Zika cost-effectiveness calculator
http://zika.cidma.us/
Described at ScienceCodex
"The researchers estimated that between 50 and 210 out of every 10,000 mothers who are infected with Zika will deliver a child with microcephaly."
"For GBS, between 2 and 8 of every 10,000 people infected with Zika are estimated to experience this complication."
"The study predicts that if 40% of the population in Latin America and the Caribbean become infected with Zika,
- there could be more than 22,000 babies born with microcephaly"
- "In previous Zika outbreaks in Micronesia and Polynesia, more than 66% of the population became infected with Zika."
Screenshots of the calculator
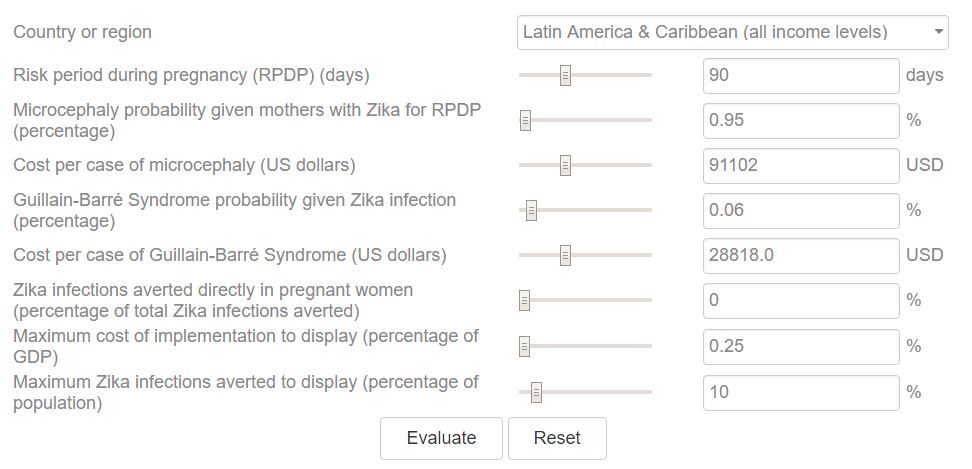
A Cost-Effectiveness Tool for Informing Policies on Zika Virus Control
PLOS x, : May 20, 2016http://dx.doi.org/10.1371/journal.pntd.0004743
Jorge A. Alfaro-Murillo , Alyssa S. Parpia , Meagan C. Fitzpatrick , Jules A. Tamagnan, Jan Medlock, Martial L. Ndeffo-Mbah, Durland Fish, María L. Ávila-Agüero, Rodrigo Marín, Albert I. Ko, Alison P. Galvani
Background
As Zika virus continues to spread, decisions regarding resource allocations to control the outbreak underscore the need for a tool to weigh policies according to their cost and the health burden they could avert. For example, to combat the current Zika outbreak the US President requested the allocation of $1.8 billion from Congress in February 2016.
Methodology/Principal Findings
Illustrated through an interactive tool, we evaluated how the number of Zika cases averted, the period during pregnancy in which Zika infection poses a risk of microcephaly, and probabilities of microcephaly and Guillain-Barré Syndrome (GBS) impact the cost at which an intervention is cost-effective. From Northeast Brazilian microcephaly incidence data, we estimated the probability of microcephaly in infants born to Zika-infected women (0.49% to 2.10%). We also estimated the probability of GBS arising from Zika infections in Brazil (0.02% to 0.06%) and Colombia (0.08%). We calculated that each microcephaly and GBS case incurs the loss of 29.95 DALYs and 1.25 DALYs per case, as well as direct medical costs for Latin America and the Caribbean of $91,102 and $28,818, respectively. We demonstrated the utility of our cost-effectiveness tool with examples evaluating funding commitments by Costa Rica and Brazil, the US presidential proposal, and the novel approach of genetically modified mosquitoes. Our analyses indicate that the commitments and the proposal are likely to be cost-effective, whereas the cost-effectiveness of genetically modified mosquitoes depends on the country of implementation.
Conclusions/Significance
Current estimates from our tool suggest that the health burden from microcephaly and GBS warrants substantial expenditures focused on Zika virus control. Our results justify the funding committed in Costa Rica and Brazil and many aspects of the budget outlined in the US president’s proposal. As data continue to be collected, new parameter estimates can be customized in real-time within our user-friendly tool to provide updated estimates on cost-effectiveness of interventions and inform policy decisions in country-specific settings.
Author Summary
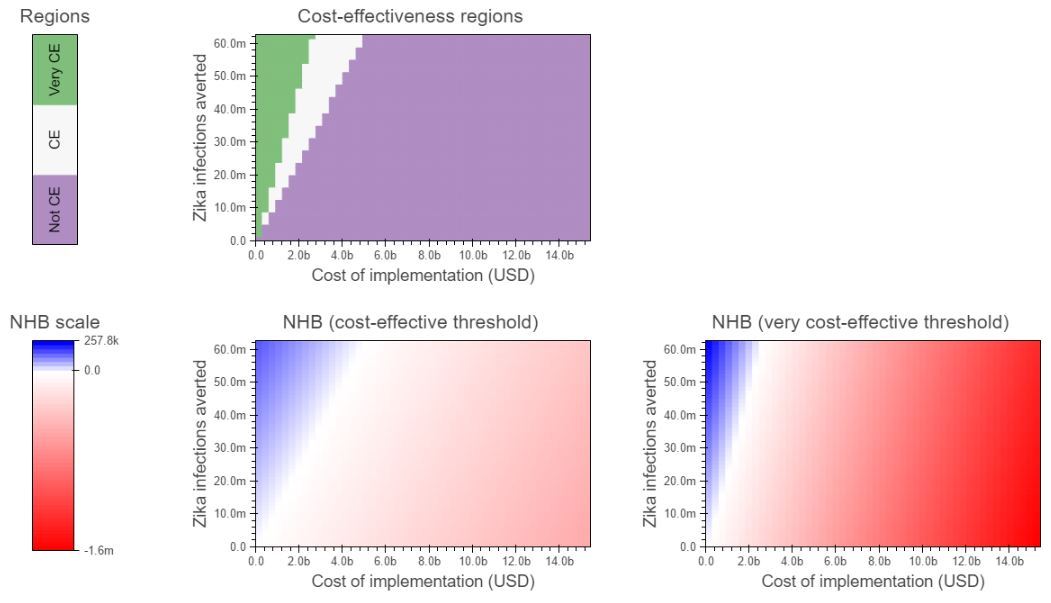
Using data on Zika virus, microcephaly, and Guillain-Barré syndrome cases from Brazil and Colombia, we compute ranges for the probability of a microcephaly outcome in infants born to Zika-infected women (0.49% to 2.10%, based on data from Northeast Brazil) and the probability of Guillain-Barré syndrome in Zika-infected individuals (0.02% to 0.06% in Brazil and 0.08% in Colombia). These results have allowed us to create a web-based cost-effectiveness tool that quantifies the relationship between the cost of an intervention and the number of Zika virus cases, as well as loss of disability-adjusted life years, that it can avert. Our tool thus identifies the threshold at which a given intervention, such as vector control, may be deemed cost-effective or very cost-effective in a variety of settings according to WHO criteria, in terms of the Zika burden that could be averted and the cost of such an intervention.
From the PDF
"For example, our base case analysis suggests that an intervention that prevents 10,000,000 Zika infections across Latin America and the Caribbean, corresponding to 1.6% of the population, would be cost-effective for expenditures below $802 million and very cost-effective below $409 million, using the average regional per capita GDP and birth rate."
"We calculated that 13,490 pregnant women are at risk of Zika infection if the outbreak is unabated in Puerto Rico. . ."
". IF an intervention is able to avert 90% of those infections (in Puerto Rico) in pregnant women, it would be cost-effective at $195.4 million"
- This is 12,141 for $195.4 million = $17,000 per pregnancy to avert both microcephaly, and Guillain-Barré syndrome
- Note: Versus less than $17 per pregnancy for Vitamin D (1000 times less costly)
Study ignored Congenital Zika infection associated with: vision-threatening ocular lesions , in utero growth restriction, fetal death, stillbirth, and central nervous system lesions, etc.
Study did not include indirect costs - which they estimated as 7 TIMES higher than the medical costs
“very cost-effective” = 1X of per capitia GDP; "cost-effective,” = 3X of per capita GDP
- Map of per capita GDP from Wikipedia
