Cystic Fibrosis appears associated with poor Vitamin D genes (radioactive tracing)
METABOLISM AND PHARMACOKINETICS OF VITAMIN D in PATIENTS with Cystic Fibrosis
J. of Steroid Biochemistry and Molecular Biology https://doi.org/10.1016/j.jsbmb.2023.106332
lMackenzie C. Bergagnini-Kolev a 1 2, Simon Hsu b c 2, Moira L. Aitken d, Christopher H. Goss e f, Andrew N. Hoofnagle b g, Leila R. Zelnick b c, Dawn Lum b c, Cora M. Best b g 3, Kenneth E. Thummel a, Bryan R. Kestenbaum b c, Ian H. de Boer b c, Yvonne S. Lin a
Abstract
Patients with cystic fibrosis (CF) commonly have lower circulating concentrations of 25-hydroxyvitamin D (25(OH)D) than healthy populations. We comprehensively compared measures of vitamin D metabolism among individuals with CF and healthy control subjects.
In a cross-sectional study, serum from participants with CF (N=83) and frequency-matched healthy control subjects by age and race (N=82) were analyzed for: 25(OH)D2 and 25(OH)D3, 1α,25-dihydroxyvitamins D2 and D3 (1α,25(OH)2D2 and 1α,25(OH)2D3), 24,25-dihydroxyvitamin D3 (24,25(OH)2D3), 4β,25-dihydroxyvitamin D3 (4β,25(OH)2D3), 25-hydroxyvitamin D3-3-sulfate (25(OH)D3-S), and 25-hydroxyvitamin D3-3-glucuronide (25(OH)D3-G). In a 56-day prospective pharmacokinetic study,
~25 μg deuterium-labeled 25(OH)D3 (d6-25(OH)D3) was administered intravenously to participants (N=5 with CF, N=5 control subjects). Serum was analyzed for d6-25(OH)D3 and d6-24,25(OH)2D3, and pharmacokinetic parameters were estimated.
In the cross-sectional study, participants with CF had similar mean (SD) total 25(OH)D concentrations as control subjects (26.7 [12.3] vs. 27.7 [9.9] ng/mL) and had higher vitamin D supplement use (53% vs. 22%).
However, participants with CF had lower total
1α,25(OH)2D (43.6 [12.7] vs. 50.7 [13.0] pg/mL),
4β,25(OH)2D3 (52.1 [38.9] vs. 79.9 [60.2] pg/mL), and
25(OH)D3-S (17.7 [11.6] vs. 30.1 [12.3] ng/mL) (p < 0.001 for all).
The pharmacokinetics of d6-25(OH)D3 and d6-24,25(OH)D3 did not differ between groups. In summary, although 25(OH)D concentrations were comparable,
participants with CF had lower 1α,25(OH)2D, 4β,25(OH)2D3, and 25(OH)D3-S concentrations than healthy controls.
Neither 25(OH)D3 clearance, nor formation of 24,25(OH)2D3, appears to account for these differences and alternative mechanisms for low 25(OH)D in CF (i.e., decreased formation, altered enterohepatic recirculation) should be explored.
Introduction
Vitamin D deficiency, defined by low circulating concentrations of 25-hydroxyvitamin D (25(OH)D), is ubiquitous in patients with cystic fibrosis (CF) [1]. Most patients with this disorder require vitamin D supplementation, often at high doses, to maintain physiologically normal 25(OH)D concentrations. Vitamin D deficiency in patients with CF is associated with low bone mineral density, impaired innate and acquired immunity, and increased risk of pulmonary complications [1], [2], [3]. These problems are further compounded due to decreased ability to exercise, malnutrition due to poor absorption of nutrients, and use of corticosteroids [2], [3]. The Cystic Fibrosis Foundation recommends a target 25(OH)D of > 30 ng/mL (75 nM) [4]. However, up to 90% of persons with CF do not achieve this recommended threshold despite routine supplementation [2], [4], [5], [6], [7], and the specific mechanisms by which their 25(OH)D concentrations remain low are poorly understood.
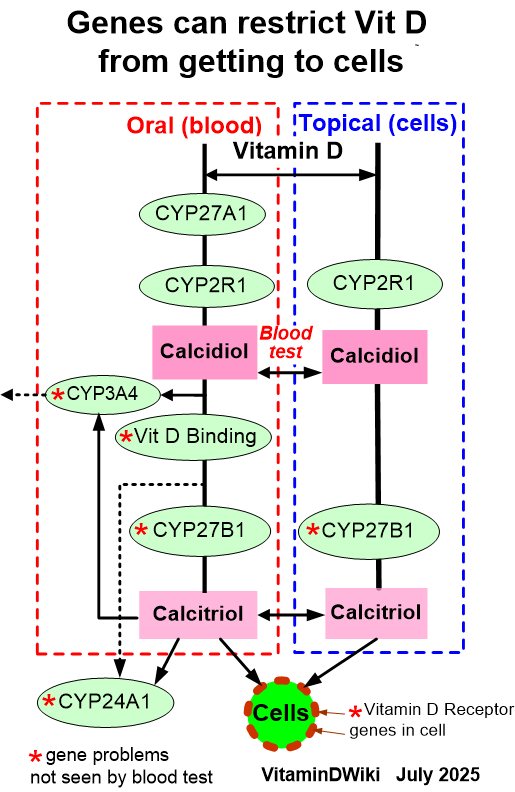
Vitamin D exists in two primary forms: vitamin D2 and vitamin D3, both of which follow similar pathways of metabolism [6], [8] (Figure S1). Derived mostly from sunlight, vitamin D is converted in the liver to 25(OH)D, the most widely used biomarker of long-term vitamin D exposure due to its long plasma half-life of 2 to 3 weeks [8], [9]. 25(OH)D3, which is more abundant than 25(OH)D2, undergoes metabolism by cytochrome P450 (CYP) 27B1, also called 1α-hydroxylase, to form the biologically active 1α,25-dihydroxyvitamin D3 (1α,25(OH)2D3) [7], [10] (Figure S1). 25(OH)D3 may also be cleared from the blood through hydroxylation or conjugation into several inactive metabolites [11]: 24 R,25-dihydroxyvitamin D3 (24,25(OH)2D3, the most abundant metabolite of 25(OH)D clearance) [7], [10], 1β,25-dihydroxyvitamin D3 [12], 4β,25-dihydroxyvitamin D3 (4β,25(OH)2D3) [13], 25-hydroxyvitamin D3-3-sulfate (25(OH)D3-S) [14], and 25-hydroxyvitamin D3-3-glucuronide (25(OH)D3-G) [15] (Figure S1).
Numerous mechanisms for low 25(OH)D in persons with CF have been hypothesized: reduced time outdoors, poor intestinal absorption of fat-soluble vitamins such as vitamin D, reduced capacity to hydroxylate vitamin D in the liver, reduced storage capacity due to low body fat [1], impaired enterohepatic recirculation of vitamin D metabolites enhancing their loss [18], urinary loss of vitamin D binding protein (VDBP) and albumin (the major carriers of vitamin D metabolites) [16], and increased 1α-hydroxylase expression in pulmonary epithelial cells that drive 1α,25(OH)2D formation from 25(OH)D [17]. Understanding the specific pathways that contribute to low circulating 25(OH)D concentrations in CF may improve how we assess and treat vitamin D-related complications of CF. Thus, we investigated the hypothesis that individuals with CF have altered concentrations of multiple vitamin D metabolites and increased clearance of 25(OH)D.
Section snippets
Study Design
We conducted two complementary studies to increase the understanding of vitamin D metabolism in CF. First, we compared a comprehensive set of vitamin D metabolites between participants with CF and healthy control subjects in a cross-sectional study. Second, we determined the pharmacokinetics of vitamin D metabolism by administering intravenous deuterium-labeled 25-hydroxyvitamin D3 (d6-25(OH)D3) to participants with CF and healthy controls. Both studies were approved by the University of
Participant Characteristics
In total, 83 participants with CF and 82 healthy controls were enrolled (Table 1). The mean age for both groups was similar, but the percentage of males in the healthy controls was lower than that of the CF group (38% vs. 55%). More than 85% of participants with CF had a clinical diagnosis of pancreatic insufficiency, and 53% were receiving vitamin D supplementation compared with 22% of healthy controls. Approximately 50% and 40% of the participants with CF were homozygous and heterozygous for….
Discussion
The present investigation is one of the first to evaluate a comprehensive set of vitamin D metabolites and the pharmacokinetics of 25(OH)D in adults with CF. Only 35% of participants with CF had total 25(OH)D concentrations greater than or equal to the guideline-recommended threshold of 30 ng/mL despite over 50% of them taking vitamin D supplements. Of the metabolites studied, concentrations of total 1α,25(OH)2D, 4β,25(OH)2D3, and 25(OH)D3-S were lower in participants with CF than in healthy….
Conclusions
Compared with healthy participants, those with CF had lower total 1α,25(OH)2D, 4β,25(OH)2D3 and 25(OH)D3-S, perhaps as a consequence of decreased formation in CF. As there were no differences in the systemic clearance or half-life of d6-25(OH)D3 between our two study groups, increased 25(OH)D3 elimination or formation of 24,25(OH)2D3 are unlikely to contribute to low 25(OH)D concentrations in persons with CF. Other factors that may explain 25(OH)D deficiency in CF, such as altered absorption of ….
Funding
This work was supported in part by grants from the National Institutes of Health: P30 DK089507, P30 DK035816, P30 DK017047, R01 DK099199, T32 GM007750 (to MCB), T32 DK007467-36 (to SH), and by an unrestricted fund from the Northwest Kidney Centers.
CRediT authorship contribution statement
Mackenzie C. Bergagnini-Kolev: Methodology, Formal analysis, Writing – Original Draft, Writing – Review & Editing; Simon Hsu: Writing – Review & Editing; Moira L. Aitken: Conceptualization, Investigation, Writing – Review & Editing; Christopher H. Goss: Conceptualization, Investigation, Writing – Review & Editing; Hoofnagle: Conceptualization, Methodology, Writing – Review & Editing; Leila R. Zelnick: Formal analysis, Data Curation, Writing – Review & Editing; Dawn Lum: Investigation, Data
Declarations of interest: none
Acknowledgements" We thank the participants of the CLEAR-CF and SKS studies for their participation.
Some of the 31 references are available online
VitaminDWiki – Cystic Fibrosis category listing contains
{include}
Any of 4 poor genes (marked with red star) can cause the altered Vitami D metabolism seen in this study