How should Vitamin D be tested – a changing landscape
Assessment of vitamin D status - a changing landscape
DOI 10.1515/cclm-2016-0264, Received April 1, 2016; accepted May 30, 2016
Markus Herrmann*, Christopher-John L. Farrell, Irene Pusceddu, Neus Fabregat-Cabello and Etienne Cavalier
Corresponding author: Prof. Dr. med. habil. Markus Herrmann, FRCPA, Department of Clinical Pathology, Bolzano Hospital, Lorenz Boehler Str. 5, 39100 Bolzano, Italy, Phone: +39 0471 909675, markus.herrmann@sabes.it
Christopher-John L. Farrell: Laverty Pathology, Sydney, NSW, Australia
Irene Pusceddu: Department of Clinical Pathology, Bolzano Hospital, Italy. http://orcid.org/0000-0001-8197-3936
Neus Fabregat-Cabello and Etienne Cavalier: Department of Clinical Chemistry, University of Liege, CHU Sart-Tilman, Domaine du Sart- Tilman, Liege, Belgium
📄 Download the PDF from VitaminDWiki
Figure 1

Abstract: In recent years it has been shown that vitamin D deficiency is associated with an increased incidence as well as the progression of a broad range of diseases including osteoporosis, rickets, cardiovascular disease, autoimmune disease, multiple sclerosis and cancer. Consequently, requests for the assessment of vitamin D status have increased dramatically. Despite significant progress in the analysis of vitamin D metabolites and an expansion of our pathophysiological knowledge of vitamin D, the assessment of vitamin D status remains a challenging and partially unresolved issue. Current guidelines from scientific bodies recommend the measurement of 25-hydroxy vitamin D (25-OHD) in blood as the preferred test. However, growing evidence indicates significant limitations of this test, including analytical aspects and interpretation of results. In addition, the relationships between 25-OHD and various clinical indices, such as bone mineral density and fracture risk, are rather weak and not consistent across races. Recent studies have systematically investigated new markers of vitamin D status including the vitamin D metabolite ratio (VMR) (ratio between 25-OHD and 24,25-dihydroxy vitamin D), bio- available 25-OHD [25-OHD not bound to vitamin D binding protein (DBP)], and free 25-OHD [circulating 25-OHD bound to neither DBP nor albumin (ALB)]. These parameters may potentially change how we will assess vitamin D status in the future. Although these new biomarkers have expanded our knowledge about vitamin D metabolism, a range of unresolved issues regarding their measurement and the interpretation of results prevent their use in daily practice. It can be expected that some of these issues will be overcome in the near future so that they may be considered for routine use (at least in specialized centers). In addition, genetic studies have revealed several polymorphisms in key proteins of vitamin D metabolism that affect the circulating concentrations of vitamin D metabolites. The affected proteins include DBP, 7-dehydrocholesterol synthase and the vitamin D receptor (VDR). Here we aim to review existing knowledge regarding the biochemistry, physiology and measurement of vitamin D. We will also provide an overview of current and emerging biomarkers for the assessment of vitamin D status, with particular attention methodological aspects and their usefulness in clinical practice.
Introduction
Vitamin D deficiency is a common problem in numerous populations worldwide [1]. Besides its role in calcium and phosphate metabolism, recent studies have provided evidence for a role of vitamin D in vascular, inflammatory, neoplastic and neurodegenerative diseases [2]. The growing awareness in the medical community that vitamin D deficiency affects large parts of the population and that the consequent health effects go far beyond bone loss and osteoporosis have triggered an exponential increase in vitamin D testing [3].
Current guidelines from scientific bodies around the globe recommend the measurement of 25-hydroxy vitamin D (25-OHD) in blood as the preferred test for the assessment of vitamin D status [4, 5]. This recommendation is based on numerous studies that have demonstrated significant associations of 25-OHD with biochemical, functional and clinical indices, such as parathyroid hormone (PTH), neuromuscular function, bone mineral density (BMD) and fracture risk [6-9]. However, closer examination of the data from these studies reveals that many of these relationships are not as strong as one might expect and are not consistent across different populations. For example, African Americans have lower 25-OHD concentrations than their White counterparts, but have significantly lower rates of osteoporotic fracture [10, 11]. Furthermore, individuals with a low 25-OHD may have normal PTH [12]. With our current understanding of vitamin D metabolism we are not able to explain such observations and one may ask if 25-OHD is really the best marker of vitamin D status. A number of recent studies have provided new insights in physiological and analytical aspects of vitamin D. Here we aim to review existing knowledge regarding biochemistry, physiology and measurement of vitamin D.
Vitamin D metabolism
Vitamin D refers to a group of fat-soluble secosteroids that are derived from cholesterol. Secosteroids are characterized by a broken bond in one of the steroid rings. To date, more than 50 different vitamin D metabolites with variable biological activity have been described [13]. The two major forms of the vitamin are D3 (cholecalciferol) and D2 (ergocalciferol), which differ in the structure of their side chains. The side chain of vitamin D2 differs from that of vitamin D3 by the presence of a double-bond between carbons 22 and 23 and a methyl group on carbon 24 [14]. Vitamin D3 is the form of the vitamin synthesized by humans. Both vitamin D3 and D2 may be obtained in small amounts from the diet, or in more significant quantities from fortified foods or vitamin supplements [15].
Vitamin D metabolism is a complex process involving the action of UV radiation and hydroxylation steps in both synthesis and catabolism. The predominant source of vitamin D in humans is production in the skin by synthesis from 7-dehydrocholesterol through the action of UV light. 7-Dehydrocholesterol, also referred to as provitamin D, is an intermediate in the cholesterol synthetic pathway, formed by the penultimate step of cholesterol biosynthesis. Cholesterol is essential for maintenance of the epidermal barrier function, and also has a role in the regulation of epidermal differentiation and desquamation [16, 17]. The epidermis is therefore an active site of de novo cholesterol synthesis, which provides a ready source of 7-dehydrocholesterol [18]. 7-Dehydrocholesterol is present in the plasma membrane of cells in both the dermis and epidermis [19], with the highest concentrations in the cells of the stratum basale and stratum spinosum layers of the epidermis [20].
Synthesis of vitamin D in the skin commences when 7-dehydrocholesterol absorbs UVB radiation with a wavelength between 290 and 315 nm. Absorption of this energy breaks the bond between carbons 9 and 10 to form an unstable 9, 10 seco-steroid, known as previtamin D3 [21]. The removal of this bond allows previtamin D3 to spontaneously rotate around the bond between carbons 5 and 6, which forms a more thermodynamically stable isomer, vitamin D3. The molecular interactions of the previtamin D3 with the lipid bilayer of the cell membrane helps to hold the previtamin D3 in a conformation (s-cis, s-cis) that facilitates this isomerization process, which has a half-life in vivo of 2.5 h [21, 22]. The isomerization process interrupts the hydrophobic and hydrophilic interactions that hold the molecule within the cell membrane and isomerization therefore expels the vitamin D3 into the interstitial fluid [23]. The presence of vitamin D binding protein (DBP) in the capillaries of the dermis maintains a concentration gradient of free vitamin D that favors the movement of vitamin D from the interstitial fluid into the circulation [24].
Although UV radiation is essential for vitamin D synthesis, it may also be responsible for its inactivation. If either previtamin D or vitamin D are exposed to further UV radiation before they reach the circulation, they are converted into biologically inactive species. The action of UV light on previtamin D3 produces the photodegradation products lumisterol3 and tachysterol3, while vitamin D is inactivated into 5,6-trans-vitamin D3, suprasterol 1 or suprasterol 2 [25]. These UV degradation processes reach significant activity with prolonged UV exposure times and, therefore, provide a mechanism preventing vitamin D toxicity under these circumstances [26]. A single episode of UV exposure may convert as much as 15% of the 7-dehydrocholesterol present in the skin into previtamin D3; however, once this threshold is reached additional previtamin D3 is not produced, rather there is increased production of luminsterol and tachysterol [26].
Vitamin D may also be obtained directly from the diet. Fatty fish, fish liver oil and egg yolk naturally contain the highest concentrations of vitamin D [27]. In some regions, the fortification of food, such as milk and margarine, may also contribute significantly to dietary vitamin D intake [15]. Variation exists in the amount of vitamin D obtained from the diet both between and within populations; however, in Western populations dietary sources generally represent only 10%-20% of total vitamin D intake [28, 29].
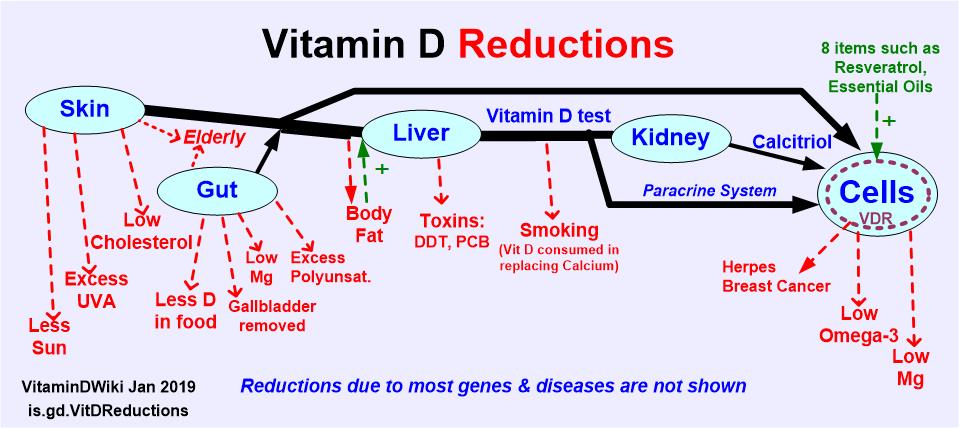
Two hydroxylation reactions are required to convert vitamin D into a biologically active form (Figure 1). The first hydroxylation occurs on the carbon 25 and is primarily performed by the cytochrome P450 enzyme CYP2R1, although other P450 enzymes are capable of catalyzing this hydroxylation, including CYP27A1, CYP3A4 and CYP2D5 [30-32]. The 25-OHD thus produced may then undergo hydroxylation at the one carbon position in the proximal tubules of the kidney under the action of the cytochrome P450 enzyme CYP27B1. It has been found that 1-hydroxylation also occurs in many extra-renal tissues, including bone, placenta, prostate, keratinocytes, macrophages, T-lymphocytes, epithelial cells of the colon, islet cells of the pancreas and several cancer cells (including those from lung, prostate and skin) as well as cells of adrenal medulla, cerebral and cerebellar cortex [32, 33]. It appears that the 1,25-(OH)2D produced by extra-renal tissues acts locally as an autocrine or paracrine signaling molecule as does not contribute significantly to circulating 1,25-(OH)2D concentrations [34].
Vitamin D2
Vitamin D2 (ergocalciferol) may be synthesized in plants and fungi by the action of UV light on ergosterol [14]. A small amount of vitamin D2 may be obtained from a natural diet. Wild-grown mushrooms are particularly rich sources of vitamin D2. In contrast, cultivated mushrooms contain little vitamin D2; but levels do increase if they are exposed to UV light during processing [35]. Vitamin D2 may be synthesized for use in supplements by exposing ergosterol in yeast to UV radiation.
Vitamin D2 undergoes identical activation steps to vitamin D3, which are mediated by the same enzymes. Therefore, in subjects regularly taking vitamin D2-con- taining supplements, a significant proportion, or even the majority, of the total circulating 25-OHD and 1,25-(OH)2D is in the D2 form [36]. Supplementation with vitamin D2 has generally been considered equivalent to vitamin D3 supplementation; however, variations in vitamin D2’s metabolic properties and binding affinity for DBP may mean that it is less effective in increasing systemic 25-OHD levels [37, 38].
Vitamin D metabolism
Figure 1: Vitamin D metabolism and assessment.
In the liver vitamin D is hydroxylated in 25-hydroxy-vitamin D (25-OHD) by the enzyme CYP2R1. Subsequently, 25-OHD is hydroxylated to bioactive 1a,25-dihydroxy-vitamin D (1,25-(OH)2D) by the enzyme CYP27B1, predominantly in the kidney. Vitamin D catabolism is predominantly due to CYP24A1, which metabolises 25-OHD to 24,25-dihydroxy-vitamin D (24,25-OH2D) and 1,25-(OH)2D to 1,24,25-dihydroxy-vitamin D (1,24,25-OH3D). Circulating vitamin D is bound to carriers (vitamin D binding protein (DBP), albumin and lipoproteins). Bioavailable vitamin D (BAVD), vitamin D metabolite ratio (VMR), automated immunoassay (automated IA).
C3-Epimer forms
C3-Epimers of vitamin D metabolites are molecules with identical structure to the primary molecule but differ in stereochemical configuration. The dominant epimer form of vitamin D, C3-epimer-25-OHD3 (3-epi-25-OHD3), differs in the position of the hydroxyl group at the three carbon position of the molecule. Similar to the primary molecule, 3-epi-25-OHD3 can undergo 1a-hydroxylation to form 3-epi-1,25-(OH)2D3, bind to DBP and the vitamin D receptor (VDR) and activate gene transcription [39, 40]. However, the affinity of 3-epi-25-OHD3 and 3-epi-1,25-(OH)2D3 to both proteins is significantly lower compared to the respective non-epimeric form [15]. While 3-epi-1,25-OH-D effectively suppresses PTH, it has significantly reduced calcemic effects [39, 40].
The presence of a significant amount of C3-epimer was first reported in children under 1 year of age, where it represented an average of 23% of the total 25-OHD [39, 40]. In our own subsequent study, we demonstrated that 3-epi- 25-OHD3 is detectable (>5 nmol/L) in 41% of samples from healthy adults. Another study using an LC-MS/MS method with a lower limit of quantification detected 3-epi-25OHD3 (>2.5 nmol/L) in 99% of healthy subjects with an age range from neonates to >80 years [40]. However, the observed range of 3-epi-25-OHD3 concentrations was very wide (2.559.3 nmol/L). 3-epi-25-OHD3 concentrations correlate with 25-OHD3 concentrations in a non-linear fashion: a greater amount of 3-epimer is seen at higher 25-OHD3 concentrations. Cross-reactivity of C3-epimer-25-OHD3 has been suggested as a potential source of interference in total 25-OHD immunoassays. However, Farrell et al. demonstrated that C3-epimer-25-OHD3 is a minor contributor to inaccuracies in these assays. Other metabolites, such as 25-OHD2 seem to have a much greater impact on total 25-OHD measurement [41].
Vitamin D binding protein
Transport of the various vitamin D species in serum is provided by a specific protein, DBP. DBP is structurally related to albumin (ALB) and binds all naturally occurring, as well as synthetic, vitamin D species at a single cleft-like binding site [42]. DBP provides a high-affinity, high-capacity binding protein for vitamin D species, carrying 95%-99% of the total 25-OHD, with the remainder circulating in association with ALB and lipoproteins via weak, non-specific binding [43]. DBP has highest affinity for 25-OHD, 24,25-OH2D and 25,26-OH2D. Its affinity for 1,25-(OH)2D is about 10- to 100-fold lower than these species, while its affinity for the parent vitamin D molecule is lower still [43]. Vitamin D2 metabolites bind similarly but slightly less well to DBP than their D3 counterparts [43].
Vitamin D catabolism
Similar to vitamin D activation, the catabolism of vitamin D largely occurs via hydroxylation in the kidney. The primary catabolic pathway in humans commences with 24-hydroxylation and culminates in the formation of cal- citroic acid, which is excreted in the bile. The mitochondrial P450 enzyme, CYP24A1, catalyzes the first step, and possibly some subsequent steps, of this pathway [44]. The preferred substrate for CYP24A1 is1,25-(OH)2D, but the enzyme is also active in metabolising 25-OHD to 24,25- (OH)2D [45, 46]. 24,25-(OH)2D has been measured in the circulation at concentrations up to 10 ng/mL and, although it is a catabolic metabolite, it may have some biological activity, such as in modulating growth plate chondrocyte physiology and parathyroid gland function [46, 47].
A number of minor catabolic pathways for vitamin D also exist, some producing intermediates with biological activity. In some instances, CYP24A1 enzyme activity may catalyze hydroxylation on carbon 23 rather than carbon 24 as the first catabolic step. In humans, this occurs at about 10% of the rate of 24-hydroxylation [44]. An initial 23-hydroxylation marks the vitamin D molecule for metabolism via a pathway which culminates in the production of 1,25-(OH)2D-26,23-lactone. In addition, human CYP24A1 is able to catabolize vitamin D2 species through a series of hydroxylation reactions, including at carbons 24, 26 and 28, as well as direct cleavage of the bond between carbons 24 and 25 [48].
Maintenance of homeostasis
The crucial control point in vitamin D homeostasis is the renal production of 1,25-(OH)2D via 1a-hydroxylase. A number of factors act to regulate this step. 1,25-(OH)2D acts to decrease its own production through both direct and indirect mechanisms. 1,25-(OH)2D acts directly to negatively feedback on the expression of 1a-hydroxylase [49]. 1,25-(OH)2D also decreases PTH synthesis [50]. PTH is responsible for increasing 1a-hydroxylase transcription; therefore, the effect of 1,25-(OH)2D on PTH provides an indirect mechanism by which 1,25-(OH)2D down-regulates its production [49]. Rising concentrations of 1,25-(OH)2 D also increase the expression of the phosphaturic factor, fibroblast growth factor 23 (FGF23) [51]. FGF23 suppresses the expression of 1a-hydroxylase in the kidney, providing another indirect pathway of 1,25-(OH)2D acting to down- regulate its production [52]. In addition, dietary calcium and phosphate intake influence 1a-hydroxylase activity: increasing intakes reduce 1a-hydroxylase activity [53].
The expression of the catabolic enzyme CYP24A1 in the kidney provides another control point in vitamin D homeostasis. 1,25-(OH)2D and FGF23 cause up-regulation of expression of CYP24A1, while raised PTH and low calcium down-regulate expression [53, 54].
Several physiological and pathological conditions are related to an individual’s vitamin D status. For example, individuals with chronic inflammatory conditions, such as asthma, inflammatory bowel disease or chronic obstructive pulmonary disease, have a higher prevalence of vitamin D deficiency [55]. However, at present it is controversial whether 25-OHD reduces inflammation or whether inflammation reduces 25-OHD concentrations. It is possible that both mechanisms are active and not mutually exclusive: vitamin D may decrease inflammation, while oxidative stress from inflammation may interfere with the metabolism of vitamin D and thus lower 25-OHD [56]. Randomized controlled trials of vitamin D have given inconsistent results. Whereas some studies showed no effect, others reported mixed or beneficial effects. A few studies even reported adverse effects of vitamin D supplementation [56]. However, comparing these studies is difficult as they differ substantially in terms of study population, assessment of inflammation and modalities of vitamin D supplementation.
Another frequent condition that impacts on circulating 25-OHD is pregnancy. Pregnant women are at risk of developing vitamin D deficiency, which in turn is associated with an increased risk of pre-eclampsia, a condition associated with increased maternal and perinatal morbidity and mortality [57]. However, the cause of vitamin D deficiency in pregnancy is still a matter of debate. Reduced dermal production, increased consumption, hemodilution and an altered hepatic DBP production are potential explanations. In light of these influences, it is important to consider the patient’s general health status when interpreting vitamin D results.
Autocrine/paracrine physiology of vitamin D
Interest in the role of vitamin D beyond bone health was sparked by the identification of the VDR in diverse cell types unrelated to calcium metabolism, including immune cells (such as macrophages, activated T and B lymphocytes and dendritic cells), enterocytes, myocytes, neurons and glial cells of the central nervous system [2, 58-60]. Further work has suggested that 1,25-OH2D acts as an autocrine or paracrine signaling molecule in these tissues, with a distinct physiology in terms of metabolism, regulation and actions. 1,25-OH2D may be synthesized and catabolized locally by most of the cell types expressing VDR. Synthesis is achieved by the expression of the CYP27B1 enzyme, which converts 25-OHD from the systemic circulation into 1,25- OH2D [61]. Unlike its expression in the kidneys, CYP27B1 in extra-renal tissues is not influenced by calcemic factors, but instead responds to cell-specific regulatory factors [61]. For example, CYP27B1 expression in macrophages is increased by inflammatory signaling molecules such as interferon-y and lipopolysaccharide [62, 63]. The expression of CYP27B1 in keratinocytes is similarly up-regulated by inflammatory intermediates, but expression is also controlled by the cell’s stage of development [64, 65].
Extra-renal tissues are also able to catabolize 1,25- OH2D locally. This is accomplished by expression of CYP24A1. Exposure to VDR agonists up-regulates the expression of CYP24A1 in these tissues [66]. This provides a mechanism for switching off the autocrine/paracrine 125 OH2D signal locally and also means that 1,25-OH2D produced in these tissues will not contribute to the circulating concentration [67, 68].
The actions of 1,25-OH2D produced in extra-renal tissues are many and diverse. Indeed, vitamin D is involved in the cell-specific regulation of over 200 genes [2, 69]. Examples of genomic 1,25-OH2D actions include multiple immune function responses, control of cell proliferation, differentiation and apoptosis, and regulation of both angiogenesis as well as pathways responsible for central nervous system detoxification and anti-oxidation [70]. Additionally, 1,25-OH2D may elicit non-genomic cellular actions through VDR located within cell membranes activating a variety of second messengers [70]. This effect has been observed in parathyroid cells, hepatocytes, chondrocytes and epithelial cells [70-74].
Assessment of vitamin D status
The many different metabolites of vitamin D vary greatly in their biological activity. Compared to vitamin D3, 1,25- (OH)2D3 is approximately five times more active in regard to intestinal calcium absorption [75, 76] and mobilization of calcium from bone [77, 78]. One important determinant of the biological activity of vitamin D metabolites is their affinity for the VDR. Receptor assays with chicken intestine have shown the highest affinity for 1,25-(OH)2D3 [78]. The affinity of all other metabolites is dramatically lower; for instance, 900 times lower for 25-OHD and 5000 times lower for 24,25-OH2D3. Therefore, it is not surprising that blood concentrations of all these vitamin D metabolites vary dramatically. In non-supplemented individuals the concentration of 1,25-(OH)2D3 is typically in the low pico-molar range whereas 25-OHD can reach up to 100200 nmol/L. In view of the multiple metabolites and their variable biological activity the question arises: what is the best test to assess an individual’s vitamin D status?
25-hydroxy vitamin D and 1,25-dihydroxy vitamin D
Current guidelines recommend using the serum circulating 25-OHD level, measured by a reliable assay, to evaluate vitamin D status in patients who are at risk for vitamin D deficiency [79]. 25-OHD is the most abundant vitamin D metabolite in the circulation and is considered the best indicator of vitamin D status. There is solid evidence that serum 25-OHD is associated with clinical outcomes, such as bone mineralization, fracture risk, falls risk, all-cause mortality and cardiovascular events [80-84]. Because of a long half-life of 2-3 weeks, serum levels vary very little within short periods of time. Furthermore, 25-OHD represents the sum of vitamin D intake and dermal production [85]. Serum 25-OHD levels show a significant response to both sun exposure, as evidenced by the seasonal variation of levels, as well as to vitamin D supplementation [81, 86-91].
25-OHD may also be the preferred marker of the ability of tissues to produce complete 1,25-OH2D autocrine/paracrine vitamin D signals in response to cell-specific stimuli. It is thought that the production of 1,25-OH2D in extra-renal tissues is more dependent on the circulating 25-OHD concentration than this process in the kidneys [61]. Measurement of the circulating 1,25-OH2D concentration does not provide an alternative marker of the autocrine/paracrine activity of vitamin D because the 1,25-OH2D produced by this system does not reach the systemic circulation [68].
Existing guidelines unanimously recommend against using serum 1,25-(OH)2D3 in the routine assessment of vitamin D status because it does not reflect vitamin D reserves. PTH, calcium, FGF-23 and phosphate tightly regulate its blood concentration. The utility of 1,25-(OH)2D3 in the evaluation vitamin D status limited because vitamin D deficient individuals frequently develop secondary hyperparathyroidism which induces renal 1a-hydroxylase expression. As a result, the serum
(OH)2D3 concentration of vitamin D deficient individuals is often normal and may even be elevated [92]. Another limitation is the short half-life of circulating 1,25-(OH)2D3 of approximately 4 h, which results in significant intraindividual variability. From an analytical point of view, 1,25-(OH)2D is a challenging analyte to measure as circulating levels are a 1000 times lower than 25-OHD. In fact, it is only recently that automated assays have become available. Additionally, there is neither an internationally accepted reference material nor a reference method. Measurement of 1,25-(OH)2D3 is considered useful only in the context of acquired or inherited disorders of vitamin D and phosphate metabolism, such as chronic kidney disease, hereditary phosphate-losing disorders, oncogenic osteomalacia, pseudovitamin D-deficiency rickets, vitamin D-resistant rickets, as well as chronic granuloma forming disorders such as sarcoidosis and some lymphomas [78, 85, 93-97].
On close inspection of the published data, the relationships between 25-OHD and various indices of bone health are relatively weak [98-100] and not consistent across races [101]. For example, in an observational study of 414 elderly Californian men, serum 25-OHD did not correlate with serum PTH (r=-0.05, p=0.3) [100]. In the same study, although serum 25-OHD was shown to be significantly associated with BMD at hip and spine, the regression coefficients were rather low (r=0.0003 for BMD at the hip; r=0.001 for BMD at the spin). In the MINOS study (881 men aged 19-85 years), biochemical markers of bone turnover and BMD did not correlate with serum 25-OHD in men under 55 years of age [102].
The relationship between 25-OHD and both bone and cardiovascular outcomes is even weaker for Black Americans than it is for White Americans [103, 104]. In fact, a nested case control study within the prospective Women’s Health Initiative Observational Study found that among Black women as serum 25-OHD concentrations increased, so did their risk of fracture [105]. In contrast, the study confirmed the expected inverse relationship between 25-OHD concentration and fracture risk in White women. Studies have also shown differences in the relationship between 25-OHD and PTH in Black compared to White subjects. While Blacks have serum concentrations of 25-OHD approximately 30% lower than Whites [106-108], this is not associated with a proportional increase in PTH. When considering individuals with comparable PTH concentrations, serum 25-OHD is again significantly lower in Blacks than in Whites.
Considering the inconsistent data a general screening for vitamin D deficiency is not recommended by current guidelines. Most scientific bodies recommend testing 25-OHD in individuals at risk for vitamin D deficiency including individuals with rickets, osteoporosis, osteomalacia, chronic kidney disease, hepatic failure, malabsorption syndromes, hyperparathyroidism and granuloma-forming disorders [79]. In addition 25-OHD testing is recommended for subjects on medication known to alter vitamin D metabolism (antiepileptics, HIV drugs and antifungals) and older adults with a history of falls and non-traumatic fractures [79]. Although not yet supported by official guidelines we believe that for persons of African descent separate cutoffs should be adopted as they have a constituently lower 25-OHD concentration due to their lower DBP concentration. There is no evidence that the lower 25-OHD concentration in Blacks is equally associated with an increased risk for bone health than in Whites.
Bioavailable vitamin D, 24,25-dihydroxy vitamin D and vitamin D metabolite ratio
As a response to the limitations of 25-OHD, it has been speculated that other surrogate markers of vitamin D metabolism might better reflect pathophysiology and predict clinical outcome [109, 110]. Some of these markers are illustrated in Figure 1. One such marker is bioavail- able vitamin D (BAVD). BAVD is the fraction of vitamin D that is not bound to DBP and thus can cross the cell membrane where it becomes available for enzymatic conversion into biologically active 1,25-(OH)2D3 or 24,25-(OH)2D, the first metabolite in vitamin D catabolism. Although the concept of BAVD was described 30 years ago [109], its physiological significance is incompletely understood. The main reason for this lack of knowledge is the absence of a reliable method for measurement. Most publications that reported bioavailable vitamin D results used a mathematical approach where bioavailable vitamin D is calculated using 25-OHD, DBP and ALB concentrations. This approach is similar to the estimation of free testosterone. In the Across the Life Span (HANDLS) Study Powe et al. observed comparable concentrations of BAVD in Blacks and Whites despite significant differences in total 25-OHD measured by liquid chromatography tandem mass spectrometry (LC-MS/MS; interassay coefficient of variation CV: 8.6%), a finding largely explained by approximately 50% lower DBP concentrations in Blacks [106]. BAVD was calculated using DBP results obtained by a monoclonal immunoassay from R&D; Systems. The study concluded that the race differences in DBP concentration resulted from single nucleotide polymorphisms (SNPs). rs7041 and rs4588 were major determinants of the DBP concentration in serum in their cohort. One allele copy of rs7041 reduced DBP by 189 pg/mL whereas one allele copy of rs4588 increased DBP by approximately 50 pg/mL. However, the monoclonal immunoassay from R&D; Systems used in this study appears to be sensitive to DBP polymorphisms [110]. The aforementioned polymorphisms result in protein variants with different affinities to the monoclonal antibodies used in R&D; Systems assay. In a more recent study from Henderson et al. DBP was measured with a LC-MS/MS method demonstrated to reliably detect the common DBP variants [110]. With this method, comparable DBP concentrations were measured in Blacks and Whites. In addition, the authors could demonstrate that their assay reliably detects common isoforms. When they compared their assay with the R&D; Systems monoclonal immunoassay, slope, intercept and regression coefficients varied substantially between the different DBP genotypes. Two very recent studies confirmed a strong dependence of calculated free 25-OHD results on the assay used for quantitation of DBP in Black individuals [111, 112]. In both studies different polyclonal DBP immunoassays yielded comparable results. However, the monoclonal ELISA from R&D; Systems returned substantially lower concentrations. Such discrepancies were not observed in Whites. Considering the variable performance of the different DBP assays, BAVD results are poorly comparable between studies. Therefore, further clinical studies with validated DBP and 25-OHD assays are needed to understand the true potential of BAVD as a biomarker of vitamin D status and metabolism.
While the analysis of protein-based markers of vitamin D status is still problematic due to a number of technical issues, measurement of certain vitamin D metabolites might be an alternative way to improve the assessment of vitamin D metabolism. A vitamin D metabolite that has recently gained much attention is 24,25-OH2D, the major product of 25-OHD catabolism. The conversion of 25-OHD into 24,25-OH2D is catalyzed by the 24-hydroxylase enzyme (CYP24A1) [44]. Considering there is direct enzymatic conversion of 25-OHD into 24,25-OH2D it is not surprising that the concentrations of both compounds are strongly correlated [113]. In contrast to DBP, this correlation is comparable across different races (Blacks: r=0.86, p<0.001; Whites: r=0.90, p<0.001) [107]. 24,25-OH2D possesses some conceptual advantages over DBP, BAVD and 25-OHD. Its serum concentration strongly depends on the availability of 25-OHD and the expression of CYP24A1. CYP24A1 is, at least in part, regulated by VDR [112, 114]. Therefore, when sufficient amounts of biologically active vitamin D are available CYP24A1 is up-regulated and more 24,25-OH2D is formed. Calculating the ratio between serum 24,25-OH-2D and 25-OHD may improve assessment of vitamin D status. This ratio is referred to as the vitamin D metabolite ratio (VMR).
When 24,25-OH2D is considered in isolation, associations with PTH are similar to those observed with 25-OHD including the differences between Blacks and Whites. In contrast, the relationship between VMR and PTH is similar in Whites and Blacks. In the view of lower 25-OHD levels and higher BMD in Blacks than in Whites it appears that VMR better reflects the metabolic situation in individuals with African background than the measurement of a single metabolite. Several studies have shown that VMR decreases in individuals with low serum 25-OHD or functional vitamin D deficiency. For example, in renal patients, where the conversion of 25-OHD into 1,25-(OH)2D3 is disturbed, the formation of 24,25-OH2D decreases with decreasing eGFR in a non-linear fashion, whereas 25-OHD measured by LC-MS/MS (interassay CV: 4.4%) is not correlated with eGFR [46]. Furthermore, 24,25- (OH)2D, which has also been measured by LC-MS/MS, shows a much stronger correlation with PTH (r=-0.44, p<0.001) than 25-OHD (r=-0.22, p<0.001) or 1,25-(OH)2D (r=-0.16, p=0.01). These results have been confirmed by a recent study of 9596 patients from five different studies that analyzed 25-OHD and 24,25-(OH)2D by LC-MS/MS [113]. Consistent with the concept of altered vitamin D metabolism in renal patients, Stubbs et al. showed that during 8 weeks of cholecalciferol supplementation there was a significantly smaller rise in 24,25-(OH)2D and VMR in CKD patients than in controls despite a similar increase in 25-OHD (measured LC-MS/MS, interassay CV: <10.7%) [115]. A potential value of VMR in monitoring the effectiveness of vitamin D supplementation has also been shown by others [116].
From an analytical point of view, 24,25-(OH)2D has also some advantages over DBP and BAVD. At present, measurement is only possible with LC-MS/MS based methods. As proteins are typically eliminated during sample preparation the measurement of 24,25-(OH)2D by LC-MS/MS is not affected by DBP or other matrix proteins. In addition, the high specificity of LC-MS/MS technology minimizes the problem of cross-reactivity with other, often more abundant, metabolites. However, highly sensitive mass spectrometers are needed for analysis as human serum concentrations of 24,25-(OH)2D are in the very low nano-molar range.
The main limitation of 24,25-(OH)2D and VMR is the lack of data relating to clinically relevant outcomes, such as BMD, fracture risk, mortality, cardiovascular disease and others. Future studies will have to clarify if the conceptual advantages of 24,25-(OH)2D and VMR analysis can be confirmed in various clinical situations.
In conclusion, DBP, BAVD and VMR are promising emerging biomarkers that may provide additional information to 25-OHD in assessing vitamin D status and metabolism. At present, only very few studies have addressed the clinical utility of these biomarkers. When assessing the diagnostic performance of 25-OHD and related metabolites, the variable performance of immunoassays needs to be considered. Diagnostic inferiority of one vitamin D metabolite compared to another may be exclusively due to analytical rather than biological reasons. This is particularly relevant for 25-OHD and DBP. More detailed methodological information about 25-OHD assays and methods for the measurement of related vitamin D metabolites is provided in “Measurement of vitamin D metabolites - analytical aspects”. Because of the limited data and the aforementioned technical issues, the use of these emerging markers of vitamin D status in clinical practice is not yet justified. Should future clinical studies confirm a superior diagnostic performance of DBP, BAVD or VMR, or should they provide additional relevant information, it is likely that one or more of these marker will make their way into clinical practice. Further research to confirm and elucidate the basis of these findings could also enhance our understanding of ethnic differences in fracture risk.
Single nucleotide polymorphisms
Sociocultural and lifestyle factors are important determinants of a person’s vitamin D status, mainly through their effects on sun exposure and dietary uptake of vitamin D. Seasonal variation, geographical latitude and supplementation are additional factors that impact the serum concentration of 25-OHD. However, a significant fraction of inter-individual variability in serum 25-OHD is not explained by these factors. Epidemiological studies provide robust evidence that genetic factors contribute substantially to an individual’s vitamin D status [117-126]. Differences in the prevalence of vitamin D deficiency among different ethnic groups can be explained at least in part by genetic variants that affect vitamin D metabolism. For example, it has been long recognized that genetic variants of the DBP lead to different phenotypes of the protein with different affinities to 25-OHD and 1,25-(OH)2D3 [120]. Furthermore, genetic polymorphisms of DBP can also alter the protein concentration in blood [106]. This results in significantly different serum 25-OHD concentrations.
Meta-analyses of genome-wide association studies (GWAS) in Europeans have identified single-nucleotide polymorphisms (SNPs) in genes involved in cholesterol synthesis, hydroxylation, and vitamin D transport that affect vitamin D status [117, 118]. The meta-analysis by Wang et al. included GWAS data of 33,996 Europeans from 15 cohorts [118]. The strongest associations were observed for genetic polymorphisms in the following genes: GC (encoding DBP), DHCR7 (encoding 7-dehydrocholesterol reductase) and CYP2R1 (encoding cytochrome P450 family 2, subfamily R, polypeptide 1).
The two most frequently studied variants of the GC gene are the SNPs that change the amino acid sequence of the protein, rs7041 (Asp-Glu) and rs4588 (Thr-Lys) [120, 127, 128]. For example, Lauridsen et al. analysed plasma from 959 postmenopausal women and found that the median concentration of 25-OHD as well as the mean concentration of 1,25-(OH)2D3 differed significantly depending on GC phenotype, being highest in Gc1-1 (CC rs4855; GG rs7041), intermediate in Gc1-2 (CC rs4588; TT rs7041), and lowest in Gc2-2 (AA rs4588; TT rs7041) [120]. In addition, the plasma concentration of DBP is significantly higher in Gc1-1, intermediate in Gc1-2 and lowest in the Gc2-2 phenotype [120]. The Gc phenotypes differ in amino acid sequence and in glycosylation. Gc1 is glycosylated with galactose and sialic acid, whereas Gc2 contains only galactose. Considering the glycosyla- tion pattern, Gc2 is metabolized faster [129], explaining the lower concentrations of vitamin D in these subjects. The Gc (rs2282679) polymorphism, located within intron 12 and near the Gc (rs4588) polymorphism, showed the strongest association with vitamin D deficiency in the two GWAS meta-analyses by Wang and Ahn [117, 118]. The average serum 25-OHD concentration in individuals with the major homozygous genotype (A:A) and the minor homozygous genotype (C:C) differ by 8-18 nmol/L. The odds of having vitamin D deficiency increases by 61% per copy of the risk allele [118].
7-Dehydrocholesterol reductase, the gene product of the DHCR7 gene on chromosome 11, converts 7-dehydrocholesterol (primary substrate of vitamin D synthetic pathway) to cholesterol. This reaction determines the availability of 7-dehydrocholesterol for the synthesis of vitamin D. Genetic variants of the DHCR7 gene have also been shown to impact circulating 25-OHD levels [117, 118]. DHCR7(rs12785878), located within intron 2 is the most relevant SNP of the DHCR7 gene. However, the effect on circulating 25-OHD is less pronounced than that of Gc(rs2282679). The average serum 25-OHD concentration in individuals with the major homozygous genotype (A:A) and the minor homozygous genotype (G:G) differs by 4-8 nmol/L. The odds of having vitamin D deficiency increase by 21% per copy of the risk allele [118].
The GWAS meta-analyses by Wang and Ahn identified the CYP2R1 (rs10741657) polymorphism as another genetic determinant of the serum 25-OHD concentration [117, 118]. This gene encodes a hepatic microsomal enzyme responsible for the 25-hydroxylation of vitamin D in the liver. The G allele is associated with a lower serum 25-OHD concentration. The median serum 25-OHD concentration in G:G carriers is 4-6 nmol/L lower than in A:A carriers.
When the three genetic variants are combined in a genotype score, the odds of having vitamin D deficiency increases by 147% in individuals in the top quartile of this score in comparison to the lowest quartile [118]. Furthermore, the risk of severe vitamin D deficiency (serum 25-OHD <20 nmol/L) increases by 43%.
The results of the two large meta-analyses are supported by recent studies in Chinese [126] and Afro-Americans [123]. Both studies confirmed the aforementioned SNPs in the GC, CYP2R1, and DHCR7 genes as significant determinants of the serum 25-OHD concentration. However, in African-Americans Batai et al. observed the strongest association for CYP2R1 (rs12794714), while in European-Americans CYP2R1 (rs1993116) was the most relevant determinant. Further detail on the associations between genetic variation in the vitamin D pathway and biochemical outcomes is provided in a review by Jolliffe et al. [119].
Genetic factors also appear to influence the responsiveness to vitamin D supplementation. Nimitphong et al. reported a lesser increase in serum 25-OHD after 3 months of 400 IU/day vitamin D3 supplementation in individuals with the GC(rs4588) CA or AA alleles when compared to CC homozygous individuals. However, no such difference was found when the supplement was vitamin D2 [130]. The group also found a significant association between variants in the PTH gene promoter and serum 25-OHD concentrations. PTH has a crucial role in the regulation of 1,25-(OH)2D, vitamin D production, and PTH gene SNPs have been related to bone growth and development. The T allele of SNP rs1459015 was associated with higher level of 25-OHD in a Sudanese cohort and the T allele of SNP rs10500783 was associated with higher level of 25-OHD in a Saudi Arabian study population [126].
Finally, results from GWAS, such as the SUNLIGHT study (Study of Underlying Genetic Determinants of Vitamin D and Highly Related Traits) have identified four SNPs significantly associated with 25-OHD level [131]. These SNPs are: rs2282679 in GC, rs12785878 near DHCR7, rs10741657 near CYP2R21, and rs6013897 in CYP24A1. All these SNPs lay in or near genes strongly involved in vitamin D metabolism. Furthermore, all these 25-OHD- decreasing alleles were associated with an increased risk of multiple sclerosis [131].
The relative difference of mean 25-OHD concentrations between subjects carrying one of the above mentioned polymorphisms and those without, ranges
from -6.4% to 34.4% for the rs2282679 (GC); from -16.7% to 0% for rs3829251 (DHCR7); and from 1.5% to 14.4% for rs2060793 (CYP2R1) [117]. Based on pooled data from various cohorts SNPs accounted for 2.8% of the overall variance of the circulating 25-OHD concentration, which is well within the analytical variation for this metabolite thus limiting the clinical significance of SNPs in daily practice. However, in some individuals with particular combinations of SNPs the effect on 25-OHD can be much greater and the assessment of SNPs may help to explain continuously low 25-OHD blood concentrations. Considering that the effects of SNPs on 25-OHD have been studied with different assays that are characterized by a variable analytical performance, questions regarding the relevance of these SNPs for the assessment of patients vitamin D status remain. Therefore, studies on large cohorts using well standardized methods for the measurement of 25-OHD are needed to shed further light on this issue.
Existing data strongly support genetic variants as important determinants of vitamin D metabolism and serum 25(OH) concentrations. The results of numerous GWAS studies have helped to improve our understanding of vitamin D homeostasis and could assist in the identification of individuals at risk of vitamin insufficiency. For example, in view of different serum 25-OHD concentrations but similar bone mineral density in Africans and Caucasians, using the same cut-off for vitamin D deficiency across different ethnic groups may be inappropriate. Furthermore, assessment of relevant SNPs may be useful to adjust treatment in individuals with an insufficient response to vitamin D supplementation.
Measurement of vitamin D metabolites - analytical aspects
The determination of vitamin D metabolites, whether 25-OHD, 1,25-(OH)2D, 24,25-(OH)2D, “bioavailable” or “free” vitamin D, is a challenging task. This section will provide an overview of the different methods available for the measurement of these metabolites and the major issues that must be addressed to ensure accuracy of measurement.
25-hydroxy vitamin D determination
25-OHD is currently considered the metabolite most representative of vitamin D status. Unfortunately, assays for 25-OHD determination remain difficult to develop despite recent technological advances [132]. 25-OHD assays need to recognize 25-OHD2 and 25-OHD3. Furthermore, 25-OHD is a very hydrophobic molecule that circulates bound to DBP, ALB and lipoproteins. Prior to detection, 25-OHD needs to be dissociated from its carriers.
As 25-OHD2 and 25-OHD3 have different affinity constants for these carriers, the dissociation step must be highly efficient to obtain an accurate quantification of total 25-OHD. This aspect is particularly important for automated immunoassays where, in contrast to radioimmunoassays (RIA), binding-protein or chromatographic assays, organic solvents cannot be used for extraction. Automated immunoassays need alternative releasing agents, which do not always achieve total dissociation of 25-OHD. Particularly in conditions such as pregnancy, estrogen therapy or renal failure, automated immunoassays often fail to correctly quantify 25-OHD [133-136]. Another issue with 25-OHD assays is linked to the recovery of the metabolite when exogenous 25-OHD is added in vitro (as in the preparation of a calibration curve). Indeed, it is not clear whether exogenous metabolites bind to all the different carriers in the same proportions as endogenous metabolites. Under-recovery of exogenous 25-OHD has been reported in automated immuoassays [137, 138] and even LC-MS/MS methods [139].
The different methods available for the quantitation of 25-OHD use either chromatographic separation (HPLC with UV or LCMS/MS detectors), antibodies or binding- proteins. If binding-protein assays have been used in the early eighties and presented clinically acceptable analytical sensitivity and imprecision, they have been superseded by the introduction of novel technologies, either HPLC or polyclonal antibodies. Indeed, the binding-protein methods that were based on the displacement of 3H-labeled 25-OHD, necessitated a chromatographic purification after organic extraction. They were time-consuming and incompatible with the demands on current laboratories.
Radio-immunoassays
RIA were developed in the early eighties. Until recently, they were in routine use in clinical laboratories. By 2015, however, they were used by <2% of all participants of the Vitamin D External Quality Assessment Scheme (DEQAS). The first commercially available RIA was manufactured by DiaSorin and was based on a method described by Hollis et al. in 1993 [140]. This assay had a limit of detection of 2.8 ng/mL, intra- and inter-assay coefficients of variation of about 6 and 15%, respectively and equimolar recovery not only of 25-OHD2 and 25-OHD3, but also 24,25-OH2D, 25,26-OH2D and 25-OHD3-26,23 lactone, which are metabolites known to increase after vitamin D supplementation with large doses. Comparison of this RIA with a HPLC/UV method gave the regression equation RIA= 0.87 x HPLC+3.1 [141].
The DiaSorin RIA method was the most widely used method for both routine diagnostic testing as well as for clinical studies. The traditional 25-OHD cut-offs in use today for vitamin D deficiency (either 20 or 30 ng/mL) have been defined on the bases of studies (and metaanalysis of studies) that predominantly used this assay. However, many of the automated methods used today in clinical laboratories do not agree well with the DiaSorin RIA. Therefore, extrapolation of these cut-offs to other methods is hazardous. This important aspect is not adequately addressed in current clinical guidelines. Hopefully, scientific societies will soon discuss this problem and provide practical guidance how to deal with between- method variability.
Automated immunoassays
The first automated immunoassay for 25-OHD determination was launched in 2001 by Nichols Diagnostics on the Advantage platform. The test was approved by the FDA (510k clearance) on the basis of a Passing-Bablok regression with the DiaSorin RIA of: Nichols=1.10x DiaSorin RIA -0.6 with a wide 95% confidence interval of the slope (0.94-1.27). The assay used a competitive ligand binding technique with acridinium-ester labeled anti-DBP. It was later demonstrated that the assay was unable to correctly measure samples containing substantial amounts of 25-OHD2 [132]. Subsequently, most of the major in-vitro diagnostic companies have launched their own methods for 25-OHD determination. The characteristics of these assays, as claimed by the manufacturers, can be found in Table 1. Most of these methods use a competition design, except the one from Fujirebio on the Lumipulse, which is a non-competitive (sandwich) method based on antimetatype monoclonal antibodies against a hapten- antibody immunocomplex using an ex vivo antibody development system, namely the Autonomously Diversifying Library system, a process which has recently been validated [142, 143].
A large number of studies have evaluated the different automated assays by comparison with RIA, HPLC or, more recently, with LC-MS/MS methods. Conclusions regarding the accuracy of assays have also been based on the results of large external proficiency testing programs, such as DEQAS. The conclusions that can be drawn from these data are unfortunately not totally clear. Indeed, the standardization of the automated assays and the comparator method may differ (see below). Furthermore, differences in the serum matrix between study populations (e.g. healthy subjects, patients with chronic kidney disease, dialysis patients, pregnant women, different ethnic groups, patients in intensive care with fluid shifts) is an important issue that can impact the performance of automated 25-OHD immunoassays. Recently, we have shown good clinical concordance between four different immunoassays and a VDSP-traceable LC-MS/MS method in healthy subjects. However, significantly poorer agreement with the same LC-MS/MS method has been found in other clinical populations [132].
Assessment of the recovery of different forms of vitamin D (i.e. 25-OHD2, 24,25-OH2D, 25,26-OH2D, C3-epimers) is another problem when comparing the performance of 25-OHD immunoassays. Experience has shown that many assays show differences in recovery of spiked vs. native samples. Unfortunately, most manufacturers make cross-reactivity claims based on spiked samples. Sometime these claims are very misleading with regard to patient samples. For example, for the Cobas assay Roche claims a recovery of the C3-epimer of 91%. While Roche evaluated C3-epimer recovery on spiked samples, a later study on native samples demonstrated that the assay does not cross-react with this metabolite at all [144]. A hypothesis that may explain this discrepancy is that the partitioning of different moieties in spiked material does not reflect the natural partitioning of these compounds in native samples. Furthermore, the kinetics of the antigen-antibody reaction may be affected by the organic solvent that is used for the spiking experiments.
Standardization of the 25-hydroxy vitamin D assays
Standardization of the different assays is key to achieving comparable results across different methods and manufacturers. Furthermore, assay standardization is of critical importance for the establishment of common clinical cut-offs and their use in routine practice. Applying a common cut-off value on results generated with poorly standardized assays will inevitably lead to inconsistent patient classification and inappropriate therapeutic decisions. The results of DEQAS or the results of recent studies that compared the most commonly used 25-OHD assays [41, 135], may be viewed in two different ways. The optimistic conclusion is that results are reasonably
? ?missing ? ? see PDF
Free and bioavailable vitamin D
Approximately 99% of 25-OHD is transported in the circulation bound to binding proteins, mostly to DBP and, to a lesser extent, ALB. Free 25-OHD is defined as circulating 25-OHD bound to neither DBP nor ALB. Bioavail- able 25-OHD is defined as the free plus ALB-bound forms. These concepts are not new since they were described in 1989 [149]. However, they have been recently put under the spotlight in different publications dealing with the free hormone hypothesis [150], the difference in DBP concentrations in Whites and Blacks [106] (even if this has recently been challenged [151] and the better association of free or bioavailable vitamin D with mineral parameters, compared to total 25-OHD in postmenopausal women [152] or hemodialysed patients [153].
Free vitamin D can be estimated with a formula, derived from the Vermeulen formula [154], that takes into account 25-OHD, DBP and ALB levels together with their affinity constants [155]: free 25-OHD=total 25-OHD/[1+(6x 103xALB)+(7x108xDBP)].
Use of this formula is not free from criticism. It has not been validated against a reference method, results will be dependent on the 25-OHD assay used and matrix effects can significantly impact the results in particular populations [156]. Caution therefore needs to be taken when interpreting the results of such a formula. An ELISA kit commercialized by Diasource is also available to determine free or bioavailable 25-OHD. The first version of the assay was withdrawn from the market due to sensitivity and reproducibility problems. A second version was recently been made available with improved precision (personal communication, unpublished data) but the lack of a reference method and the very low concentrations of free and bioavailable vitamin D remain clear limitations.
1,25-(OH)2D and 24,25-(OH)2D
Immunoassays
The first assays for the determination of 1,25-(OH)2D were developed in the early 1970s. They were based on the isolation of a protein from rachitic chick intestinal mucosa (later identified as being the VDR) and a competition for this receptor between 1,25-(OH)2[3H]D3 and the patient’s endogenous 1,25-(OH)2D extracted with organic solvents [157-159]. These assays required laborious extraction of the receptor and chromatographic separation prior to measurement. Furthermore, these assays required a substantial sample volume, typically 5-20 mL. The sensitivity of these assays was up to 10 pg per tube, but no 1,25- (OH)2D was detected in the plasma of nephrectomized subjects and end-stage renal failure patients [160]. Subsequently, RIA methods using rabbit antibodies, chromatographic separation and 1,25-(OH)2[3H]D3 were described [161, 162]. Such methods had a sensitivity of 2 pg per tube, an inter-assay CV of 12.6% and required 1.5 mL of serum. With these assays 1,25-(OH)2D could be detected in end- stage renal failure patients, for example, in 67 hemodialysis patients a mean 1,25-OH2D concentration of 18.7±6.4 ng/L was reported [161]. The first RIA using 125I-labeled q,25-(OH)2D was developed and commercialized in 1996
. This assay used an acetonitrile extraction followed by solid phase chromatography, required 500-750 pL of serum and had a sensitivity of 2.4 pg/mL. The imprecision ranged between 12 and 20%. With this method, the mean 1,25-(OH)2D concentration in hemodialysed patients was 9.3±3.4 pg/mL. The latest evolution in RIA assays has been developed by IDS with the use of antibody bound mini-immunocapsules that capture 1,25-(OH)2D after sample delipidation. In 2007 the same company launched an ELISA that apparently demonstrated good sensitivity
. In the last 2 years, IDS and DiaSorin have commercialized automated methods for the measurement of 1,25- (OH)2D on the iSYS and Liaison XL platforms, respectively. The first version of the IDS method is a semi-automated method that uses an offline extraction of the immune- capsules and determination on the iSYS instrument in a competitive fashion using an acridinium ester derivative
. A few months later, the company launched a fully automated version of their assay [166]. The first independent validation studies of these methods revealed an underestimation when compared to the IDS RIA and an under-recovery of 1,25-(OH)2D2. However, according to the investigators the results obtained with these automated methods compare well to LC-MS/MS-MS methods and ALTM in the DEQAS program.
Concurrently, DiaSorin launched a fully automated 1,25-(OH)2D assay on the Liaison XL platform that uses a recombinant fusion protein to capture 1,25-(OH)2D and a murine monoclonal antibody that specifically recognizes the complex formed by the recombinant fusion protein and 1,25-(OH)2D. This elegant assay has a CV of about 5%, performance superior to two LCMS/MS methods [167]. A clinical evaluation of this assay has also shown that it gives the expected variations in patients compared to “normal” values obtained in an extensive reference population [168]. These automated assays are, however, quite new and we lack an extensive evaluation of their performance in daily practice.
LC-MS/MS methods
Despite the great advances that have recently occurred in terms of separation techniques, together with an improvement of the sensitivity in mass spectrometry detectors, absolute quantification of the main dihydroxylated metabolites of vitamin D still remains a challenge.
The first LC-MS/MS methodology able to quantify both 24,25-(OH)2D and 1,25-(OH)2D, including vitamin D2, vitamin D3 and 25-OHD3 in human plasma, was described by Watson et al. in 1991 [169]. However, this method lacked sensitivity and thus was not feasible for use in clinical practice. The first LC-MS/MS method with clinically useful limits of quantification (LOQ) was described almost 20 years later by Duan et al. [170], with validated LOQs for 1,25-(OH)2D3 and 24,25-(OH)2D3 of 5 pg/mL and 50 pg/mL, respectively.
The first important issue that has to be addressed when dealing with these vitamin D metabolites is to accurately select the species to be measured. The only 24,25-(OH)2D form found in humans is the 24R isomer (24R,25-(OH)2D3) [171] whereas 1a,25-(OH)2D is the isomer of interest when 1,25-(OH)2D is measured. 1a,25-(OH)2D2 and 1a,25-(OH)2D3 are usually quantified together. Normal circulating values for 24,25-(OH)2D range from 1 to 4 ng/mL and are even lower for 1,25-(OH)2D, ranging from 15 to 60 pg/mL [172]. Another drawback is that half-life for 24,25-(OH)2D is approximately 7 days but circulating 1,25- (OH)2D has a very short half-life of 4 h only [173]. The low concentrations of these analytes force laboratories to buy instruments with the highest sensitivity.
However, the main challenges faced when measuring 24R,25-(OH)2D3 and 1a,25-(OH)2D with mass spectrometry are the occurrence of interferences and a low ionization efficiency. Isobaric interferences are common in mass spectrometry, especially when using triple quadrupoles in selected reaction monitoring (SRM) mode for quantification. They arise from ions possessing the same nominal mass as the ion of interest and lead to incorrect quantification as triple quadrupole mass spectrometers resolve ions in mass units. To avoid isobaric interferences, chromatographic separation of these compounds prior to mass spectrometry is mandatory. For example, 1a,25-(OH)2D and 24R,25-(OH)2D share the same transitions in the mass spectrometer because they differ only in the position of one hydroxyl group. Consequently, when co-eluted they can interfere with each other. Another potential interference is the occurrence of the epimeric forms 1a,25-(OH)2-3-epi-D3 and 24,25-(OH)2-3-epi-D3 [174], which need to be separated by chromatography. An extensive list of potentially interfering compounds can be consulted in the Supplementary Information of the work of Duan et al. [170]. Recently, it has been observed that some lubricants used in LC-MS instruments can also hamper an accurate quantification of some monohydroxylated compounds including 25-OHD as they can share the same transitions. However, no studies have been performed for the dihydroxylated compounds 1a,25-OH2D and 24R,25-OH2D.
Most of the interferences described above are due to the fact that when using electrospray ionization (ESI), the most sensitive transition is an unspecific water loss. If one sample contains two different hydroxylated compounds with the same molecular weight but different molecular formula, they will usually produce the same transition via a water loss. Strategies to differentiate these molecules are chromatographic separation prior to mass spectrometry or the selection of another specific fragment that is not the result of a water loss. Another type of interference arises from the difficulty in differentiating the loss of an ammonia moiety (NH4-) or water in the ion source as both share the same molecular weight of 18 g/mol. Consequently, resolution of these interferences can only be achieved by exact mass instruments such as time of flight (Q-TOF) or Orbitrap mass spectrometers. Nowadays, the most advanced separation technique for the determination of selected hydroxylated compounds, alone or in combination, is ultra-high pressure liquid chromatography with C18 columns (UHPLC) [175-180]. Chiral columns have also been proposed for the separation of these compounds in shorter time-frames [174, 181]. Two-dimensional UHPLC (2D-LC) with column switching systems [182, 183] has also been tested, but the sophisticated configuration of a 2D-LC is rather difficult to set up. Another possibility is to use micro-flow UHPLC [170] with flow rates of 1-10 pL/min. However, such slow flow rates tend to be unstable. When measuring 1a,25-OH2D and 24R,25-OH2D by LC-MS/MS the preferred ionization technique is positive electrospray ionization (ESI+) due to its superior sensitivity compared to atmospheric pressure chemical ionization (APCI) [173, 180].
In many of the published LC-MS/MS methods the poor ionization of hydroxylated vitamin D metabolites, and resulting low sensitivity in the mass spectrometer, is addressed by derivatization with a Cookson-type reagent. Via a Diels-Alders reaction selective to dienes, the ionization can be improved 100- to 1000-fold by resonance after the addition of crown ether complexes. Such a deri- vatization can overcome the main problems related to the measurement of vitamin D metabolites: a very low analyte concentration, thermal instability and low polarity of the target compounds. The most common Cookson- type reagent is PTAD [171, 175-177, 179-194], but other similar reactants such as MBOTAD [187], DMEQ-TAD [188] or DAPTAD [168, 188, 190] have also been tested. Today, the commercial Amplifex Diene from ABSciex is increasingly used [191, 192] since it provides better sensitivity compared to PTAD. For example, when determining 1,25- (OH)2D with a method that the uses the Amplifex Diene from ABSciex for derivatization the signal-to-noise ratio increases 10-fold compared to PTAD. This improvement is mainly achieved through a quaternary amine moiety [191].
Another, much simpler, approach to increase sensitivity when measuring hydroxylated vitamin D metabolites present at low concentrations is the addition of mobile phase modifiers. For example, Casetta et al. promoted the addition of 0.5 mM lithium acetate to the mobile phase, which results in the formation of Li-adducts that can be detected by tandem mass spectrometers with high sensitivity [182, 186]. However, without derivatization, the LOQ for the measurement of 1,25-(OH)2D is still too high for clinical use (around 15 pg/mL). Another option is the addition of methylamine in order to increase the ionization efficiency after derivatization with PTAD [175].
In order to mitigate the described problems, it is almost mandatory to perform a thorough sample clean-up. The vast majority of sample pre-treatments described in the literature are based on protein precipitation, followed by solid phase extraction (SPE) with OASIS HLB cartridges and derivatization with a Cookson-type reagent [170, 175, 185, 188]. Liquid-liquid extraction (LLE) is another option that is significantly cheaper due to the low cost of solvents compared to SPE cartridges. However, SPE is preferred over LLE as it is faster, more precise and provides cleaner extracts. Another alternative is selective SPE immunoex- traction followed by PTAD derivatization [193]. With this approach a very low LOQ of 1.5 pg/mL can be achieved, but the total sample pre-treatment time is 36 h. A method published by Yuan et al. employs SPE immunoextraction without derivatization. With this approach total sample pre-treatment time is significantly shorter, however the LOQ for 1,25-(OH)2D is 3.4 pg/mL [187]. Recently, selective extraction by supported liquid-liquid extraction (SLE) has been proposed as a further improvement by Biotage Applications [194]. This technique is based on the use of a diatomaceous earth as a stationary vehicle for the aqueous phase of the LLE procedure and the subsequent elution of compounds with organic solvents. Compared with LLE, SLE offers the advantages of an equivalent, or more efficient, extraction, no emulsion formation, easy automation, as well as reduction of organic solvent consumption and glassware. Additionally, there is no need to equilibrate or wash the cartridges containing the stationary phase as in routine SPE extraction. From a routine clinical laboratory’s point-of-view, automation of all the sample treatment steps is almost mandatory, because of the high workload [195, 196].
Sample volume is a key issue when designing a sample pre-treatment procedure. For example, the candidate reference procedure recently proposed by Tai and Nelson will be difficult to apply in routine laboratories, since it requires 2 g of serum [197]. Any reduction in sample volume has to be balanced with the need to assure sample homogeneity. A sample volume between 100 and 250 pL is probably a reasonable compromise. Interestingly, for dihydroxy metabolites, the lowest LOQs are achieved with plasma whereas monohydroxylates are quantified more easily in serum [198]. Furthermore, sample pre-treatment with SPE results in lower LOQs than classical deproteinization.
Finally, taking into account the complexity and variability of plasma and serum samples, it is necessary to add isotopically labeled internal standards (IL-IS) for each analyte at the beginning of the sample pre-treatment procedure. The use of IL-IS enables compensation for matrix effects, variability during sample treatment and any fluctuation of the instrument signal. This method is called isotope dilution mass spectrometry (IDMS) and is known to yield the most accurate, precise and reliable results. It is worth pointing out that the development of an extraction procedure based on IDMS requires, firstly, quantitative extraction of the analyte species and, secondly, complete isotope equilibration in the liquid phase between the endogenous and isotopically added enriched species. Although this is usually a problem related to sample pretreatment of solid samples, complex liquid matrices, such as serum or plasma, can also be affected, since the added standards are not linked to the matrix in the same way as endogenous compounds [139]. Most current methods for the quantification of 1,25-(OH)2D and 24,25-(OH)2D use d6-1,25-(OH)2D3 as internal standard for both compounds. However, the lack of a specific isotopic analog for 24,25- (OH)2D results in a slightly higher imprecision and, in some cases, underestimation of 24,25-(OH)2D [178]. In 2014, d6-24,25-(OH)2D3 became available and should be used as IL-IS in all future studies where 24,25-(OH)2D is measured by LC-MS/MS [178].
It can be expected that future LC-MS/MS methods for the simultaneous determination 24,25-(OH)2D and 1.25-(OH)2D will employ online automated sample pretreatment without any derivatization step. However, when instrument sensitivity is insufficient to reach the desired LOQ, a less extensive sample clean-up with a subsequent Cookson-type reagent based derivatization step is the best option. Another derivatization reagent has been also proposed in a patent from DH Technologies Singapore, in which a reactant permits a specific carboxyl (CO) loss instead of the common water loss [199]. Regarding chromatography, UHPLC with C18 columns is the most convenient and user friendly system. Recently, another separation technique based on the use of CO2 as mobile phase, known as supercritical fluid chromatography (SFC), has been proposed as another approach that promises superior separation of the compounds of interest compared with traditional reverse phase columns [200]. However, this system is still very uncommon even in research laboratories due to its technical difficulty.
Practical implications of analytical uncertainty
The lack of standardization of the measurement of 25-OHD and other vitamin D metabolites causes substantial analytical uncertainty, which has to be taken into consideration when reading epidemiological studies and interpreting individual patient results. Many of the studies that have been taken into consideration for the setting of the common 75 nmol/L cut-off have been performed with the Diasorin RIA. Therefore, when applying this cut-off across assays they should all be traceable to the Diasorin RIA. Otherwise, the validity of this cut-off is limited and review is needed. From our point of view, the application of a common cut-off for 25-OHD across different assays is inappropriate because by the end of 2015 EQA programs showed that assays from different manufacturers can differ by more than 100%. When using a common cut-off such discrepancies have major clinical implications as patient classification is strongly assay dependent. Therefore, current guidelines should be reviewed with a focus on analytical uncertainty. We believe that manufacturers should provide an alternative assay specific cut-off based on the long term bias of their assay in EQA programs or large studies with a sufficient number of samples containing a 25-OHD concentration around the 75 nmol/L cut-off.
In addition to assay specific cut-offs, racial differences should also be considered. The significantly lower 25-OHD concentration in Blacks compared to Whites without significant differences in PTH is the best argument for such differential cut-offs. In view of the variable performance of 25-OHD assays and uncertainties about the validity of a common cut-off, one might ask if the substantial increase in 25-OHD testing is justified. Our long term experience with a thoroughly validated commercial LC-MS/MS method from RECIPE, which performs excellently in the EQA scheme from the Royal College of Pathologists of Australasia, demonstrates average 25-OHD concentrations in the insufficient range across all age groups, with lowest values in children and adolescent. Considering the physiological consequences of an insufficient supply of vitamin D for growth, bone mass accrual, fracture risk and muscle function, limiting vitamin D testing to specific groups is hard to achieve practically and ethically questionable.
Conclusions
The assessment of vitamin D status is a changing landscape. Although 25-OHD is still recommended as the marker of choice by virtually all scientific bodies growing evidence indicates significant limitations that hamper the utility of this analyte in clinical practice. Issues related to the use of 25-OHD include analytical aspects and the interpretation of results. While in normal individuals the agreement of results generated with automated assays is improving, comparibility of results in distinct populations, such as children, pregnant women, hemodialysis patients or intensive care patients, remains problematic. The lack of assay standardization hampers the use of a common cut-off for 25-OHD. Furthermore, the cut-offs used today are based on studies that measured 25-OHD with a non-standardized assay that does not compare well with many of the current methods. Therefore, scientific bodies urgently need to review their recommendations regarding the use of a common cut-off across different methods and different ethnic groups. The relationships between 25-OHD and various clinical indices are rather weak and not consistent across races. Recent studies have provided new insights in physiological and analytical aspects of vitamin D that may change the way how we will assess vitamin D status in the future. The VMR (25-OHD/24,25- OH2D ratio), ‘free’ and ‘bioavailable’ vitamin D are all interesting markers that have expanded our knowledge about vitamin D metabolism. However, a range of unresolved analytical issues limit the use of these markers in daily practice. It can be expected that some of these limitations will be overcome in the near future so that these analytes may be considered for routine use (at least in specialized centers). It has also emerged that genetic variants are important determinants of vitamin D metabolism and serum 25-OH concentrations. Assessment of SNPs in the genes of DBP, 7-dehydrocholesterol reductase and VDR can assist in the identification of individuals at risk of vitamin D insufficiency and may be useful to adjust treatment in individuals with an insufficient response to vitamin D supplementation.
Author contributions: All the authors have accepted responsibility for the entire content of this submitted manuscript and approved submission.
Research funding: None declared.
Employment or leadership: None declared.
Honorarium: None declared.
Competing interests: The funding organization(s) played no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the report for publication.
References
Lips P. Worldwide status of vitamin D nutrition. J Steroid Bio- chem Mol Biol 2010;121:297-300.
Holick MF. Vitamin D deficiency. N Engl J Med 2007;357:266-81.
Zhao S, Gardner K, Taylor W, Marks E, Goodson N. Vitamin D assessment in primary care: changing patterns of testing. London J Prim Care (Abingdon) 2015;7:15-22.
Holick MF. Sunlight “D”ilemma: risk of skin cancer or bone disease and muscle weakness. Lancet 2001;357:4-6.
Nowson CA, McGrath JJ, Ebeling PR, Haikerwal A, Daly RM, Sanders KM, et al. Vitamin D and health in adults in Australia and New Zealand: a position statement. Med J Aust 2012;196:686-7.
Chapuy MC, Meunier PJ. Prevention of secondary hyperparathyroidism and hip fracture in elderly women with calcium and vitamin D3 supplements. Osteoporos Int 1996;6(Suppl 3):60-3.
Murad MH, Elamin KB, Abu Elnour NO, Elamin MB, Alkatib AA, Fatourechi MM, et al. Clinical review: the effect of vitamin D on falls: a systematic review and meta-analysis. J Clin Endocrinol Metab 2011;96:2997-3006.
Bischoff-Ferrari HA, Dietrich T, Orav EJ, Dawson-Hughes B. Positive association between 25-hydroxy vitamin D levels and bone mineral density: a population-based study of younger and older adults. Am J Med 2004;116:634-9.
Bischoff-Ferrari HA, Willett WC, Wong JB, Giovannucci E, Dietrich T, Dawson-Hughes B. Fracture prevention with vitamin D supplementation: a meta-analysis of randomized controlled trials. J Am Med Assoc 2005;293:2257-64.
Harris SS, Soteriades E, Coolidge JA, Mudgal S, Dawson-Hughes B. Vitamin D insufficiency and hyperparathyroidism in a low income, multiracial, elderly population. J Clin Endocrinol Metab 2000;85:4125-30.
Barrett JA, Baron JA, Karagas MR, Beach ML. Fracture risk in the U.S. Medicare population. J Clin Epidemiol 1999;52:243-9.
Cheng S, Tylavsky F, Kroger H, Karkkainen M, Lyytikainen A, Koistinen A, et al. Association of low 25-hydroxyvitamin D concentrations with elevated parathyroid hormone concentrations and low cortical bone density in early pubertal and prepubertal Finnish girls. Am J Clin Nutr 2003;78:485-92.
Zerwekh JE. Blood biomarkers of vitamin D status. Am J Clin Nutr 2008;87:1087S-91S.
Horst RL, Reinhardt TA. Vitamin D metabolism. In: Feldman D, Pike JW, Glorieux FH, editors. Vitamin D, 2nd ed. Amsterdam: Elsevier, 2005.
National Institutes of Health. Vitamin D: fact sheet for health professionals [Internet] National Institutes of Health, Office of Dietary Supplements 2014 [cited 2015 Dec 1]. Available at: https:// ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/.
Pappas A. Epidermal surface lipids. Dermatoendocrinol 2009;1:72-6.
Elias PM, Williams ML, Choi EH, Feingold KR. Role of cholesterol sulfate in epidermal structure and function: lessons from X-linked ichthyosis. Biochim Biophys Acta 2014;1841:353-61.
Glossmann HH. Origin of 7-dehydrocholesterol (provitamin D) in the skin. J Invest Dermatol 2010;130:2139-41.
Tsiaras WG, Weinstock MA. Factors influencing vitamin D status. Acta Derm Venereol 2011;91:115-24.
Holick MF, MacLaughlin JA, Clark MB, Holick SA, Potts JT Jr, Anderson RR, et al. Photosynthesis of previtamin D3 in human skin and the physiologic consequences. Science 1980;210: 203-5.
Chen TC, Lu Z, Holick MF. Photobiology of vitamin D. In: Holick M, editor. Vitamin D: physiology, molecular biology, and clinical applications, 2nd ed. New York: Humana Press, 2010.
Holick MF, Tian XQ, Allen M. Evolutionary importance for the membrane enhancement of the production of vitamin D3 in the skin of poikilothermic animals. Proc Natl Acad Sci USA 1995;92:3124-6.
Tian XQ, Chen TC, Lu Z, Shao Q, Holick MF. Characterization of the translocation process of vitamin D3 from the skin into the circulation. Endocrinology 1994;135:655-61.
Whyte MP, Haddad JG Jr, Walters DD, Stamp TC. Vitamin D bioavailability: serum 25-hydroxyvitamin D levels in man after oral, subcutaneous, intramuscular, and intravenous vitamin D administration. J Clin Endocrinol Metab 1979;48:906-11.
Webb AR, DeCosta BR, Holick MF. Sunlight regulates the cutaneous production of vitamin D3 by causing its photodegradation. J Clin Endocrinol Metab 1989;68:882-7.
Holick MF, MacLaughlin JA, Doppelt SH. Regulation of cutaneous previtamin D3 photosynthesis in man: skin pigment is not an essential regulator. Science 1981;211:590-3.
Ross AC, Taylor CL, Yaktine AL, Del Valle HB. Dietary reference intakes for calcium and vitamin D. Washington DC: National Academies Press, 2011.
Holick MF. Vitamin D: the underappreciated D-lightful hormone that is important for skeletal and cellular health. Curr Opin Endocrinol Diab 2002;9:87-98.
Willett AM. Vitamin D status and its relationship with parathyroid hormone and bone mineral status in older adolescents. Proc Nutr Soc 2005;64:193-203.
Cheng JB, Levine MA, Bell NH, Mangelsdorf DJ, Russell DW. Genetic evidence that the human CYP2R1 enzyme is a key vitamin D 25-hydroxylase. Proc Natl Acad Sci USA 2004;101:7711-5.
Christakos S, Ajibade DV, Dhawan P, Fechner AJ, Mady LJ. Vitamin D: metabolism. Endocrinol Metab Clin North Am 2010;39:243-53.
Lehmann B. The vitamin D3 pathway in human skin and its role for regulation of biological processes. Photochem Photobiol 2005;81:1246-51.
Zehnder D, Bland R, Williams MC, McNinch RW, Howie AJ,
Stewart PM, et al. Extrarenal expression of 25-hydroxyvitamin d(3)-1 alpha-hydroxylase. J Clin Endocrinol Metab 2001;86: 888-94.
Prentice A, Goldberg GR, Schoenmakers I. Vitamin D across the lifecycle: physiology and biomarkers. Am J Clin Nutr 2008;88:500S-6S.
Teichmann A, Dutta P, Staffas A, Jagerstad M. Sterol and vitamin D-2 concentrations in cultivated and wild grown mushrooms: effects of UV irradiation. LWT Food Sci Technol 2007;40:815-22.
Markestad T, Aksnes L, Ulstein M, Aarskog D. 25-Hydroxyvitamin D and 1,25-dihydroxyvitamin D of D2 and D3 origin in maternal and umbilical cord serum after vitamin D2 supplementation in human pregnancy. Am J Clin Nutr 1984;40:1057-63.
Tripkovic L, Lambert H, Hart K, Smith CP, Bucca G, Penson S, et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: a systematic review and meta-analysis. Am J Clin Nutr 2012;95:1357-64.
Houghton LA, Vieth R. The case against ergocalciferol (vitamin D2) as a vitamin supplement. Am J Clin Nutr 2006;84:694-7.
Farrelll CJ, Herrmann M. Determination of vitamin D and its metabolites. Best Prract ResClin Endocrinol Metab 2013;27: 675-88.
Bailey D, Velijkovic K, Yazdanapanah M, Adeli K. Analytical measurement and clinical relevance of vitamin D3 C3-epimer. Clin Biochem 2013;46:190-6.
Farrell C-J, Martin S, McWhinney B, Straub I, Williams P, Herrmann M. State-of-the-art vitamin D assays: a comparison of automated immunoassays with liquid chromatography-tandem mass spectrometry methods. Clin Chem 2012;58:531-42.
Laing C, Cooke N. Vitamin D binding protein. In: Feldman D, Pike JW, Glorieux FH, editors. Vitamin D, 2nd ed. Amsterdam: Elsevier, 2005.
Bouillon R. Why modest but widespread improvement of the vitamin D status is the best strategy? Best Pract Res Clin Endocrinol Metab 2011;25:693-702.
Jones G, Prosser DE, Kaufmann M. Cytochrome P450-mediated metabolism of vitamin D. J Lipid Res 2014;55:13-31.
Shinki T, Jin CH, Nishimura A, Nagai Y, Ohyama Y, Noshiro M, et al. Parathyroid hormone inhibits 25-hydroxyvitamin D3-24-hydroxylase mRNA expression stimulated by 1 alpha,25- dihydroxyvitamin D3 in rat kidney but not in intestine. J Biol Chem 1992;267:13757-62.
Bosworth CR, Levin G, Robinson-Cohen C, Hoofnagle AN, Ruzinski J, Young B, et al. The serum 24,25-dihydroxyvitamin D concentration, a marker of vitamin D catabolism, is reduced in chronic kidney disease. Kidney Int 2012;82:693-700.
Schwartz Z, Sylvia VL, Larsson D, Nemere I, Casasola D, Dean DD, et al. 1alpha,25(OH)2D3 regulates chondrocyte matrix vesicle protein kinase C (PKC) directly via G-protein-dependent mechanisms and indirectly via incorporation of PKC during matrix vesicle biogenesis. J Biol Chem 2002;277:11828-37.
Urushino N, Yasuda K, Ikushiro S, Kamakura M, Ohta M, Sakaki T. Metabolism of 1alpha,25-dihydroxyvitamin D2 by human CYP24A1. Biochem Biophys Res Commun 2009;384:144-8.
Murayama A, Takeyama K, Kitanaka S, Kodera Y, Hosoya T, Kato S. The promoter of the human 25-hydroxyvitamin D3 1 alpha- hydroxylase gene confers positive and negative responsiveness to PTH, calcitonin, and 1 alpha,25(OH)2D3. Biochem Biophys Res Commun 1998;249:11-6.
Kim MS, Fujiki R, Murayama A, Kitagawa H, Yamaoka K, Yamamoto Y, et al. 1Alpha,25(OH)2D3-induced transrepression by vitamin D receptor through E-box-type elements in the human parathyroid hormone gene promoter. Mol Endocrinol 2007;21:334-42.
Prie D, Friedlander G. Reciprocal control of 1,25-dihydroxyvitamin D and FGF23 formation involving the FGF23/Klotho system. Clin J Am Soc Nephrol 2010;5:1717-22.
Shimada T, Kakitani M, Yamazaki Y, Hasegawa H, Takeuchi Y, Fujita T, et al. Targeted ablation of Fgf23 demonstrates an essential physiological role of FGF23 in phosphate and vitamin D metabolism. J Clin Invest 2004;113:561-8.
Omdahl JL, Morris HA, May BK. Hydroxylase enzymes of the vitamin D pathway: expression, function, and regulation. Annu Rev Nutr 2002;22:139-66.
Dusso AS, Rodriguez M. Enhanced induction of Cyp24a1 by FGF23 but low serum 24,25-dihydroxyvitamin D in CKD: implications for therapy. Kidney Int 2012;82:1046-9.
Mousa A, Misso M, Teede H, Scragg R, de Courten B. Effect of vitamin D supplementation on inflammation: protocol for a systematic review. BMJ Open 2016;6:e010804.
Cannell JJ, Grant WB, Holick MF. Vitamin D and inflammation. Dermatoendocrinol 2014;6:1-10.
De-Regil LM, Palacios C, Lombardo LK, Pena-Rosas JP. Vitamin D supplementation for women during pregnancy. Cochrane Database Syst Rev 201614;1:8858-73.
Jones G, Strugnell SA, DeLuca HF. Current understanding of the molecular actions of vitamin D. Physiol Rev 1998;78: 1193-231.
Kamen DL, Tangpricha V. Vitamin D and molecular actions on the immune system: modulation of innate and autoimmunity. J Mol Med (Berl) 2010;88:441-50.
Eyles DW, Smith S, Kinobe R, Hewison M, McGrath JJ. Distribution of the vitamin D receptor and 1[alpha]-hydroxylase in human brain. J Chem Neuroanat 2005;29:21-30.
Bikle D. Nonclassic actions of vitamin D. J Clin Endocrinol Metab 2009;94:26-34.
Stoffels K, Overbergh L, Bouillon R, Mathieu C. Immune regulation of 1alpha-hydroxylase in murine peritoneal macrophages: unravelling the IFNgamma pathway. J Steroid Biochem Mol Biol 2007;103:567-71.
Esteban L, Vidal M, Dusso AJ. 1Alpha-hydoxylase transactivation of gamma-interferon in murine macrophages required enhanced C/EBPbeta expression and activation. J Steroid Biochem Mol Biol 2004;89-90:131-7.
Bikle DD, Pillai S, Gee E, Hincenbergs M. Regulation of 1,25-dihydroxyvitamin D production in human keratinocytes by interferon-gamma. Endocrinology 1989;124:655-60.
Pillai S, Bikle DD, Eliasa PM. 1,25-Dihydroxyvitamin D production and receptor binding in human keratinocytes varies with differentiation. J Biol Chem 1988;263:5390-5.
Jones G, Prosser DE, Kaufman M. 25-Hydroxyvitamin D-24-hy- droxylase (CYP24A1): its important role in the degradation of vitamin D. Arch Biochem Biophys 2012;523:9-18.
Lohnes D, Jones G. Further metabolism of 1 alpha,25-dihydroxy- vitamin D3 in target cells. J Nutr Sci Vitaminol (Tokyo) 1992;Spec No:75-8.
Adams JS, Hewison M. Extrarenal expression of the 25-hydroxyvitamin D-1-hydroxylase. Arch Biochem Biophys 2012;523: 95-102.
Bikle DD. Vitamin D metabolism, mechanism of action, and clinical applications. Chem Biol 2014;21:319-29.
Pusceddu I, Farrell CJ, Di Pierro AM, Jani E, Herrmann W, Herrmann M. The role of telomeres and vitamin D in cellular aging and age-related disease. Clin Chem Lab Med 2015;53:1661-78.
Bourdea A, Atmani F, Grosse B, Lieberherr M. Rapid effects of 1,25-dihydroxyvitamin D3 and extracellular Ca2+ on phospholipid metabolism in dispersed porcine parathyroid cells. Endocrinology 1990;127:2738-43.
Sorensen AM, Baran DR. 1 alpha,25-Dihydroxyvitamin D3 rapidly alters phospholipid metabolism in the nuclear envelope of osteoblasts. J Cell Biochem 1995;58:15-21.
Sylvia VL, Schwartz Z, Ellis EB, Helm SH, Gomez R, Dean DD, et al. Nongenomic regulation of protein kinase C isoforms by the vitamin D metabolites 1 alpha,25-(OH)2D3 and 24R,25-(OH)2D3. J Cell Physiol 1996;167:380-93.
Wali RK, Baum CL, Sitrin MD, Brasitus TA. 1,25(OH)2 vitamin D3 stimulates membrane phosphoinositide turnover, activates protein kinase C, and increases cytosolic calcium in rat colonic epithelium. J Clin Invest 1990;85:1296-303.
Wong RG, Myrtle JF, Tsai HC, Norman AW. Studies on calciferol metabolism. V. The occurrence and biological activity of 1,25-dihydroxy-vitamin D 3 in bone. J Biol Chem 1972;247:5728-35.
Tsai HC, Wong RG, Norman AW. Studies on calciferol metabolism. IV. Subcellular localization of 1,25-dihydroxy-vitamin D 3 in intestinal mucosa and correlation with increased calcium transport. J Biol Chem 1972;247:5511-9.
Myrtle JF, Norman AW. Vitamin D: a cholecalciferol metabolite highly active in promoting intestinal calcium transport. Science 1971;171:79-82.
Norman AW, Okamura WH, Friedlander EJ, Henry HL, Johnson RL, Mitra MN, et al. Current concepts of the chemical conformation, metabolism, and interaction of the steroid, vitamin D, with the endocrine system for calcium homeostasis. Calcif Tissue Res 1976;21:153-9.
Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2011;96:1911-30.
Bischoff-Ferrari HA, Giovannucci E, Willett WC, Dietrich T, Dawson-Hughes B. Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am J Clin Nutr 2006;84:18-28.
Priemel M, von Domarus C, Klatte TO, Kessler S, Schlie J, Meier S, et al. Bone mineralization defects and vitamin D deficiency: histomorphometric analysis of iliac crest bone biopsies and circulating 25-hydroxyvitamin D in 675 patients. J Bone Miner Res 2010;25:305-12.
Dobnig H, Pilz S, Scharnagl H, Renner W, Seelhorst U, Wellnitz B, et al. Independent association of low serum 25-hydroxyvitamin d and 1,25-dihydroxyvitamin d levels with all-cause and cardiovascular mortality. Arch Intern Med 2008;168:1340-9.
Ginde AA, Scragg R, Schwartz RS, Camargo CA Jr. Prospective study of serum 25-hydroxyvitamin D level, cardiovascular disease mortality, and all-cause mortality in older U.S. adults. J Am Geriatr Soc 2009;57:1595-603.
Herrmann M, Sullivan DR, Veillard AS, McCorquodale T, Straub IR, Scott R, et al. Serum 25-hydroxyvitamin D: a predictor of macrovascular and microvascular complications in patients with type 2 diabetes. Diabetes Care 2015;38:521-8.
Holick MF. Vitamin D status: measurement, interpretation, and clinical application. Ann Epidemiol 2009;19:73-8.
Woitge HW, Knothe A, Witte K, Schmidt-Gayk H, Ziegler R, Lem- mer B, et al. Circaannual rhythms and interactions of vitamin D metabolites, parathyroid hormone, and biochemical markers of skeletal homeostasis: a prospective study. J Bone Miner Res 2000;15:2443-50.
Schottker B, Jorde R, Peasey A, Thorand B, Jansen EH, Groot Ld, et al. Vitamin D and mortality: meta-analysis of individual participant data from a large consortium of cohort studies from Europe and the United States. BMJ 2014;348:g3656.
Zittermann A, Ernst JB, Gummert JF, Borgermann J. Vitamin D supplementation, body weight and human serum 25-hydroxyvitamin D response: a systematic review. Eur J Nutr 2014;53:367-74.
Glendenning P, Chew GT, Seymour HM, Gillett MJ, Goldswain PR, Inderjeeth CA, et al. Serum 25-hydroxyvitamin D levels in vitamin D-insufficient hip fracture patients after supplementation with ergocalciferol and cholecalciferol. Bone 2009;45:870-5.
Wamberg L, Pedersen SB, Richelsen B, Rejnmark L. The effect of high-dose vitamin D supplementation on calciotropic hormones and bone mineral density in obese subjects with low levels of circulating 25-hydroxyvitamin d: results from a randomized controlled study. Calcif Tissue Int 2013;93:69-77.
Diamond T, Wong YK, Golombick T. Effect of oral cholecalciferol 2,000 versus 5,000 IU on serum vitamin D, PTH, bone and muscle strength in patients with vitamin D deficiency. Osteoporos Int 2013;24:1101-5.
Arya V, Bhambri R, Godbole MM, Mithal A. Vitamin D status and its relationship with bone mineral density in healthy Asian Indians. Osteoporos Int 2004;15:56-61.
Dusso AS, Brown AJ, Slatopolsky E. Vitamin D. Am J Physiol Renal Physiol 2005;289:F8-28.
Hollis BW. Assessment of vitamin D status and definition of a normal circulating range of 25-hydroxyvitamin D. Curr Opin Endocrinol Diabetes Obes 2008;15:489-94.
Holick MF. Resurrection of vitamin D deficiency and rickets. J Clin Invest 2006;116:2062-72.
Demay MB. Hereditary defects in vitamin D metabolism and vitamin D receptor defects. In: DeGroot L, editor. Endocrinology. Philadelphia: WB Saunders, 1995:1173-8.
Drezner MK. Clinical disorders of phosphate homeostasis. Vitamin D, 2nd ed. Boston, MA: Elsevier Academic Press, 2005:1159-87.
Sai AJ, Walters RW, Fang X, Gallagher JC. Relationship between vitamin D, parathyroid hormone, and bone health. J Clin Endocrinol Metab 2011;96:436-46.
Saadi HF, Nagelkerke N, Benedict S, Qazaq HS, Zilahi E, Mohamadiyeh MK, et al. Predictors and relationships of serum 25 hydroxyvitamin D concentration with bone turnover markers, bone mineral density, and vitamin D receptor genotype in Emirati women. Bone 2006;39:1136-43.
Saquib N, von Muhlen D, Garland CF, Barrett-Connor E. Serum 25-hydroxyvitamin D, parathyroid hormone, and bone mineral density in men: the Rancho Bernardo study. Osteoporos Int 2006;17:1734-41.
van Ballegooijen AJ, Robinson-Cohen C, Katz R, Criqui M, Budoff M, Li D, et al. Vitamin D metabolites and bone mineral density: The multi-ethnic study of atherosclerosis. Bone 2015;78:186-93.
Szulc P, Munoz F, Marchand F, Chapuy MC, Delmas PD. Role of vitamin D and parathyroid hormone in the regulation of bone turnover and bone mass in men: the MINOS study. Calcif Tissue Int 2003;73:520-30.
Robinson-Cohen C, Hoofnagle AN, Ix JH, Sachs MC, Tracy RP, Siscovick DS, et al. Racial differences in the association of serum 25-hydroxyvitamin D concentration with coronary heart disease events. J Am Med Assoc 2013;310:179-88.
Aloia JF. African Americans, 25-hydroxyvitamin D, and osteoporosis: a paradox. Am J Clin Nutr 2008;88:545S-50S.
Cauley JA, Danielson ME, Boudreau R, Barbour KE, Horwitz MJ, Bauer DC, et al. Serum 25-hydroxyvitamin D and clinical fracture risk in a multiethnic cohort of women: the Women’s Health Initiative (WHI). J Bone Miner Res 2011;26:2378-88.
Powe CE, Evans MK, Wenger J, Zonderman AB, Berg AH, Nalls M, et al. Vitamin D-binding protein and vitamin D status of black Americans and white Americans. N Engl J Med 2013;369:1991-2000.
Berg AH, Powe CE, Evans MK, Wenger J, Ortiz G, Zonderman AB, et al. 24,25-Dihydroxyvitamin d3 and vitamin D status of community-dwelling black and white Americans. Clin Chem 2015;61:877-84.
Warden SJ, Hill KM, Ferira AJ, Laing EM, Martin BR, Hausman DB, et al. Racial differences in cortical bone and their relationship to biochemical variables in Black and White children in the early stages of puberty. Osteoporos Int 2013;24:1869-79.
Bikle DD, Halloran BP, Gee E, Ryzen E, Haddad JG. Free 25-hydroxyvitamin D levels are normal in subjects with liver disease and reduced total 25-hydroxyvitamin D levels. J Clin Invest 1986;78:748-52.
Henderson CM, Lutsey PL, Misialek JR, Laha TJ, Selvin E, Eck- feldt JH, et al. Measurement by a Novel LC-MS/MS Methodology Reveals Similar Serum Concentrations of Vitamin D-Binding Protein in Blacks and Whites. Clin Chem 2016;62:179-87.
Nielson CM, Jones KS, Chun RF, Jacobs JM, Wang Y, Hewison M, et al. Free 25-hydroxyvitamin D: impact of vitamin D binding protein assays on racial-genotypic associations. J Clin Endocrinol Metab 2016;101:2226-34.
Nielson CM, Jones KS, Chun RF, Jacobs J, Wang Y, Hewison M, et al. Role of assay type in determining free 25-hydroxyvitamin D levels in diverse populations. N Engl J Med 2016;374:1695-6.
de Boer IH, Sachs MC, Chonchol M, Himmelfarb J, Hoofnagle AN, Ix JH, et al. Estimated GFR and circulating 24,25-dihydroxy- vitamin D3 concentration: a participant-level analysis of 5 cohort studies and clinical trials. Am J Kidney Dis 2014;64: 187-97.
Pike JW, Meyer MB. Regulation of mouse Cyp24a1 expression via promoter-proximal and downstream-distal enhancers highlights new concepts of 1,25-dihydroxyvitamin D(3) action. Arch Biochem Biophys 2012;523:2-8.
Stubbs JR, Zhang S, Friedman PA, Nolin TD. Decreased conversion of 25-hydroxyvitamin D3 to 24,25-dihydroxyvitamin D3 following cholecalciferol therapy in patients with CKD. Clin J Am Soc Nephrol 2014;9:1965-73.
Wagner D, Hanwell HE, Schnabl K, Yazdanpanah M, Kimball S, Fu L, Sidhom G, Rousseau D, Cole DE, Vieth R. The ratio of serum 24,25-dihydroxyvitamin D(3) to 25-hydroxyvitamin D(3) is predictive of 25-hydroxyvitamin D(3) response to vitamin D(3) supplementation. J Steroid Biochem Mol Biol 2011;126:72-7.
Ahn J, Yu K, Stolzenberg-Solomon R, Simon KC, McCullough ML, Gallicchio L, Jacobs EJ, Ascherio A, Helzlsouer K, Jacobs KB, Li Q, Weinstein SJ, Purdue M, Virtamo J, Horst R, Wheeler W, Chanock S, Hunter DJ, Hayes RB, Kraft P, Albanes D. Genomewide association study of circulating vitamin D levels. Hum Mol Genet 2010;19:2739-45.
Wang TJ, Zhang F, Richards JB, Kestenbaum B, van Meurs JB, Berry D, et al. Common genetic determinants of vitamin D insufficiency: a genome-wide association study. Lancet 2010;376:180-8.
Jolliffe DA, Walton RT, Griffiths CJ, Martineau AR. Single nucleotide polymorphisms in the vitamin D pathway associating with circulating concentrations of vitamin D metabolites and non-skeletal health outcomes: Review of genetic association studies. J Steroid Biochem Mol Biol 2015;15:30153-9.
Lauridsen AL, Vestergaard P, Hermann AP, Brot C, Heickendorff L, Mosekilde L, et al. Plasma concentrations of 25-hydroxyvitamin D and 1,25-dihydroxy-vitamin D are related to the phenotype of Gc (vitamin D-binding protein): a cross-sectional study on 595 early postmenopausal women. Calcif Tissue Int 2005;77:15-22.
Hansen JG, Tang W, Hootman KC, Brannon PM, Houston DK, Kritchevsky SB, et al. Genetic and environmental factors are associated with serum 25-hydroxyvitamin D concentrations in older African Americans. J Nutr 2015;145:799-805.
Al-Daghri NM, Al-Attas OS, Krishnaswamy S, Yakout SM, Mohammed AK, et al. Association between promoter region genetic variants of PTH SNPs and serum 25(OH)-vitamin D level. Int J Clin Exp Pathol 2015;8:8463-71.
Batai K, Murphy AB, Shah E, Ruden M, Newsome J, Agate S, et al. Common vitamin D pathway gene variants reveal contrasting effects on serum vitamin D levels in African Americans and European Americans. Hum Genet 2014;133:1395-405.
Cheung CL, Lau KS, Sham PC, Tan KC, Kung AW. Genetic variant in vitamin D binding protein is associated with serum 25-hydroxyvitamin D and vitamin D insufficiency in southern Chinese. J Hum Genet 2013;58:749-51.
Lafi ZM, Irshaid YM, El-Khateeb M, Ajlouni KM, Hyassat D. Association of rs7041 and rs45 88 Polymorphisms of the Vitamin D Binding Protein and the rs10741657 Polymorphism of CYP2R1 with Vitamin D Status Among Jordanian Patients. Genet Test Mol Biomarkers 2015;19:629-36.
Zhang Z, He JW, Fu WZ, Zhang CQ, Zhang ZL. An analysis of the association between the vitamin D pathway and serum 25-hydroxyvitamin D levels in a healthy Chinese population.J Bone Miner Res 2013;28:1784-92.
Sinotte M, Diorio C, Berube S, Pollak M, Brisson J. Genetic polymorphisms of the vitamin D binding protein and plasma concentrations of 25-hydroxyvitamin D in premenopausal women. Am J Clin Nutr 2009;89:634-40.
Engelman CD. Genetic architecture of vitamin D. Wisconsin Med J 2009;108:273-4.
Kawakami M, Blum CB, Ramakrishnan R, Dell RB, Goodman DS. Turnover of the plasma binding protein for vitamin D and its metabolites in normal human subjects. J Clin Endocrinol Metab 1981;53:1110-6.
Nimitphong H, Saetung S, Chanprasertyotin S, Chailurkit LO, Ongphiphadhanakul B. Changes in circulating 25-hydroxyvitamin D according to vitamin D binding protein genotypes after vitamin D3 or D2 supplementation. Nutr J 2013;12:39.
Mokry LE, Ross S, Ahmad OS, Forgetta V, Smith GD, Leonga A, et al. Vitamin D and risk of multiple sclerosis: a mendelian randomization study. PLoS Med 2015;12:e1001866.
Hollis BW. The determination of circulating 25-hydroxyvitamin D: No easy task. J Clin Endocrinol Metabolism 2004;89: 3149-51.
Moreau E, Bacher S, Mery S, Le Goff C, Piga N, Vogeser M, et al. Performance characteristics of the VIDAS® 25-OH Vitamin D Total assay - comparison with four immunoassays and two liquid chromatography-tandem mass spectrometry methods in a multicentric study. Clin Chem Lab Med 2016;54:45-53.
Depreter B, Heijboer AC, Langlois MR. Accuracy of three automated 25-hydroxyvitamin D assays in hemodialysis patients. Clin Chim Acta 2013;415:255-60.
Heijboer AC, Blankenstein MA, Kema IP, Buijs MM. Accuracy of 6 routine 25-hydroxyvitamin D assays: Influence of vitamin D binding protein concentration. Clin Chem 2012;58:543-8.
Cavalier E, Lukas P, Crine Y, Peeters S, Carlisi A, Le Goff C, et al. Evaluation of automated immunoassays for 25(OH)-vitamin D determination in different critical populations before and after standardization of the assays. Clin Chim Acta 2014;431:60-5.
Carter GD, Jones JC, Berry JL. The anomalous behaviour of exogenous 25-hydroxyvitamin D in competitive binding assays. J Steroid Biochem Mol Biol 2007;103:480-2.
Horst RL. Exogenous versus endogenous recovery of 25-hydroxyvitamins D2 and D3 in human samples using high- performance liquid chromatography and the DiaSorin LIAISON Total-D Assay. J Steroid Biochem Mol Biol 2010;121:180-2.
Lankes U, Elder PA, Lewis JG, George P. Differential extraction of endogenous and exogenous 25-OH-vitamin D from serum makes the accurate quantification in liquid chromatography- tandem mass spectrometry assays challenging. Ann Clin Biochem 2015;52:151-60.
Hollis BW, Kamerud JQ, Selvaag SR, Lorenz JD, Napoli JL. Determination of vitamin D status by radioimmunoassay with an 125I-labeled tracer. Clin Chem 1993;39:529-33.
Hollis BW, Frank NE. Solid phase extraction system for vitamin D and its major metabolites in human plasma. J Chromatogr 1985;343:43-9.
Omi K, Ando T, Sakyu T, Shirakawa T, Uchida Y, Oka A, et al. Noncompetitive immunoassay detection system for haptens on the basis of antimetatype antibodies. Clin Chem 2015;61: 627-35.
Saleh L, Mueller D, von Eckardstein A. Analytical and clinical performance of the new Fujirebio 25-OH vitamin D assay, a comparison with liquid chromatography-tandem mass spectrometry (LC-MS/MS) and three other automated assays. Clin Chem Lab Med 2016;54:617-25.
Van den Ouweland JM, Beijers AM, van Daal H, Elisen MG, Steen G, Wielders JP. Evaluation of 3-epi-25-hydroxyvitamin D3 cross-reactivity in the Roche Elecsys Vitamin D Total protein binding assay. Clin Chem Lab Med 2014;52:373-80.
Binkley N, Sempos CT. Standardizing vitamin D assays: the way forward. J Bone Min Res 2014;29:1709-14.
Tai SS, Bedner M, Phinney KW. Development of a candidate reference measurement procedure for the determination of 25-hydroxyvitamin D3 and 25-hydroxyvitamin D2 in human serum using isotope-dilution liquid chromatography-tandem mass spectrometry. Anal Chem 2010;82:1942-8.
Stepman HC, Vanderroost A, Van Uytfanghe K, Thienpont LM. Candidate reference measurement procedures for serum 25-hydroxyvitamin D3 and 25-hydroxyvitamin D2 by using isotope-dilution liquid chromatography-tandem mass spectrometry. Clin Chem 2011;57:441-8.
Stockl D, Sluss PM, Thienpont LM. Specifications for trueness and precision of a reference measurement system for serum/plasma 25-hydroxyvitamin D analysis. Clin Chim Acta 2009;408:8-13.
Cooke NE, Haddad JG. Vitamin D binding protein (Gc-globulin). Endocr Rev 1989;10:294-307.
Chun RF, Peercy BE, Orwoll ES, Nielson CM, Adams JS, Hewison M. Vitamin D and DBP: The free hormone hypothesis revisited. J Steroid Biochem Mol Biol 2013;144:132-7.
Hoofnagle AN, Eckfeldt JH, Lutsey PL. Vitamin D - binding protein concentrations quantified by mass spectrometry. N Engl J Med 2015;373:1480-2.
Johnsen MS, Grimnes G, Figenschau Y, Torjesen PA, Almas B, Jorde R. Serum free and bio-available 25-hydroxyvitamin D correlate better with bone density than serum total 25-hydroxyvitamin D. Scand J Clin Lab Invest 2014;74:1-7.
Bhan I, Powe CE, Berg AH, Ankers E, Wenger JB, Karumanchi SA, et al. Bioavailable vitamin D is more tightly linked to mineral metabolism than total vitamin D in incident hemodialysis patients. Kidney Int 2012;82:84-9.
Vermeulen A, Verdonck L, Kaufman JM. A critical evaluation of simple methods for the estimation of free testosterone in serum. J Clin Endocrinol Metab 1999;84:3666-72.
Powe CE, Ricciardi C, Berg AH, Erdenesanaa D, Collerone G, Ankers E, et al. Vitamin D-binding protein modifies the vitamin D-bone mineral density relationship. J Bone Min Res 2011;26:1609-16.
Rousseau A-F, Damas P, Janssens M, Kalin S, Ledoux D, Le Goff C, et al. Critical care and vitamin D status assessment: what about immunoassays and calculated free 25OH-D? Clin Chim Acta 2014;437:43-7.
Brumbaugh PF, Haussler MR. 1-alpha, 25 dihydroxycholecalcif- erol receptors in intestine. J Biol Chem 1974;249:1251-7.
Brumbaugh PF, Haussler DH, Bressler R, Haussler MR. Radioreceptor assay for 1 alpha,25-dihydroxyvitamin D3. Science 1974;183:1089-91.
Frolik CA, DeLuca HF. Solubilization and partial purification of a rat intestinal 1,25-dihydroxyvitamin d3 binding protein. Steroids 1975;26:683-5.
Eisman JA, Hamstra AJ, Kream BE, DeLuca HF. 1,25-Dihydroxy- vitamin D in biological fluids: a simplified and sensitive assay. Science 1976;193:1021-3.
De Leenheer AP, Bauwens RM. Radioimmunoassay for 1,25-dihydroxyvitamin D in serum or plasma. Clin Chem 1985;31:142-6.
Clemens TL, Hendy GN, Graham RF, Baggiolini EG, Uskokovic MR, O’Riordan JL. A radioimmunoassay for 1,25-dihydroxy- cholecalciferol. Clin Sci Mol Med 1978;54:329-32.
Hollis BW, Kamerud JQ, Kurkowski A, Beaulieu J, Napoli JL. Quantification of circulating 1,25-dihydroxyvitamin D by radioimmunoassay with an 125I-labeled tracer. Clin Chem 1996;42:586-92.
Seiden-Long I, Vieth R. Evaluation of a 1,25-dihydroxyvitamin D enzyme immunoassay. Clin Chem 2007;53:1104-8.
Hussein H, Ibrahim F, Boudou P. Evaluation of a new automated assay for the measurement of circulating 1,25-dihydroxyvitamin D levels in daily practice. Clin Biochem 2015;48:1160-2.
Denimal D, Lemaire-Ewing S, Duvillard L. Performance of a new 1,25-dihydroxyvitamin D fully automated assay on IDS-iSYS system. Clin Biochem 2015;48:1209-10.
Van Helden J, Weiskirchen R. Experience with the first fully automated chemiluminescence immunoassay for the quantification of 1a, 25-dihydroxy-vitamin D. Clin Chem Lab Med 2015;53:761-70.
Souberbielle J-C, Cavalier E, Delanaye P, Massart C, Brailly- Tabard S, Cormier C, et al. Serum calcitriol concentrations measured with a new direct automated assay in a large population of adult healthy subjects and in various clinical situations. Clin Chim Acta 2015;451:149-53.
Watson D, Setchell KD, Ross R. Analysis of vitamin D and its metabolites using thermospray liquid chromatography/mass spectrometry. Biomed Chrom. 1991;5:153-60.
Duan X, Weinstock-Guttman B, Wang H, Bang E, Li J, Ramana- than M, et al. Ultrasensitive quantification of serum vitamin D metabolites using selective solid-phase extraction coupled to microflow liquid chromatography and isotope-dilution mass spectrometry. Anal Chem 2010;82:2488-97.
Cashman KD, Hayes A, Galvin K, Merkel J, Jones G, Kaufmann M, et al. Significance of serum 24,25-dihydroxyvitamin D in the assessment of vitamin D status: a double-edged sword? Clin Chem 2015;61:636-45.
Higashi T, Shimada K, Toyo’oka T. Advances in determination of vitamin D related compounds in biological samples using liquid chromatography-mass spectrometry: a review. J Chroma- togr B 2010;878:1654-61.
El-Khoury JM, Reineks EZ, Wang S. Progress of liquid chromatography-mass spectrometry in measurement of vitamin D metabolites and analogues. Clin Biochem 2011;44:66-76.
Kamao M, Tatematsu S, Reddy GS, Hatakeyama S, Sugiura M, Ohashi N, et al. Isolation, identification and biological activity of 24R,25-dihydroxy-3-epi-vitamin D3: a novel metabolite of 24R,25-dihydroxyvitamin D3 produced in rat osteosarcoma cells (UMR 106). J Nutr Sci Vitaminol (Tokyo) 2001;47:108-15.
Ding S, Schoenmakers I, Jones K, Koulman A, Prentice A, Volmer DA. Quantitative determination of vitamin D metabolites in plasma using UHPLC-MS/MS. Anal Bioanal Chem 2010;398:779-89.
Wang Z, Senn T, Kalhorn T, Zheng XE, Zheng S, Davis CL, et al. Simultaneous measurement of plasma vitamin D(3) metabolites, including 4P,25-dihydroxyvitamin D(3), using liquid chromatography-tandem mass spectrometry. Anal Biochem 2011;418:126-33.
Van den Ouweland JM, Vogeser M, Bacher S. Vitamin D and metabolites measurement by tandem mass spectrometry. Rev Endocr Metab Disord 2013;14:159-84.
Burild A, Frandsen HL, Jakobsen J. Simultaneous quantification of vitamin D 3, 25-hydroxyvitamin D 3 and 24,25-dihydroxyvitamin D 3 in human serum by LC-MS/MS. Scand J Clin Lab Invest 2014;74:418-23.
Volmer DA, Mendes LR, Stokes CS. Analysis of vitamin D metabolic markers by mass spectrometry: current techniques, limitations of the “gold standard” method, and anticipated future directions. Mass Spectrom Rev 2015;34:2-23.
Qi Y, Geib T, Schorr P, Meier F, Volmer DA. On the isobaric space of 25-hydroxyvitamin D in human serum: potential for interferences in liquid chromatography/tandem mass spectrometry, systematic errors and accuracy issues. Rapid Communications in Mass Spectrom 2015;29:1-9.
Lewandowski CM, Taylor A, Susarla R, Keevil B, Kilby M, Hewison M. A high throughput LC-MS/MS method for the analysis of multiple vitamin D analytes in serum and solid tissues using supported liquid-liquid extraction. MSACL 2016;1:24-5.
Casetta B, Jans I, Billen J, Vanderschueren D, Bouillon R. Development of a method for the quantification of 1alpha,25(OH)2- vitamin D3 in serum by liquid chromatography tandem mass spectrometry without derivatization. Eur J Mass Spectrom 2010;16:81-9.
Raml R, Ratzer M, Obermayer-Pietsch B, Mautner A, Pieber TR, Sinner FM, et al. Quantifying vitamin D and its metabolites by LC/Orbitrap MS. Anal Methods 2015;7:8961-6.
Vreeken RJ, Honing M, van Baar BL, Ghijsen RT, de Jong GJ, Brinkman UA. On-line post-column Diels-Alder derivatization for the determination of vitamin D3 and its metabolites by liquid chromatography/thermospray mass spectrometry. Biol Mass Spectrom 1993;22:621-32.
Aronov P, Hall LM, Dettmer K, Stephensen CB, Hammock BD. Metabolic profiling of major vitamin D metabolites using Diels- Alder derivatization and ultra-performance liquid chromatography-tandem mass spectrometry. Anal Bioanal Chem 2008;391:1917-30.
Yuan C, Kosewick J, He X, Kozak M, Wang S. Sensitive measurement of serum 1alpha,25-dihydroxyvitamin D by liquid chromatography/tandem mass spectrometry after removing interference with immunoaffinity extraction. Rapid Commun Mass Spectrom 2011;25:1241-9.
Higashi T, Awada D, Shimada K. Determination of 24,25-dihydroxyvitamin D3 in human plasma using liquid chromatography-mass spectrometry after derivatization with a Cookson-type reagent. Biomed Chrom 2001;15:133-40.
Kaufmann M, Gallagher JC, Peacock M, Schlingmann KP, Konrad M, DeLuca HF, et al. Clinical utility of simultaneous quantitation of 25-hydroxyvitamin D and 24,25-dihydroxyvitamin D by LC-MS/MS involving derivatization with DMEQ-TAD. J Clin Endocrinol Metab 2014;99:2567-74.
Ogawa S, Ooki S, Morohashi M, Yamagata K, Higashi T. A novel Cookson-type reagent for enhancing sensitivity and specificity in assessment of infant vitamin D status using liquid chromatography/tandem mass spectrometry. Rapid Commun Mass Spectrom 2013;27:2453-60.
Ogawa S, Ooki S, Shinoda K, Higashi T. Analysis of urinary vitamin D3 metabolites by liquid chromatography/tandem mass spectrometry with ESI-enhancing and stable isotope-coded derivatization. Anal Bioanal Chem 2014;406:6647-54.
Hedman CJ, Wiebe DA, Dey S, Plath J, Kemnitz JW, Ziegler TE. Development of a sensitive LC/MS/MS method for vitamin D metabolites: 1,25 Dihydroxyvitamin D2&3 measurement using a novel derivatization agent. J Chromatogr B 2014;953- 954:62-7.
Chan N, Kaleta EJ. Quantitation of 1a,25-dihydroxyvitamin D by LC-MS/MS using solid-phase extraction and fixed-charge derivitization in comparison to immunoextraction. Clin Chem Lab Med 2015;53:1399-407.
Strathmann FG, Laha TJ, Hoofnagle AN. Quantification of 1, 25-dihydroxy vitamin D by immunoextraction and liquid chromatography-tandem mass spectrometry. Clin Chem 2011;57:1279-85.
Biotage. Application Note AN812.V.2. Extraction of 1,25 di-OH Vitamin D2, 1,25 di-OH Vitamin D3, 25 OH Vitamin D2 and 25 OH Vitamin D3 from serum Using ISOLUTE® SLE+ prior to LC-MS/MS Analysis Extraction of 1,25 di-OH Vitamin D2, 1,25 di-OH Vitamin D3, 25 OH Vitam 2014.
Mata-Granados JM, Ferreiro-Verab C, Luque de Castro MD, Que- sada Gomez JM. Determination of the principal metabolites of vitamin D in blood by means of on-line solid phase extraction with liquid chromatography-tandem mass spectrometry. Rev Osteoporos Metab Miner 2010;2:55-61.
Mena-Bravo A, Ferreiro-Vera C, Priego-Capote F, Maestro MA, Mourino A, Quesada-Gomez JM, et al. Quantitative analytical method to evaluate the metabolism of vitamin D. Clin Chim Acta 2015;442:6-12.
Tai SS, Nelson M. Candidate reference measurement procedure for the determination of (24 R),25-dihydroxyvitamin D3 in human serum using isotope-dilution liquid chromatography-tandem mass spectrometry. Anal Chem 2015;87: 7964-70.
Mena-Bravo A, Priego-Capote F, de Castro MD. Study of blood collection and sample preparation for analysis of vitamin D and its metabolites by liquid chromatography-tandem mass spectrometry. Anal Chim Acta 2015;879:69-76.
Dey S, Pillal S, Willamson BL, Purkayastha S. Patent US 2014/0127825 A1. Quantitative analysis of vitamin D3, vitamin D2, and metabolites thereof 2014.
Vukovic J. Patent US2015/0308987 A1. Methods and apparatus for the analysis of vitamin D metabolites 2015.