No vitamin D test needed before supplementing (typically)
Testing vitamin D levels
Canadian Family Physician VOL 60: APRIL • AVRIL 2014
Adrienne J. Lindblad acpr PharmD Scott Garrison md PhD James McCormack PharmD
Dr Lindblad is Knowledge Translation and Evidence Coordinator with the Alberta College of Family Physicians.
Dr Garrison is Associate Professor in the Department of Family Medicine at the University of Alberta in Edmonton.
Dr McCormack is Professor in the Faculty of Pharmaceutical Sciences at the University of British Columbia in Vancouver.
The opinions expressed in this Tools for Practice article are those of the authors and do not necessarily mirror the perspective and policy of the Alberta College of Family Physicians.
Clinical question
What is the evidence for testing serum vitamin D (VTD) levels in adults?
Bottom line
Routine testing of VTD levels is unnecessary. Laboratories often report serum VTD levels between 50 and 80 nmol/L to be insufficient, but this claim is not supported by evidence. Additionally, large variability in testing limits interpretation of repeat measurements.
Evidence
A systematic review1 on 25-hydroxyvitamin D (25[OH] D) suggests levels greater than 75 nmol/L "are not consistently associated with increased benefit"; greater than 50 nmol/L are "practically sufficient for all persons"; between 30 and 50 nmol/L "places some, but not all, persons at risk for inadequacy"; and less than 30 nmol/L puts one "at risk relative to bone health."
No RCTs in falls or fractures investigated treating specific VTD level targets.
The proportions of the Canadian, American, and British populations with 25(OH)D levels less than 75 to 80 nmol/L are 97%, 77%, and 87%, respectively2-4; but this is not necessarily a concerning level, according to the systematic review.1 However, of potential concern, 61% of Canadians had levels less than 50 nmol/L,2 and 13% had levels less than 40 nmol/L.1
Context
Some provincial laboratories5 consider 25(OH)D levels of 74 nmol/L or less to be "insufficient," but this is not supported by the evidence.
Every 800 IU of VTD increases 25(OH)D by 8 to 16 nmol/L; however, the dose-response relationship is not directly linear and is affected by many factors (eg, season, adiposity, skin pigmentation).1,6
Vitamin D assays have a coefficient of variation that might be as high as 10% to 20%,1 meaning changes in levels with doses of 800 IU/d might not be discernible owing to variability in testing.
Guidelines7 suggest supplementing without testing, and explain when testing might be helpful.
Mega VTD doses (ie, 150 000 IU every 3 months) have been associated with increased adverse events (eg, falls, fractures).8,9
In trials, enrolment was not based on VTD levels and treating on speculation was beneficial10,11; doses were not adjusted based on VTD levels.12-14
A 25(OH)D assay costs $61.32.15
Implementation
Routine VTD testing is not required or recommended; however, testing might be beneficial for some when clinically indicated: those with
parathyroid disease,
hypocalcemia,
hypercalcemia,
hyperphosphatemia,
serious renal or liver disease, or
malabsorption syndromes;
those taking medications that affect VTD metabolism (eg, valproate) or absorption (eg, cholestyramine); or
those with possible hypervitaminosis D.7
Do not test calcitriol levels unless 1-a-hydroxylase abnormality is suspected.1,7
Patients older than age 50 can take 800 to 1000 IU/d of VTD to reduce the risk of falls, fractures, and overall mortality.16 &
References
1. Ross AC, Taylor CL, Yaktine AL, Del Valle HB, editors. Dietary reference intakes for calcium and vitamin D. Washington, DC: National Academies Press; 2011.
2. Rucker D, Allan JA, Fick GH, Hanley DA. Vitamin D insufficiency in a population of healthy western Canadians. CMAJ 2002;166(12):1517-24. Erratum in: CMAJ 2002;167(8):850.
3. Hypponen E, Power C. Hypovitaminosis D in British adults at age 45 y: nationwide cohort study of dietary and lifestyle predictors. Am J Clin Nutr 2007;85(3):8608.
4. Ginde AA, Liu MC, Camargo CA Jr. Demographic differences and trends of vitamin D insufficiency in the US population, 1988-2004. Arch Intern Med 2009;169(6):626-32.
5. BC Biomedical Laboratories [website]. Adult reference ranges. Surrey, BC: BC Biomedical Laboratories; 2014. http://198.71.215.83/refranges/Laboratory%20Adult%20Reference%20Intervals.pdf. Accessed 2013 Nov 18.
6. Moyad MA. Vitamin D: a rapid review. Dermatol Nurs 2009;21(1):25-30, 55.
7. Toward Optimized Practice [website]. Guideline for vitamin D testing and supplementation in adults. Edmonton, AB: Toward Optimized Practice; 2012. www.topalbertadoctors.org/cpgs/28048723. Accessed 2013 Nov 18.
8. Sanders KM, Stuart AL, Williamson EJ, Simpson JA, Kotowicz MA, Young D, et al. Annual high-dose oral vitamin D and falls and fractures in older women: a randomized, controlled trial. JAMA 2010;303(18):1815-22. Erratum in: JAMA 2010;303(23):2357.
9. Glendenning P, Zhu K, Inderjeeth C, Howat P, Lewis JR, Prince RL. Effects of three-monthly oral 150,000 IU cholecalciferol supplementation on falls, mobility, and muscle strength in older postmeno-pausal women: a randomized controlled trial. J Bone Miner Res 2012;27(1):170-6.
10. Bischoff-Ferrari HA, Willett WC, Wong JB, Stuck AE, Staehelin HB, Orav EJ, et al. Prevention of non-vertebral fractures with oral vitamin D and dose dependency: a meta-analysis of randomized controlled trials. Arch Intern Med 2009;169(6):551-61.
11. Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC, Staehelin HB, Bazemore MG, Zee RY, et al. Effect of Vitamin D on falls: a meta-analysis. JAMA 2004;291(16):1999-2006.
12. Chapuy MC, Arlot ME, Duboeuf F, Brun J, Crouzet B, Arnaud S, et al. Vitamin D3 and calcium to prevent hip fractures in the elderly women. N Engl J Med 1992;327(23):1637 2.
13. Trivedi DP, Doll R, Khaw KT. Effect of four monthly oral vitamin D3 (cholecalciferol) supplementation on fractures and mortality in men and women living in the community: randomised double blind controlled trial. BMJ 2003;326(7387):469.
14. Grant AM, Avenell A, Campbell MK, McDonald AM, MacLennan GS, McPherson GC, et al. Oral vitamin D3 and calcium for secondary prevention of low-trauma fractures in elderly people (Randomised Evaluation of Calcium Or vitamin D, RECORD): a randomised placebo-controlled trial. Lancet 20005;365(9471):1621-8.
15. Guidelines and Protocols Advisory Committee. Vitamin D testing protocol. Victoria, BC: British Columbia Medical Association; 2013.
16. Allan GM, Korownyk C. What is the benefit of vitamin D: trend or treat? In: Tools for Practice [website]. Edmonton, AB: ACFP; 2009. Available from: www.acfp.ca/docs09/ToolsforPracticeInfoforWebsiteOct192009.pdf. Accessed 2014 Mar 10.
Tools for Practice articles in Canadian Family Physician (CFP) are adapted from articles published on the Alberta College of Family Physicians (ACFP) website, summarizing medical evidence with a focus on topical issues and practice-modifying information. The ACFP summaries and the series in CFPare coordinated by Dr G. Michael Allan, and the summaries are co-authored by at least 1 practising family physician and are peer reviewed. Feedback is welcome and can be sent to toolsforpractice@cfpc.ca. Archived articles are available on the ACFP website: www.acfp.ca.
See also VitaminDWiki
No longer debating vitamin D supplementation, now debating need for testing first – April 2013
50,000 IU monthly safe to take without any vitamin D testing – RCT Dec 2013
80 X increase in Vitamin D testing in Australia in a decade - June 2013
Vitamin D testing typically not needed, but in 9 cases it is – April 2012 probably the similar exclusions as listed in the article on this page
Quick, FREE, self-test for Vitamin D deficiency approx < 15 ng
Active level of vitamin D are not indicated by standard blood tests - Sept 2012
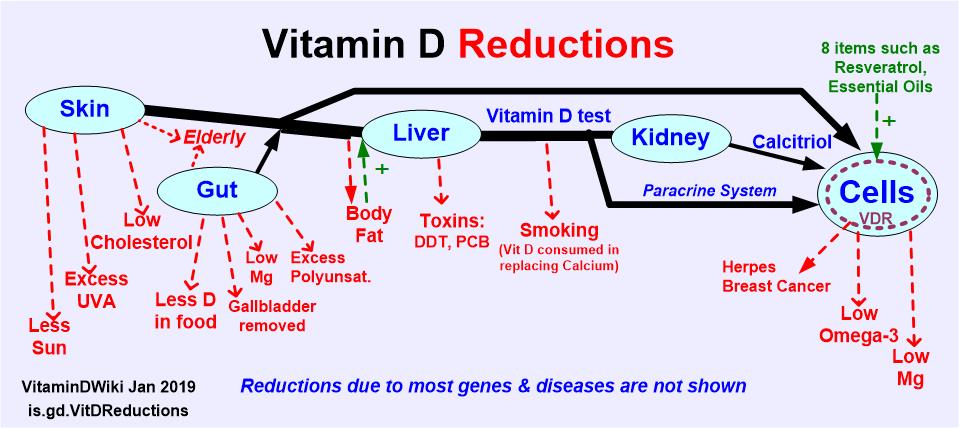
Vitamin D reduced so low that Victorian age diseases are returning has the following chart
- some people can have OK blood test level but have little vitamin D getting into cells - due to poor kidney, low Omega-3, lack Magnesium, genes, etc