No NCAA player had a healthy Omega-3 index
The Omega-3 Index in National Collegiate Athletic Association Division I Collegiate Football Athletes
Journal of Athletic Training 2019;54(1):000—000, doi: 10.4085/1062-6050-387-18
📄 Download the PDF from VitaminDWiki
Anthony Anzalone, MS; Aaron Carbuhn, PhD, Rdf; Lauren Jones, MS, RD, CSSDi; Ally Gallop, MS, RD, CSSDi; Alex Smith, MS, RDJ; Palmer Johnson, mS, RD§; Lisa Swearingen, MS, RDII; Craig Moore, RD, CsSd±; Ernest Rimeri; Joe McBethi; William Harris, PhD #; K. Michelle Kirkff; David Gable, MS, ATC, LAT; Andrew Askow, BS; Will Jennings, BS; Jonathan M. Oliver, PhD
- The Sport Science Center at Texas Christian University, Fort Worth; tDepartment of Dietetics and Nutrition, University of Kansas Medical Center, Kansas City; University of Utah Athletics, Salt Lake City; §University of Missouri Athletics, Columbia; IIUniversity of South Carolina Athletics, Columbia; Department of Internal Medicine, Sanford School of Medicine, University of South Dakota, Vermillion; #OmegaQuant, LLC, Sioux Falls, SD; **Athletics and ttJPS Sports Medicine Fellowship, Texas Christian University, Fort Worth
Context: The essential omega-3 fatty acids (m-3 FAs) eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) exhibit vital biological roles and are critical for cardiovascular and neurologic health. Compared with the general population, football athletes may be at an increased risk of cardiovascular disease. Further, those same athletes are also exposed to repetitive head impacts, which may lead to long-term neurologic deficits. Both diets high in m-3 FAs and supplementation with m-3 FAs have been reported to reduce the risk of cardiovascular disease, and early evidence suggests a potential neuroprotective effect of supplementation.
Objective: To determine the (1) erythrocyte content of DHA and Epa, as measured by the Omega-3 Index, expressed as a percentage of total fatty acids, in National Collegiate Athletic Association Division I football athletes and (2) the distribution across the Omega-3 Index risk zones established for cardiovascular disease: high risk, <4%; intermediate risk, 4% to 8%; and low risk, >8%.
Design: Cross-sectional descriptive study.
Setting: Multicenter trial.
Patients or Other Participants: Deidentified data including complete erythrocyte fatty acid profile from the 2017-2018 season, age at time of testing, height, weight, and ethnicity were collected from 404 athletes.
Main Outcome Measure(s): Omega-3 Index.
Results: About
34% of athletes (n = 138) had an Omega-3 Index considered high risk (<4%), and
66% (n = 266) had a risk considered intermediate (4%-8%).
None had a low-risk Omega- 3 Index.
Conclusions: The Omega-3 Index is a simple, minimally invasive test of m-3 FA status. Our data indicate that football athletes may be deficient in the m-3 FAs DHA and EPA. The fact that no athlete had an Omega-3 Index associated with low risk suggests football athletes may be at increased risk for cardiovascular disease in later life.
Key Points
Football athletes constitute an at-risk population for cardiovascular disease and head trauma.
Omega-3 (m-3) fatty acids are reportedly beneficial for cardiovascular disease and neuroprotection.
Football athletes were deficient in m-3 fatty acids.
A focus on ingestion of m-3 and potential supplementation should be considered.
Eicosapentaenoic acid (EPA; 20: 5, n-3) and docosahexaenoic acid (DHA; 22:6, n-3), long-chain polyunsaturated fatty acids (FAs) of the omega-3 (m-3) FA family, exhibit vital biological roles as components of phospholipid cell membranes and have been reported1 to be critical for cardiovascular and neurologic development and health. Humans have a limited capacity to synthesize these essential m-3 FAs from precursor FA a- linolenic acid (ALA; 18:3, n-3),2 and thus must obtain these fats from the diet. Despite the importance of these m-3 FAs, worldwide consumption is low.3 In fact, the EPA and DHA blood levels of North Americans (those in Canada and the United States) rank ‘‘very low’’ among countries.3
Compared with the general population, American football athletes may experience an increased risk for cardiovascular disease (CVD).4 A meta-analysis5 of 10 studies demonstrated that m-3 FA status was inversely associated with CVD risk. Additional data supported those findings, as EPA and DHA administration reduced the risk of CVD and may reduce the risk of coronary heart disease mortality and stroke.6 Furthermore, the same athletes were exposed to repetitive head injuries.7 Animal models consistently demonstrated that treatment with DHA attenuated axonal damage, a characteristic of head trauma,8 when administered before insult.9-11 In addition, recent evidence12 from football athletes indicates a potential neuroprotective effect of DHA as measured by a surrogate marker of head trauma.
The Omega-3 Index, the sum of EPA and DHA levels in erythrocyte membranes, expressed as a percentage of total erythrocyte FA, reflects EPA and DHA intake and status in other tissues.13,14 This measure could provide unique insight into the ffl-3 FA status of potential at-risk populations, such as football athletes. To date, no authors have examined the Omega-3 Index of National Collegiate Athletic Association (NCAA) football players, a population at risk for both CVD4 and neurologic damage secondary to repetitive head injuries.7 Therefore, we took an exploratory approach to examining the ffl-3 FA status as measured by the Omega-3 Index among a cohort of NCAA football athletes. Also, given that the FA intake is related to erythrocyte FAs, we also obtained a complete FA profile.
METHODS
Data Collection
A retrospective, cross-sectional investigation was conducted to assess Omega-3 status among NCAA Division I football athletes. Given the noninvasive, retrospective nature of the study and the minimal risk posed to privacy, the institutional review board approved the study and granted a full waiver of consent. Four geographically distinct Division I football programs that independently included the Omega-3 Index as part of standard-of-care athlete health and wellness monitoring were identified. From those deidentified data, a complete erythrocyte FA profile (conducted by the same independent commercial laboratory), age at the time of testing, height, weight, and ethnicity from the 2017-2018 season were collected from 404 athletes.
The Erythrocyte FA Analyses
The erythrocyte FA analyses were conducted by OmegaQuant Analytics, LLC (Sioux Falls, SD), a Clinical Laboratory Improvement Amendments—certified laboratory providing FA and Omega-3 Index testing.
One drop of whole blood collected from a finger stick was placed on proprietary filter paper pretreated with an antioxidant cocktail fatty acid preservative solution and allowed to dry at room temperature for 15 minutes. After arrival at the laboratory, a punch from the dried blood spot card was transferred to a screw-cap glass vial and a mixture of methanol (containing 14% boron trifluoride) and toluene (35:30:35 v/v/v; Sigma-Aldrich, St Louis, mO) was added to the vial. The vial was briefly vortexed and heated in a hot bath at 100°C for 45 minutes. After cooling, hexane (EMD Chemicals, Philadelphia, PA) and high-pressure liquid chromatography-grade water were added and the tubes were recapped, vortexed briefly, and centrifuged to separate the layers. An aliquot of the hexane layer was transferred to a gas chromatography vial. Gas chromatography was carried out using a model GC-2010 Gas Chromatograph
Table 1. Demographic Characteristics of Study Participants (N = 404)
(Shimadzu Corporation, Columbia, MD) equipped with an SP-2560, 100-m fused silica capillary column (0.25-mm internal diameter, 0.2-pm film thickness; Supelco, Belle- fonte, PA).
Fatty acids were identified by comparison with a standard mixture of fatty acids characteristic of erythrocytes (model GLC OQ-A; NuCheck Prep, Elysian, MN), which was also used to construct individual fatty acid calibration curves. For each test, the following 24 fatty acids (by class) were identified: saturated (14:0, 16:0, 18:0, 20:0, 22:0, 24:0); cis monounsaturated (16:1, 18:1,20:1,24:1); trans (16:1, 18:1, 18:2); cis n-6 polyunsaturated (18:2, 18:3, 20:2, 20:3, 20:4, 22:4, 22:5); and cis n-3 polyunsaturated (18:3, 20:5, 22:5, 22:6). The coefficients of variation for all the fatty acids measured were <6%. The Omega-3 Index was defined as red blood cell EPA + DHA, which was derived from the dried blood spot EPA + DHA value by a regression equation (r = 0.97). The coefficient of variation for this metric was <5%.
Statistical Analysis
We categorized athletes based on the proposed Omega-3 Index risk zones for CVD5: high risk, <4%; intermediate risk, 4% to 8%; and low risk, >8%. Means and standard deviations were computed.
RESULTS
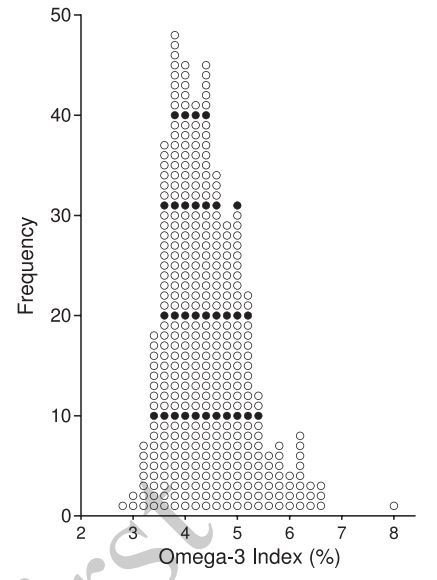
Demographics are presented in Table 1. The mean Omega-3 Index among all athletes was 4.4% ± 0.8%. In other words, EPA + DHA accounted for <5% of all the FAs present. Results from the erythrocyte FA analysis are reported in Table 2. The Figure provides a histogram of the players’ Omega-3 Indexes. A total of 34% (n = 138) had an Omega-3 Index of <4%, or high risk, whereas 66% (n = 266) were stratified into the intermediate-risk category. No participants had an Omega-3 Index associated with low risk. Only 1 participant had an Omega-3 Index of 8, just below the cutoff for low risk.
DISCUSSION
Table 2. Erythrocyte Fatty Acid Composition in Athletes as a Percentage of Total Fatty Acids Analyzed
Figure. Histogram of Omega-3 Index in a sample of collegiate football athletes (n = 404).
We measured the ffl-3 FA status, specifically EPA and DHA, as well as the FA profile of a large cohort of NCAA football athletes. To our knowledge, this is the first investigation of the ffl-3 FA status of a representative group of NCAA football athletes. Our main finding was that none of the football athletes had an Omega-3 Index above the targeted value for a reduction in CVD risk (8%).
Though most health concerns are common to the majority of the population, football athletes have unique concerns because of sport participation. For example, although increased body mass is associated with increased playing time and greater rates of pay,15 evidence4 suggests that the increase in size observed, particularly over the last several decades, has direct implications for player health. In addition to high rates of obesity,16 a large percentage of football athletes are either prehypertensive or hyperten- sive17 and present with dyslipidemia,18 factors that increase the risk of CVD.4 Diets high in m-3 FA reduce blood pressure19 and circulating triglycerides.20 The Omega-3 Index was proposed as a clinical stratification system that provides information regarding the CVD risk,21 and researchers5 recently confirmed that an Omega-3 Index <4% constituted high risk and >8%, low risk, for the development of fatal CVD. These data suggest that, at least in the current cohort of football athletes, another risk factor for CVD was present.
Football athletes are also at an increased risk of head trauma,7 which, even in the absence of a clinically discernible injury, results in quantifiable pathophysiological changes.22 Indeed, a lifetime of head trauma associated with participation in sport may lead to long-term neurologic consequences.23 A unique pathologic consequence of traumatic brain injury (TBI) in animal models is a reduction in neuronal DHA after injury,24 and deficient brain DHA content in animal models, as induced by dietary restriction, heightens the pathophysiological response to injury.25 This may at least partially explain why animal models of TBI clearly demonstrated that prophylactic m-3 FA supplementation attenuated the pathophysiological response.26 Two clinical case studies of human patients with severe head trauma showed a potential benefit of m-3 FA supplementation,27,28 and a single clinical trial12 conducted in humans identified a potential neuroprotective effect of DHA supplementation in football athletes.
The neuroprotective effects of supplemental DHA observed in rodent models of TBI demonstrated the greatest efficacy when administered at a dose9 of 40 mg-kg-1-d-1, which corresponds to a dose of approximately 4 g-kg-1-d-1 in today’s collegiate football athlete.29 This is higher than has been reported. Arterburn et al1 described a dose- dependent relationship in which plasma DHA increased up to a dosage of approximately 2 g-d-1. Above that dose, only incremental increases were observed as saturation was approached.1 A dose-response effect was noted in the only clinical trial12 in which doses of 2, 4, and 6 g-d-1 were provided to collegiate football athletes. The substantial increases observed with the 4 and 6 g-d-1 doses led those authors to suggest that higher doses may be necessary, as no apparent plateau was observed. Given the larger size of football athletes compared with the general population and other athletes30 and the fact that physical activity is known to affect fatty acid composition,31 the finding was not necessarily surprising. However, further examination of those data12 suggested that the low-dose treatment group actually experienced the greatest attenuation in head trauma. Human trials are lacking, but an inherent limitation in the study of head trauma in humans is the heterogeneity of injury. The risks of increasing DHA intake are virtually nonexistent.11 Further, considering the low incidence of proper concussion reporting32 and the presence of a pathophysiological response even in the absence of a concussion,33 increasing intake should be strongly considered, particularly given our findings.
The fact that the football athletes in the current study had Omega-3 indexes below the desirable range was not necessarily surprising. Using a similar method and exploratory approach, von Schacky et al34 reported that only 1 endurance athlete out of 106 had a desirable Omega- 3 Index. Dietary sources of EPA and DHA are limited, with certain microalgae at the base of the marine food chain being the primary producers. Fish that consume these nutrients are thus the richest source in the human diet. This may at last partially explain why worldwide consumption is low.3 In the United States, the estimated combined intake of DHA and EPA is only about 100 mg-dW In contrast, Americans generally consume diets much higher in the m-3 FA ALA35; as previously noted, although ALA can be metabolically converted to EPA and DHA, conversion is limited, especially in men.2
In this retrospective descriptive study, our lack of dietary assessment, including supplemental intake, was a limitation. Without dietary information, we were unable to discern if the low Omega-3 Index, an indicator of an individual’s EPA + DHA status, was due to a diet low in m3 FA or a high rate of turnover, but the average intakes noted above for Americans in general probably apply to young male athletes as well.
CONCLUSIONS
Using a simple, minimally invasive method, we observed that football athletes may be deficient in the m-3 FAs EPA and DHA. Although further study is warranted to determine if the deficiency is indeed due to diet and not physical activity, the likelihood of the latter is unlikely given similar reports among athletes and the United States at large. Regardless of the cause of these low levels, efforts to increase tissue EPA and DHA levels in athletes should be considered because football athletes may experience unique health concerns, including an increased risk of CVD and exposure to repetitive head impacts. Whether this would include promoting increased consumption of oily fish (salmon, mackerel, sardines, etc) or the use of m-3 supplements (or both) is a topic for further discussion. In either case, the risks of increasing EPA and DHA intake are virtually nonexistent,11 and the potential benefits appear to be substantial.