficiency-induced osteoporosis in the rat: uncoupling of bone formation and bone resorption. Magnes Res 12:257-267
Ryder KM, Shorr RI, Bush AJ, Kritchevsky SB, Harris T, Stone K, Cauley J, Tylavsky FA (2005) Magnesium intake from food and supplements is associated with bone mineral density in healthy older white subjects. J Am Geriatr Soc 53:1875-1880
Sahmoun AE, Singh BB (2010) Does a higher ratio of serum calcium to magnesium increase the risk for postmenopausal breast cancer? Med Hypotheses 75:315-318
Saris NE, Mervaala E, Karppanen H, Khawaja JA, Lewenstam A (2000) Magnesium. An update on physiological, clinical and analytical aspects. Clin Chim Acta 294:1-26
Schnack C, Bauer I, Pregant P, Hopmeier P, Schernthaner G (1992) Hypomagnesaemia in type 2 (non-insulin-dependent) diabetes mellitus is not corrected by improvement of long-term metabolic control. Diabetologia 35:77-79
Schroeder HA (1966) Municipal drinking water and cardiovascular death rates. JAMA 195:81-85
Seelig MS (1994) Consequences of magnesium deficiency on the enhancement of stress reactions; preventive and therapeutic implications (a review). J Am Coll Nutr 13:429-446
Sendur OF, Tastaban E, Turan Y, Ulman C (2008) The relationship between serum trace element levels and clinical parameters in patients with fibromyalgia. Rheumatol Int 28:1117-1121
Sgambato A, Wolf FI, FaragliaB, Cittadini A (1999) Magnesium depletion causes growth inhibition, reduced expression of cyclin D1, and increased expression of P27Kip1 in normal but not in transformed mammary epithelial cells. J Cell Physiol 180:245-254
Shils ME (1969) Experimental production of magnesium deficiency in man. Ann N Y Acad Sci 162:847-855
Singh RB, Manmohan MD, Dube KP, Singh VP (1976) Serum magnesium concentrations in atrial fibrillation. Acta Cardiol 31:221-226
Skorodin MS, Freebeck PC, Yetter B, Nelson JE, van de Graaff WB, Walsh JM (1994) Magnesium sulfate potentiates several cardiovascular and metabolic actions of terbutaline. Chest 105:701-705
Song Y, Manson JE, Buring JE, Liu S (2004) Dietary magnesium intake in relation to plasma insulin levels and risk of type 2 diabetes in women. Diabetes Care 27:59-65
Song Y, Ridker PM, Manson JE, Cook NR, Buring JE, Liu S (2005) Magnesium intake, C-reactive protein, and the prevalence of metabolic syndrome in middle-aged and older U.S. women. Diabetes Care 28:1438-1444
Song Y, Li TY, van Dam RM, Manson JE, Hu FB (2007) Magnesium intake and plasma concentrations of markers of systemic inflammation and endothelial dysfunction in women. Am J Clin Nutr 85:1068-1074
Stepura OB, Martynow AI (2009) Magnesium orotate in severe congestive heart failure (MACH). Int J Cardiol 134:145-147
Tam M, Gomez S, Gonzalez-Gross M, Marcos A (2003) Possible roles of magnesium on the immune system. Eur J Clin Nutr 57:1193-1197
Tiffany BR, Berk WA, Todd IK, White SR (1993) Magnesium bolus or infusion fails to improve expiratory flow in acute asthma exacerbations. Chest 104:831-834
Tucker KL, Hannan MT, Chen H, Cupples LA, Wilson PW, Kiel DP (1999) Potassium, magnesium, and fruit and vegetable intakes are associated with greater bone mineral density in elderly men and women. Am J Clin Nutr 69:727-736
Turlapaty PD, Altura BM (1980) Magnesium deficiency produces spasms of coronary arteries: relationship to etiology of sudden death ischemic heart disease. Science 208:198-200
Tzivoni D, Banai S, Schuger C, Benhorin J, Keren A, Gottlieb S, Stern S (1988) Treatment of torsade de pointes with magnesium sulfate. Circulation 77:392-397
Veronese N, Berton L, Carraro S, Bolzetta F, de Rui M, Perissinotto E, Toffanello ED, Bano G, Pizzato S, Miotto F, Coin A, Manzato E, Sergi G (2014) Effect of oral magnesium supplementation on physical performance in healthy elderly women involved in a weekly exercise program: a randomized controlled trial. Am J Clin Nutr 100:974-981
Veronese N, Watutantrige-Fernando S, Luchini C, Solmi M, Sartore G, Sergi G, Manzato E, Barba- gallo M, Maggi S, Stubbs B (2016) Effect of magnesium supplementation on glucose metabolism in people with or at risk of diabetes: a systematic review and meta-analysis of double-blind randomized controlled trials. Eur J Clin Nutr 70:1354-1359
Veronese N, Stubbs B, Solmi M, Noale M, Vaona A, Demurtas J, Maggi S (2017) Dietary magnesium intake and fracture risk: data from a large prospective study. Br J Nutr 117:1-7
von Ehrlich B, Barbagallo M, Classen HG, Guerrero-Romero F, Mooren FC, Rodriguez-Moran M, Vierling W, Vormann J, Kisters K (2014) The significance of magnesium in insulin resistance, metabolic syndrome and diabetes—recommendations of the association of magnesium research e.V. (Die Bedeutung von Magnesium für Insulinresistenz, metabolisches Syndrom und Diabetes mellitus—Empfehlungen der Gesellschaft für Magnesium-Forschung e.V.). Diabetologie und Stoffwechsel 9:96-100
Vural H, Demirin H, Kara Y, Eren I, Delibas N (2010) Alterations of plasma magnesium, copper, zinc, iron and selenium concentrations and some related erythrocyte antioxidant enzyme activities in patients with Alzheimer’s disease. J Trace Elem Med Biol 24:169-173 Wälti MK, Zimmermann MB, Walczyk T, Spinas GA, Hurrell RF (2003) Measurement of magnesium absorption and retention in type 2 diabetic patients with the use of stable isotopes. Am J Clin Nutr 78:448-453
Wark PA, Lau R, Norat T, Kampman E (2012) Magnesium intake and colorectal tumor risk: a case-control study and meta-analysis. Am J Clin Nutr 96:622-631
Weglicki WB, Bloom S, Cassidy MM, Freedman AM, Atrakchi AH, Dickens BF (1992) Antioxidants and the cardiomyopathy of Mg-deficiency. Am J Cardiovasc Pathol 4:210-215
Weglicki WB, Mak IT, Kramer JH, Dickens BF, Cassidy MM, Stafford RE, Philips TM (1996) Role of free radicals and substance P in magnesium deficiency. Cardiovasc Res 31:677-682
Winkler AW, Smith PK, Hoff HE (1942) Intravenous magnesium sulfate in the treatment of nephritic convulsions in adults. J Clin Invest 21:207-216
Yang XY, Hosseini JM, Ruddel ME, Elin RJ (1990) Blood magnesium parameters do not differ with age. J Am Coll Nutr 9:308-313
VitaminDWiki - Magnesium and Vitamin D contains
{include}
VitaminDWiki - Overview Magnesium and vitamin D Has a venn diagram
{include}
VitaminDWiki - studies in both categories Magnesium and Mortality
This list is automatically updated
{category}
Some Google Scholar items on Magnesium and Health- Oct 2022
Deficient energy metabolism is associated with low free magnesium in the brains of patients with migraine and cluster headache - March 2001 - https://doi.org/10.1016/S0361-9230(01)00440-3
SARS-CoV-2: influence of phosphate and magnesium, moderated by vitamin D, on energy (ATP) metabolism and on severity of COVID-19 Jan 2021 https://doi.org/10.1152/ajpendo.00474.2020 FREE PDF
Energy Metabolism Impairment in Migraine - 2019, https://doi.org/10.2174/0929867325666180622154411
Magnesium in Aging, Health and Diseases Jan 2021, https://doi.org/10.3390/nu13020463 - FREE PDF
- cardiovascular diseases, hypertension and stroke, cardio-metabolic syndrome and type 2 diabetes mellitus, airways constrictive syndromes and asthma, depression, stress-related conditions and psychiatric disorders, Alzheimer’s disease (AD) and other dementia syndromes, muscular diseases (muscle pain, chronic fatigue, and fibromyalgia), bone fragility, and cancer.
Magnesium and Fibromyalgia: A Literature Review - Aug 2021 https://doi.org/10.1177/21501327211038433 FREE PDF
Magnesium Role in Health and Longevity Nov 2018 - https://doi.org/10.1007/978-3-030-03742-0_9
Magnesium Status and Stress: The Vicious Circle Concept Revisited - Nov 2020 https://doi.org/10.3390/nu12123672 FREE PDF
Magnesium Deficiency Questionnaire: A New Non-Invasive Magnesium Deficiency Screening Tool Developed Using Real-World Data from Four Observational Studies - July 2020 https://doi.org/10.3390/nu12072062 - FREE PDF
Variations in Magnesium Concentration Are Associated with Increased Mortality: Study in an Unselected Population of Hospitalized Patients June 2020,https://doi.org/10.3390/nu12061836 FREE PDF
Magnesium: Biochemistry, Nutrition, Detection, and Social Impact of Diseases Linked to Its Deficiency - March 2021 https://doi.org/10.3390/nu13041136 FREE PDF
Effectively Prescribing Oral Magnesium Therapy for Hypertension: A Categorized Systematic Review of 49 Clinical Trials - Jan 2021https://doi.org/10.3390/nu13010195
- oral magnesium (≥240 mg/day) safely lowers BP in Uncontrolled Hypertensive patients taking antihypertensive medications, while >600 mg/day magnesium is required to safely lower BP in Untreated Hypertensives; <600 mg/day for non-medicated hypertensives may not lower both SBP and DBP but may safely achieve other risk factor improvements without antihypertensive medication side effects
The effect of vitamin D and magnesium supplementation on the mental health status of attention-deficit hyperactive children: a randomized controlled trial - 2021 - https://bmcpediatr.biomedcentral.com/articles/10.1186/s12887-021-02631-1 FREE PDF
- Vitamin D (50,000 IU/week) and magnesium (6 mg/kg/day) co-supplementation for a duration of 8-weeks could improve the behavioral function and mental health of children with ADHD
Challenges in the Diagnosis of Magnesium Status - Sept 2018 https://doi.org/10.3390/nu10091202 FREE PDF
- "Magnesium is a critical mineral in the human body and is involved in ~80% of known metabolic functions. It is currently estimated that 60% of adults do not achieve the average dietary intake (ADI) and 45% of Americans are magnesium deficient, a condition associated with disease states like hypertension, diabetes, and neurological disorders, to name a few."