Autism, Vitamin D, and serotonin - Patrick interview by Mercola
Interview with Dr. Rhonda Patrick
By Dr. Joseph Mercola
Interview with Mercola including the following sections and a video
Vitamin D Is an Important Gene Regulator
Autism Has Risen in Tandem With Vitamin D Deficiency
Gut Versus Brain Serotonin
Vitamin D Keeps Gut Serotonin in Check
The Role of Serotonin During Early Brain Development
Maternal Autoimmunity and Autism
Vitamin D Deficiency Can Fuel Autoimmune Response During Pregnancy
Serotonin in the gut and in the placenta
Common Gene Polymorphism Predisposes Many to Low Vitamin D Levels
 The TOP articles in Autism and Vitamin D are listed here:
{category}
Autism treated by Vitamin D: Dr. Cannell - video June 2013
includes many reasons why he believes Autism is related to Vitamin D
{include}
The TOP articles in Autism and Vitamin D are listed here:
{category}
Autism treated by Vitamin D: Dr. Cannell - video June 2013
includes many reasons why he believes Autism is related to Vitamin D
{include}
Transcript serotonin occurs 52 times, vitamin d occurs 91 times
JM: Dr. Joseph Mercola
RP: Rhonda Patrick

JM: Autism, an increasing epidemic, 200 times increase from when I first started practicing. Are there simple preventive approaches other than vaccines? Hi, this is Dr. Mercola, helping you take control of your health. Today I am joined by a delightful biological scientist, Dr. Rhonda Patrick, who is just a pleasure to interact with. She’s published two papers that really expand on some very exciting, simple, simple but powerful lifestyle interventions that could have profound influence not only on autism but a variety of other developmental disorders in childhood. Welcome today and thank you for joining us, Dr. Patrick.
RP: Thank you for having me, Dr. Mercola.
JM: Just fascinating work you’ve done, basically impacting simple things like vitamin d and nutrients in the diet. We’ve heard about the influence in vitamin d and autism before but only from a superficial level. But what you’ve done in your studies is you’ve really dug deep and have come up with just a brilliant hypothesis. It seems to have quite a significant validity to it. I’m wondering if you could pave the way for us and help explain what you found.
RP: Absolutely. I think usually before I get into how vitamin d may be playing a role in autism, I like to kind of explain just briefly what vitamin d is.
JM: Sure.
RP: It’s kind of important to understanding how it may play a role in brain function or brain dysfunction. Despite the name, vitamin d , it actually gets converted into a steroid hormone. Estrogen is a steroid hormone, testosterone is a steroid hormone, and vitamin d gets converted into a steroid hormone. It actually regulates over a thousand different physiological processes inside the body, which is a lot. It’s actually controlling around 5 percent of the human genome. That’s a pretty significant amount.
JM: I know you say those numbers, and I don’t dispute them, but Dr. Holick, who’s really one of the leaders in vitamin d research, he thinks it’s twice as many. I specifically asked him that when I was with him last because you had mentioned it was 5 percent. He’s convinced it’s 10 percent. Any idea what the difference is on the opinion on that?
RP: I think there is some emerging literature that’s showing now there may be even twice as many different genes that contain a little tell-tell sequence in their DNA that vitamin d ... When you have enough vitamin d in the body, it binds to something called the vitamin d receptor. It’s kind of like when you have a key and you put it in a lock. It fits just right, you turn the lock, and it opens the door. vitamin d , when there’s enough around in the body, it binds to something called the vitamin d receptor, and it fits just right. When they’re bound together, they can unlock a lot of things in the body.
The way it does that is this vitamin d receptor complex can go deep inside the DNA. It recognizes this little tell-tell sequence like a little code. The code itself can tell this vitamin d receptor complex to either turn the gene on so the gene is active (it’s even more active and it’s doing a certain function), or it can tell it, “Hey, let’s turn things down. I know you’re here, but we don’t need as much of you active.” It actually turns the gene down. Even though the gene is there, it’s almost like it’s not there because it’s not as active. The sequence itself, that little tell-tell sequence, it can tell it on or off.
With respect to Dr. Holick and him thinking that maybe vitamin d is important for regulating maybe even 10 percent of the human genome, that’s because there is now new emerging evidence that shows those little tell-tell sequence are even in as twice as many genes. But it hasn’t been empirically shown that indeed it does activate or not, or turn it off.
JM: OK.
RP: I think I agree with Dr. Holick that it’s very likely that it may be controlling even more than what we know.
JM: It’s a profound influence. There’s no question. We’ve probably just only began to appreciate the tip of the iceberg of its influence. Eventually, investigators, like yourself, will uncover even more of the details on how it impacts our health. Thank you for expanding on that and answering my question. I’ll let you continue.
RP: And it’s so relevant because so many people are not getting enough vitamin d . I think it has huge relevance. You mentioned that autism had been increasing about 20 0...
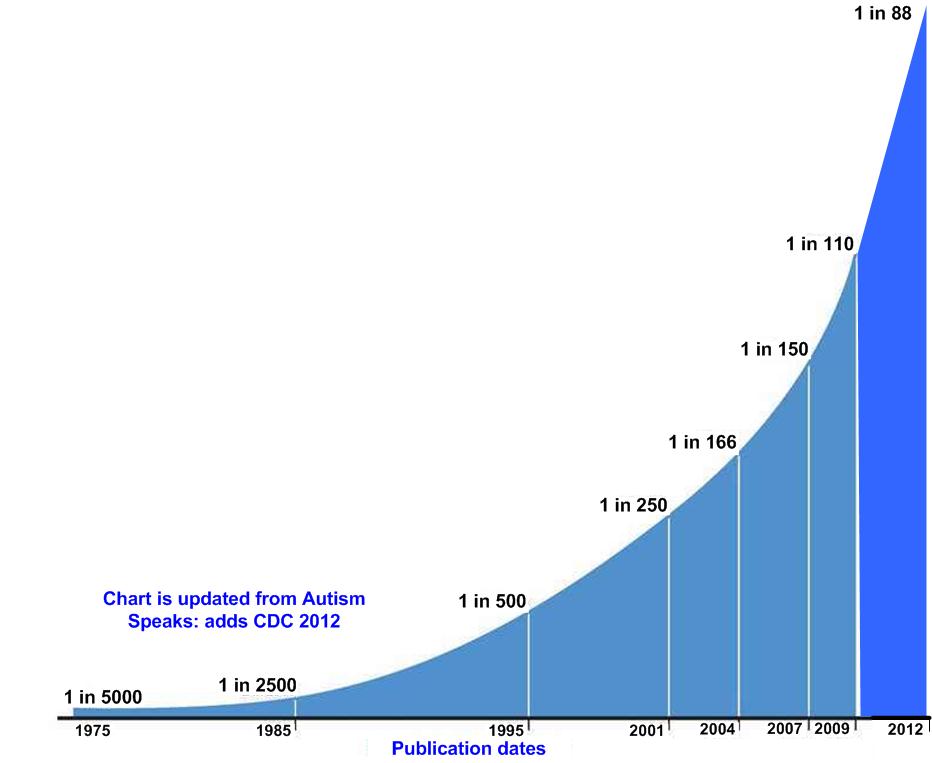
JM: 200-fold. It was 1 in 10,000 when I was in medical school. Now it’s about. The studies vary. The minimum is about 1 in 60. I’ve seen estimates from the Centers for Disease Control (CDC) for as low as 1 in 30.
RP: Wow.
JM: Here’s what’s even more frightening: the projections from reputable experts are suggesting that within 10 to 20 years, it’s going to be half if the trend continues - 1 in 2 kids will have some type of autistic disorder. How can a culture continue to thrive if half the kids’ brains aren’t functioning? It can’t. It’s just a prescription for disaster.
RP: Yeah. It’s been increasing by like 500 percent since the 1970s. Yes, there is a very strong component of increased awareness. More people are becoming aware, so diagnoses are increasing. But that just can’t account for the exponential increase in autism incidence.
I’m coming from this vitamin d angle. At the same time this autism incidence is going up, the vitamin d deficiency has been going up. Or you can look at it the other way. vitamin d sufficiency has been going down. There’s that correlation between autism incidence rising and vitamin d deficiency rising largely as a consequence of people wearing sunscreens. UVB radiation is very important to make vitamin d in the skin. And also staying indoors more, computer screens, and televisions. There are many different factors that are playing a role in that.
But as I mentioned, vitamin d has been shown to control at least 5 percent of the human genome, and it may even be much more than that. What I found and what my research identified when I was at Children’s Hospital Oakland Research Institute (CHORI) with Dr. Bruce Ames, is that one of those genes that vitamin d is regulating is a gene that encodes foreign enzyme called tryptophan hydroxylase (TPH), which is responsible for converting tryptophan (which you get from the protein that you eat) into serotonin .
Most people associate serotonin with being a neurotransmitter in the brain that regulates your mood. It’s important for feeling good. But actually it does so much more in the brain during brain development and also throughout the rest of the body.
What was really interesting about my research and what I had identified is that first, there are two different tryptophan hydroxylase genes in the body. We have one in the brain and we have one in the gut. The one in the brain makes serotonin in the brain, and the one in the gut converts tryptophan into serotonin in the gut. They’re completely opposite. The serotonin in the gut does not cr ossover to the blood-brain barrier and get into the brain. That’s different.
JM: I apologize for stopping you. But that is such an important point. It’s a point I didn’t really understand and I think most people watching this don’t understand. The reason this comes up is that typically we’re taught that 80 percent or the majority of the serotonin in your body is produced in your gut. You’re thinking it’s going to improve brain function but it doesn’t, because it doesn’t cross the blood-brain barrier. It’s such an essential point. I just want to emphasize that.
RP: Totally. Actually like 90 percent of the serotonin made in the body is in the gut , and it doesn’t cross the blood-brain barrier. It does serve a very important function. The serotonin made in the gut gets taken up by your platelets. Platelets can’t make their own serotonin , so they need to get it from the serotonin that’s made in the gut.
It plays a very important role in causing platelets to aggregate together , which is important when you injure yourself. If you cut yourself or if you bruise yourself, you want to have that coagulation. You want to have the platelets aggregate together to form a clot, so that you don’t bleed out, have a hemorrhage and bleed out. Serotonin plays an important role in making sure that platelets do that.
You need to make serotonin in your gut. But on the other hand, it’s a double -edged sword, because too much serotonin in the gut actually causes gut inflammation. The reason it does that is it also activates immune cells in your gut called T-cells. It causes them to proliferate. They can start firing away pro- inflammatory cytokines and things like that.
That’s actually been shown in mouse models of colitis or inflammatory bowel disease. You can genetically engineer mice to get colitis or inflammatory bowel disease, or you can give them environmental cues to cause gut inflammation. It’s been shown that if you stop those mice from producing serotonin in the gut, it completely takes away their gut inflammation. It resolves very robustly. Too much inflammation in the gut is not good.
[-— 10:00 -—]
What I found is that the tell-tell (T-cell?) sequence I was talking about that vitamin d recognizes in the gene, which is important in making that enzyme that converts tryptophan into serotonin in the gut actually turns it off in the gut. It turns it down. It’s like, “OK, you don’t need to make so much of the serotonin .” It kind of keeps it in check. It’s not going crazy making too much serotonin .
Whereas the tryptophan hydroxylase gene in the brain has a sequence that is completely opposite. It’s actually consistent with activation. vitamin d would then recognize the one in the brain and go, “Oh, turn it on. Make more serotonin in the brain.” Serotonin in the brain plays a very important role in the way you feel. It plays an important role in impulse control, long-term planning, long-term behavior, anxiety, and memory. It plays an important role in a lot of different cognitive functions and behaviors.
Actually, there have been a lot of very interesting studies that neuropsychologists, neurobehavioralists, and also neuroscientists have done in collaboration with each other where normal people are given a big shake full of branch-chained amino acids like leucine and isoleucine, which actually compete with tryptophan.
As I mentioned, you need tryptophan to make serotonin . But tryptophan has to get into your brain. It has to be transported into the brain. The transporter that allows tryptophan to get into the brain also allows other amino acids like leucine and isoleucine to get into the brain. But those other branch-chained amino acids get in better. They tend to outcompete tryptophan. When there are a lot of branch-chained amino acids around and not enough tryptophan, when the ratio is off, not a lot of tryptophan can get into the brain, which means you’re not able to make as much serotonin in the brain.
This has relevance for exercising, for example. When you’re lifting weights, you actually cause branch - chained amino acids to be taken up into your muscle cells to build muscle. That alleviates the competition and allows tryptophan to get into the brain. It’s part of the reason why, in addition to endorphins and many other things, exercise makes you feel so good, because you’re now allowing tryptophan to get into the brain , so you can make more serotonin . Anyway, I digressed.
JM: That’s interesting. There’s an interesting other component of that, too, which I just appreciated recently. It’s that when you are on a ketogenic diet, burning primarily fats as fuel, those ketones are very similar in structure to the branch-chained amino acids. The body seems to preferentially metabolize the ketones and the branch-chained amino acids. Those actually increase even though your intake didn’t increase at all, because they’re not degrading them and using them as fuel.
RP: Interesting.
JM: I didn’t understand the connection between the competitive inhibition into passing the blood-brain barrier. I guess that’s a potential complication. You could actually decrease brain levels of serotonin by increasing the branch-chained amino acids.
RP: Yes. If you don’t let the branch-chained amino acids go to other places like the muscle where they actually serve a really important role in muscle mass. But you can actually deplete people of their brain serotonin by giving them a big shake of amino acids, or essentially branch-chained amino acids, without tryptophan. You take away the tryptophan, and you just give them a bunch of leucine and isoleucine.
JM: Interesting.
RP: And because they outcompete tryptophan, within a few hours, about 90 percent of the brain serotonin levels drop .
JM: Wow.
RP: Right. This gives scientists an opportunity to study the behavioral effects, the causal behavioral effects, of lowering brain serotonin in people.
JM: That’s a standard intervention to produce serotonin deficiency?
RP: Yes.
JM: Wow.
RP: This is a standard intervention in research to induce brain serotonin deficiency in people - normal people, people with autism, and people with attention-deficit hyperactivity disorder (ADHD). It’s been done in a variety of different disease states as well as with people who have not been diagnosed with any sort of brain dysfunctional disorder.
What’s pretty ubiquitous is that people become very impulsive. They’re more likely to just kind of make a decision without thinking about it, without thinking of the long-term benefits, or kind of weighing the costs, the risks-benefits ratio. Their long-term thinking, their long-term planning kind of shuts down a little bit. They kind of just go with that impulse.
Mood is affected . People become a little more depressed. They become anxious. Memory is affected. Sensory gating, the ability to filter out all these stimuli our brain’s getting - auditory, visual... These things are coming in, and our brain can focus in on one thing, a conversation that we’re having, for example. That is affected when serotonin is low. Everything comes in and you sort of get this overload where you just don’t know what to do. Lots of different brain functions are affected by lowering brain serotonin levels.
JM: Depression being a primary one. I mean, the most common antidepressant is selective serotonin reuptake inhibitors (SSRIs).
RP: Exactly.
JM: It’s a question whether or not they really work that way, because of this whole placebo effect. But anyway, that’s at least their suspected mechanism.
RP: Yeah. The way they work is sort of understood, but there are so many different feedback effects, effects that aren’t understood, that we just don’t really know exactly what’s going on with SSRIs. There are a lot of negative feedback/effects as well. That’s a whole other topic. But yeah, depression is one of the major ones that’s known to be regulated by serotonin ** . I digressed a little bit, but I just want people to.
JM: It’s important.
RP: Know how important serotonin is in normal brain function. Again, vitamin d . What I found is that vitamin d is activating that gene that is making serotonin in the brain, and it’s kind of turning down the one in the gut, so you’re not making as much serotonin in the gut.
Since I published my first paper on this back in 2014, an independent group at the University of Arizona biochemically validated that indeed vitamin d does activate that gene, tryptophan hydroxylase 2 (TPH2), to make a lot more of it in a variety of different neuronal cell types, which was a really nice validation of my work from an independent group showing that indeed vitamin d does activate that gene in the brain to make serotonin .
JM: Just to emphasize: this was not known prior to you finding this out and publishing it. This is a new finding. Just major kudos and congratulations for that discovery, because it really is a significant advance in the understanding of this disease.
RP: I appreciate that. Yeah, it was not known. I did a lot of research that was theoretical in a sense that I wasn’t doing any experimental work. It was actually my first theoretical publication . Up until then I have been assigned doing experiments, publishing on things that I have been testing experimentally. This was the first time that I had just taken all this data that’s out in the literature and sort of put the pieces together like a puzzle. Things just started to fit together. Maybe I was wrong on some things that other scientists will find out, but I think that...
JM: That is one of your great characteristics and traits. There’s no question about it. It’s so clear to me that you. There are so few scientists who can look at the data, connect the dots, and make some really good predictions. It’s the rare researcher who can do this. You can do it on steroids. It’s just amazing how gifted you are doing this.
I’m just so excited to have a collaboration with you. You share this healthy viewpoint on life where you’re applying most of these interventions yourself and really trying to push the limits in things. It’s just a great combination of gifts to have to really help us understand and find the truth.
RP: Great complimentary. Thank you. And thanks for giving me a microphone to get the word out. I’m also very appreciative of that.
JM: All right.
RP: Let’s get back to autism, right?
JM: Yes.
RP: Can we get back to autism?
JM: Sure.
RP: OK. The other thing that serotonin is doing in the brain during early brain development, fetal brain development, is it actually (when you have a developing fetus, the brain’s developing) accesses what’s called a brain morphogen.
What that means is serotonin is required in a developing fetal brain in order to shape the structure and the wiring of the brain. It does this by telling neurons where to go in the brain and what type of neurons to become. If you don’t have serotonin there doing that, this leads to abnormal brain structure and abnormal brain wiring. In mouse models, it’s been shown to lead to sort of the mouse equivalent of autistic behaviors.
Serotonin is playing a very important role in brain development. What’s really interesting is that the developing fetus depends entirely on the mother’s levels of vitamin d . The maternal levels of vitamin d crossovers the placenta, gets into the blood-brain barrier, gets into the fetal brain, and activates all those fetal genes.
[-— 20:00 -—]
You can imagine that if a mother is deficient in vitamin d , this may have severe consequences in the developing fetal brain of her child, because maybe that gene that needs vitamin d to get activated is not getting activated. As a consequence, there’s not enough serotonin being made in that infant’s brain. It possibly could affect the way that brain develops.
This is sort of the connection I made between... As you mentioned, Dr. Mercola, earlier, vitamin d has been linked to autism by many different researchers, and low serotonin has been linked to autism by many different researchers. But no one has sort of put the two together as a mechanism going, “Look, maybe the low vitamin d leads to low serotonin in the developing brain. This may be part of the reason why there’s an increase in autism and maybe part of the way why low vitamin d leads to autism.”
I think there’s a very complex interaction between that and also genes. Variations in genes are called gene polymorphisms. Really, all you need to know about that is people have different variation of genes that lead to different functions. Many genes involved in the serotonin production and serotonin function also can be disrupted, and those have been shown to lead to autism. If you have someone who’s already susceptible genetically to low serotonin and on top of that have vitamin d deficiency, it’s like a double whammy.
I think that’s something that I’d like people to recognize. There’s an interesting interaction between our genes also and the nutrients, the way different nutrients are interacting with the way we’re making serotonin . That’s kind of one end.
I talk about many different things in this paper in terms of autism incidence. I think that’s one of the most compelling arguments. There’s also another one that has to do with the gut, if you want to talk about that.
JM: Sure. Let’s go into that.
RP: OK. The other way is that maternal autoimmunity has been linked to autism. Are you aware of this?
JM: No, I wasn’t.
RP: Mothers of autistic children are four times more likely to have autoantibodies against fetal brain proteins in their blood at any time. You shouldn’t have in your blood antibodies against brain proteins. That’s not normal. But mothers of autistic children are four times more likely to have this.
In addition to that, studies that have been done at UC Davis have shown experimentally that when you cause monkeys, pregnant monkeys, to have a very strong autoimmune response during pregnancy, this leads to abnormal brain development. Having an autoimmune response is not a good thing for anyone, and it’s strictly not a good thing for a pregnant mother.
For people that don’t really understand what that means, an autoimmune response means your immune system is so activated that it starts to recognize its own organs, its own tissue as something foreign, like a bacteria or a virus when no, it’s not foreign; this is your own organ, this is your own tissue. But your immune cells for a variety of different reasons can’t recognize that, so they start attacking it and damaging the tissue.
In the case of pregnancy, you have a fetus. There’s an embryo that starts developing and starts growing into this little developing fetus. Your body can recognize that as foreign. It’s like, “Whoa, what’s this? This isn’t supposed to be here. Attack. Attack. Attack. Get rid of it.” That can lead to a very severe autoimmune response.
But our bodies are wonderfully designed and we have a protective mechanism against that happening. We can make a type of immune cell called T regulatory cells (Tregs). T regulatory cells are very important because the more of them you have... These tell your body, “No, wait a minute. This is my body. This is supposed to be here. Quiet down, immune system. Don’t go crazy.”
Really, the T regulatory cells are a type of immune cells that play a very important role in keeping your immune system in check, making sure that your immune system knows what’s really foreign and what’s your own self. T regulatory cells are very important.
I mentioned earlier that there’s another enzyme that we have in our gut that converts tryptophan into serotonin . This is separate from the brain one. It turns out that females also have the same enzyme in the gut in the placenta. In the placenta, you can convert tryptophan into serotonin . You want to do this to some degree.
But tryptophan also gets metabolized by another pathway into something called kynurenine, which forms T regulatory cells, those important immune cells I just mentioned that are important for keeping your immune system in check, so it doesn’t go crazy. If you don’t let tryptophan form the kynurenine, the T regulatory cells will plummet.
This has been shown in animal models, in mice, for example. You take a mouse and you delete that enzyme genetically that produces kynurenine, which allows tryptophan to be converted into kynurenine and into the T regulatory cells. Pregnant female mice have such a strong autoimmune response that they actually end up aborting the fetus, because the immune system just attacks it.
Thus you want to make sure that not all the tryptophan is being converted into serotonin in the placenta. You also want it to be converted into this other pathway into T regulatory cells. It turns out that tryptophan actually binds three times tittered to the enzyme tryptophan hydroxylase, which is converting tryptophan into serotonin .
Back to vitamin d . If you don’t have enough vitamin d around, if you’re vitamin d deficient, you may be making way more of this enzyme that binds tryptophan and it may act like sink, a trap where tryptophan is being sucked into that pathway and producing serotonin in the placenta. The tryptophan doesn’t have a chance to be converted to that other pathway that forms kynurenine and T regulatory cells. This may have a negative effect, particularly during pregnancy, because you’re not making enough T regulatory cells, and therefore you start to have a heightened autoimmune response.
vitamin d ’s been connected to autoimmunity for a variety of different mechanisms. I think this is one potential additional mechanism that vitamin d may be regulating autoimmunity, because it may quiet down that other enzyme that binds to the tryptophan so tightly and may be acting as a trap for that tryptophan. It keeps getting sucked into it like a vacuum. Instead vitamin d turns that down a little bit. It quiets it. Now the tryptophan can be more balanced out. It can go this way into forming serotonin in the gut and in the placenta, and it can be going the other way to form the kynurenine and the T regulatory cells.
JM: Do you think this will play a role in other autoimmune diseases also? There’s no question in my clinical experience that it’s reprehensible clinical malpractice if you don’t optimize vitamin d levels in someone with an autoimmune disease. That is the first step you’ve got to do.
RP: Absolutely. I think it plays a huge role. We know that vitamin d undoubtedly... There is irrefutable evidence that it plays a huge role in preventing multiple sclerosis. That’s like. You just can’t deny that data. It’s just genetically from every angle. vitamin d levels - every angle you look at it, it comes out that vitamin d plays an important role.
JM: It’s a classic autoimmune disease.
RP: A classic autoimmune disease. Exactly. I know I went a little bit into the weeds on this one.
JM: No, it’s important to do it because not many people are discussing this, so I appreciate your insights.
RP: Yeah. It’s not being discussed. I think it’s important not only during pregnancy, but I think it’s important just during development, during adult life. It’s important. It’s a general mechanism that potentially is one other way vitamin d is regulating autoimmunity and preventing autoimmune responses by making sure you have enough of those Tregs.
JM: I haven’t heard of that before, so I appreciate the insights. I just wanted to confirm that it was true for other autoimmune diseases and it apparently is.
RP: Yeah. I think it is. There is going to be more and more experimental work definitively showing that. I think it’s one other potential way. You can expand it for other autoimmune diseases. It’s not just during pregnancy.
You mentioned it’s almost malpractice for a physician not to optimize someone’s vitamin d levels, particularly if you have an autoimmune disease. I think that there’s a simple solution for OB-GYN practitioners, normal family practitioners, or for any female that wants to get pregnant or is pregnant. I think there’s a simple solution and that is 1) get your vitamin d levels measured and 2) supplement. Make sure you’re getting enough vitamin d , high enough to make sure that you have optimal levels, so you’re not deficient.
[-— 30:00 -—]
I think that’s a simple solution to possibly preventing diseases like autism. This is relevant for other diseases as well - ADHD, schizophrenia, and a variety of different brain dysfunctions. As I mentioned, serotonin plays an important role for a variety of behaviors. I think that if you generalize, just for a lot of different brain functioning.
JM: Just to highlight and remind people what those levels are... Because I’ve sort of transitioned back and forth on that. But after reviewing this for nearly two decades, I’m fairly convinced of the data that the range is probably between 40 and 60 nanograms per ml. You don’t want to be under 40. That is for sure. The sweet spot might be 50.
Bruce Hollis did some really interesting work in pregnant women actually and found out that vitamin d sufficiency was right around that level. And 60 gives you a little threshold to go down. Because if you’r e relying on sunlight exposure, and obviously you’re not going to have access to sunlight continuously, you’ll have a reserve that you can fluctuate down and below that.
RP: Just to add on to that, I think the sweet spot for vitamin d is very important. Oftentimes when people find out that something is good for them, they have a tendency to just go overboard.
JM: The Goldilocks syndrome.
RP: Right. What’s it called?
JM: Goldilocks syndrome.
RP: Goldilocks syndrome, right. It’s very important, because too much vitamin d can be toxic. I think there is a sweet spot.
JM: Well, it has a very low level of toxicity. You’d really have to overdose in millions of units.
RP: Yeah, I don’t mean toxic in the acute sense.
JM: But less than optimal. You’re not going to hit the sweet spot. There’s no reason to go crazy with this.
RP: Right. I think that between 40 and 60 is a really good window, because studies have shown that people within that range. Meta-analyses have shown between 1960s and 2012 or something (there are lots and lots of studies aggregated together) have shown that blood levels of vitamin d within that range have the lowest all-cause mortality. Meaning, they die less of all non-accidental deaths like cancer, neurodegenerative disease, cardiovascular-related diseases, and respiratory diseases. There is something to be said for that.
Also people genetically who have low vitamin d levels are susceptible to higher all-cause mortality. That’s also something to consider. vitamin d does play a very important role in the aging process. I don’t know if you’ve seen any of these studies with mice.
JM: Telomere line?
RP: Telomere’s probably the mechanism, but there’s another study that was published. I love this study. It was published back in 2009 (I’ll send it to you) where researchers genetically engineered mice to not be able to respond to vitamin d . They altered their vitamin d receptors. Essentially these mice, it’s like being vitamin d deficient. Their cells can’t respond to vitamin d . It’s like there’s no vitamin d there.
These mice have a progeria phenotype. They have an accelerated aging phenotype. If you look at controlled mice that have normal levels of vitamin d throughout their life and you compare it to these mice that are genetically designed to be vitamin d deficient, out of four months of age, they look the same. They look similar. But then you look at them again around eight months of age, and the vitamin d - deficient mouse lost all of its hair, its skin is really wrinkled, its organs are starting to age rapidly. Its kidneys are shutting down. The liver’s not working. It just looks awful.
vitamin d is playing a very important role in the aging process. And as you mentioned, it does play an important role in telomere length.
JM: Yes.
RP: I’ m sure you’ve talked about telomere.
JM: And just to reinforce, too. The ideal way, the way that we were designed to get vitamin d is from being outside in adequate sunshine having enough skin exposed.
RP: Yes.
JM: Clearly in the winter, in the majority of the population in the U.S., this is not going to happen. It just isn’t. That’s one of the reasons why I moved to Florida, so I can get it natural. I haven’t swallowed an oral vitamin d in a long time, like years, many, many years.
RP: Wow.
JM: My level’s still within that sweet spot. But the question I have for you is really about these polymorphisms. If you can’t get it from sun exposure, you’re going to have to swallow a pill. But there’s a fairly significant portion of the population who even when they’re given 10,000, 20,000, 30,000 units a day still don’t get to levels within that. Is that because of these polymorphisms that essentially don’t allow the liver to hydroxylate the vitamin d ? Because that’s what we measure in the blood, the 25-hydroxy D.
RP: You nailed it. Yes, that’s exactly why. There is a very common gene polymorphism and a gene that burns enzyme called CYP2R1.
JM: OK.
RP: Which converts vitamin d 3 into 25-hydroxy vitamin d , which is the major circulating form of vitamin d . It’s what most physicians measure as a marker of a vitamin d status. This polymorphism in the gene, which just basically alters the sequence in the gene which alters the function of it, what it does is it alters it in a way that that enzyme doesn’t work as well. vitamin d 3 is not getting converted into 25 - hydroxy vitamin d very well.
As a consequence, people with this gene polymorphism, in some cases, have to take very, very high doses of vitamin d 3 orally to achieve normal levels of 25-hydroxy vitamin d , and levels that people like you and I would never take, because it could induce some negative effects. But you wouldn’t know that if you never got your vitamin d levels measured. I actually know some people in my close friend network that have this gene polymorphism, and they have to take very, very high levels of vitamin d .
JM: Physicians see this all the time if they are monitoring patients. There are loads of people in this population. I don’t know what the incidence is, but I suspect it’s over 5 percent. This is not a small percentage of people who have it.
RP: I agree with you. I don’t know what the incidence either. I’m trying to look into it to see how troubling it is, because that’s sort of important to know. In order for anything to be considered a gene polymorphism, it has to be over 1 percent of the population.
JM: OK. I didn’t know that was the definition.
RP: The difference between a mutation and a gene polymorphism, for people listening: a mutation is thought to occur randomly. When a mutation happens to your gene, it happens randomly. For whatever reason, your mitochondria metabolism isn’t working properly, and it’s dumping all sorts of toxic things that may possibly cause a mutation, that happens randomly in a population.
A gene polymorphism is thought to be because of a certain reason like it’s been selected for. The reason this has been thought is it occurs in at least 1 percent of the population, and in some cases, up to 50 percent of the population. There are always variations in different genes that are so common. There has to be a reason.
It’s largely thought, at least in the scientific community, that these gene polymorphisms occur based on nutrition, based on our environment, or where we live. We used to be hunter-gatherers. We lived in isolated regions.
If, for example, we’re going to live in a part of the world where the selenium in the soil is very, very high, as a population, we could have gotten a gene polymorphism in the gene that lowers our selenium absorption, because we don’t need as much. We’re getting it all the time. Our body’s like, as a response, “I don’t need as much selenium. I’m going to get too much of it.” It changes the sequence of DNA in such a way that the gene that controls that now isn’t doing as much. There are many examples of this.
JM: Let me give you a really good illustration of this. It’s a personal one. I have a gene polymorphism for one of the hemoglobin genes. It’s called thalassemia, Mediterranean anemia, which is similar to sickle cell. It produces a hemoglobin variant that makes the red blood cells really tiny and it produces an excess of them, its relative polycythemia.
The reason why this persists in a population is that... What is one of the most common causes of death in the world ever? Malaria. More people have died from malaria I think than any other cause. This polymorphism provides a relative protection to acquiring an infection or dying from it, which is interesting. That’s why it persists.
[-— 40:00 -—]
RP: Exactly. Great example, Dr. Mercola. I love it. It reminds me of another very, very common gene polymorphism called apolipoprotein E (APOE). It just forms APOE 1, 2, 3, and 4. I’m sure you’re familiar with this. APOE 4 is in 25 percent of the population. It’s very, very common. It has all these negative effects. It increases cardiovascular rates. It has a much higher incidence of Alzheimer’s. But what’s really interesting I found in the literature is that people with this APOE 4 allele or having this polymorphism are protected from malaria. Again, that’s a pretty important function.
JM: It’s such a common cause of death. If you want the population to persist in the environment, you’re going to have some type of relative protection against these common causes of death.
RP: Exactly. If you think about in the case of APOE 4, you’re talking about Alzheimer’s disease or cardiovascular diseases, these are age-related diseases. These occur much later in life. The body doesn’t care. The body cares about surviving right now, being able to live, so you can reproduce and pass on your genes. Malaria will take you out when you’re at any age. That’s something that is obviously very important to protect against. You can imagine that it’s going to stay within the population.
JM: All right. We’re going on a little tangent. I think it’s important to illust rate these points though. But getting back to vitamin d and going back to the original hypothesis, assuming with these gene polymorphisms that limit that percentage of the populations, which we don’t know what, but clearly over 1 percent, probably under 10 percent, where people need a lot of extra vitamin d .
I would imagine those same individuals if they were to get their primary exposure through sunlight, healthy doses of sunlight, that they could generate... Most people don’t realize and appreciate how much vitamin d you’ll get if you expose your skin to sunlight. You can easily get 10,000, 20,000, to 30,000 units with a relatively small amount of time exposure if you’re healthy and you’ve got your biological systems up.
My guess is that these individuals wouldn’t even necessarily notice it, because they’re sort of overdosing themselves through their feedback loops, regulating it, so it’s normal anyway. It bypasses that polymorphism. Would that be a fair assumption?
RP: I’ m not sure. Because you’re making vitamin d in your skin, the body, it’s very tightly regulated. You get to a certain level, there’s always mechanisms degrade precursors for D3 to something else, so that it doesn’t become D3 because your body doesn’t. Because it’s a fat-soluble vitamin, if you’re out in the sun, like we were when we were hunter-gatherer, we were out there all the time, vitamin d toxicity never really occurs from the sun because of that tight regulation where your body can sense what your levels are and go, “OK. I’ve got enough. I don’t need to keep making more of this.” So, I don’t really know.
JM: But won’t that feedback be altered if there was a polymorphism that influenced the hydroxylation?
RP: One would think it would, so you probably keep making it.
JM: The bottom line is that the body just self-regulates. It’s just a beautiful system. The more how we come to understand how it does it, the simpler the recommendations are, and the more effective they’d become.
RP: Yes. I agree. The body is beautifully designed. It knows best. It’s able to understand things that we’re just scratching the surface and getting to scratch the surface on understanding.
The case of getting it from the sun is obviously like many women that have melanin, for example, which protects them from the burning rays of the sun but also prevents their bodies from making vitamin d 3 as efficiently. Living in places like Chicago, living in northern latitudes where six months of the year, UVB rays aren’t even actually hitting the atmosphere.
I think that one has to consider many factors in terms of whether or not they’re going to supplement and in terms of whether or not they can even make it from the sun, depending on where they live, how dark their skin color is, their health status (if they’re obese or overweight), or what their age is. There are many different things.
If you are out there making vitamin d from the sun, get a blood test to make sure that you’re within that sweet spot range.
JM: Definitely.
RP: You should ask your physician to do it. You can even order it online. There’s a variety of tests that are available.
JM: Sure. Thank you so much for your work, for your investigations, and for providing such an articulate and elegant description of what’s likely occurring. It has actually been proven scientifically since your original paper.
So, let’s put it all together, because you’re so good at tying the dots. The message that we want to share with them is an important one: an ounce of prevention is worth tons of a cure. Many times you can’t even get a cure, because it’s just not possible because you have irreversible damage. The key message here is before you even think about getting pregnant, certainly if you are, or if you know anyone who is, you’ve got to get their vitamin d tested. It just has to be done. There’s no way around it.
We went over that pretty clearly. But the second one, which we didn’t discuss in detail, is that in your paper, you suggested that it’s probably wise to consider a tryptophan supplement additionally.
RP: A tryptophan supplement could help more with the treatment in autism.
JM: The recommendation wasn’t a preventive approach?
RP: Not with tryptophan.
JM: OK. I misread the paper. I’m sorry.
RP: That’s OK. It’s so complex. It’s a very long paper. I go into prevention versus treatment, because prevention is key, like you mentioned. But I think getting that and making sure you have that vitamin d is very, very important for making sure that the developing brain is getting enough of it since it’s relying on its mother’s levels of vitamin d to activate the serotonin in the developing brain.
JM: OK. Well, it’s been known for a while, as we said in the beginning, that vitamin d is useful to lower the incidence of this, but we didn’t know why until you uncovered it. Thank you so much for that really brilliant research and for helping us understand the details, because the devil is in the details. If you can understand the mechanism, then you can begin to better appreciate, and have a finer recommendation and better revision of what the strategy is to prevent these diseases.
RP: Absolutely. Thanks again, Dr. Mercola, for having me on your show and letting me discuss my recent research.
JM: We definitely look forward to it. And you have your own show at FoundMyFitness.com. It is one that I review regularly, because you interview some of the top scientists in the world. You really are a very gifted researcher.
Your brain works so well that you can connect all these dots together, because most people can’t connect the dots. They’re just experts in their little specific field. They just can’t think out of the box to how this connects to anything else. Someone has to do that. In medicine, it’s the job of the famil y physician to really sort of have this comprehensive view and help people apply that knowledge from all these different subspecialists. You do that in the biological science field. I appreciate that.
Your interviews are a joy to watch. It’s free to subscribe. FoundMyFitness.com. We have put some and we’ll be putting more of your interviews up as you do them. Thank you for that.
RP: Thank you very much. Can I plug anything?
JM: Sure. Absolutely.
RP: OK. In addition to doing interviews, I also have a health newsletter where I write articles. I also make videos where I sort of put together connect the dots and transfer information to people, so they can understand to the best of their ability the best lifestyle strategies to help them age the best way they can.
JM: That’s sort of what I was seeking to communicate when I mentioned it earlier. You do these interviews but you have these other videos that you produce. The beautiful thing about your videos, which you can tell, if you’ve watched this video up until now, that you’re able to translate very complex technical issues into simple language that people can understand. That is a rare gift.
I think I do that somewhat well on my site for medical things, but you do it really well for the biological sciences. That’s why I’m so really fond of your work. So, definitely, if you have the time, I would strongly recommend and encourage you to subscribe to her newsletter. They’re just a joy to watch.
RP: Thank you, Dr. Mercola.
JM: All right. We’ll definitely continue to highlight some of the research and the work that you’re uncovering. Thanks for all that you’re doing.
[END]