Upsurge in Metabolic diseases may be due to low vitamin D
Vitamin D Deficiency - A Missing Link in The Upsurge of Metabolic Diseases??
INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH Volume : 5 | Issue : 5 | May 2016
M.Sc, PhD Biochemistry; Associate Professor, Department of Biochemistry, Vivekananda Institute of Medical Sciences, Rama Krishna Mission Seva Pratishhan, Kolkata, India * Corresponding Author
📄 Download the PDF from VitaminDWiki
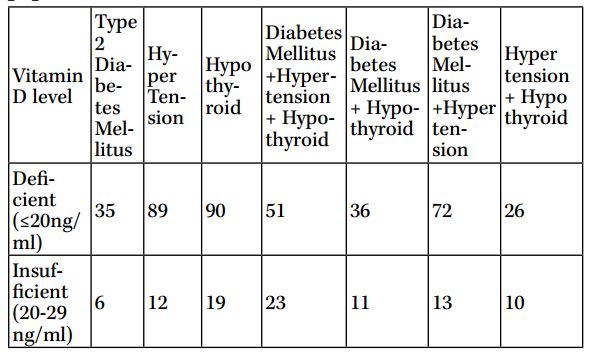
Co-occurances of Metabolic Syndrome Diseases (Table 1)
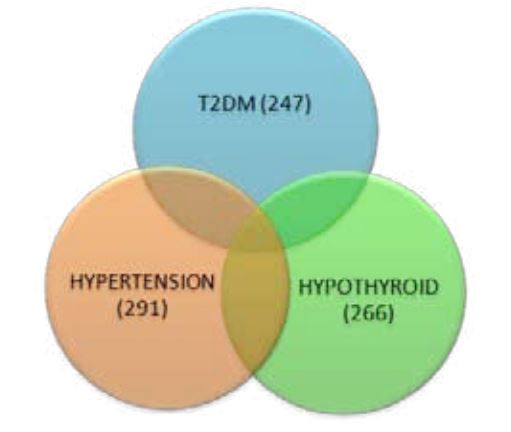
Venn diagram: Overlap of Metabolic Syndromes if have low vitamin D (Figure 5)
Introduction: Vitamin D deficiency (VDD) is a global health problem. Emerging evidences show an involvement of VDD in to a broad spectrum of non skeletal diseases in recent years. It has been identified as a risk factor for Type 2 Diabetes Mellitus (T2DM), Hypothyroid and Hypertension (HTN). Role of vitamin D in insulin resistance, regulation and maintenance of hormones of the HPT axis and the suppression of the RAS pathway have recently been elucidated. Thus VDD is supposed to be a key player in the pathogenesis of these metabolic diseases.
Objective: To study a retrospective analysis on the prevalence of T2DM, Hypothyroid and HTN among the vitamin D deficient group in a large cohort of 2044 patients attending OPD of RKMSP, West Bengal.
Method- All biochemical parameters were tested in the department of Biochemistry, RKMSP and data collected from hospital medical records.
Results: 82.2% Vitamin D deficiency was observed. Prevalence of T2DM, Hypothyroid and HTN were found to be 14.6%, 15.8% and 17.3% either individually or in combination.
Conclusion: T2DM, Hypothyroid and HTN were significantly prevalent in the VDD population.
Introduction :
Vitamin D, the major medical breakthrough of the last decade, has been linked to a cascade of diseases caused due to its deficiency (VDD) (Van Schoor N M and Lips P,2011) apart from its role in bone mineral homeostasis. VDD has become a silent epidemic worldwide and affects around 80% of the world population irrespective of geographical location and seasonal variation. Lack of exposure to sunlight, use of sunscreen, sedentary lifestyle - physical inactivity, obesity, poor nutrition contribute significantly in the progression of VDD. India being a tropical country receives ample sunlight but VDD is prevalent in a large scale (Ritu G et.al, 2014) The predisposing effect of VDD on Type 2 Diabetes Mellitus (T2DM), Hypothyroid and Hypertension (HTN) has been cited in many literatures. The sharp rise of diseases with VDD points towards a greater interplay which is yet to be deciphered.
Vitamin D and Type 2 Diabetes Mellitus
Among metabolic disorders type 2 diabetes mellitus (T2DM) is a pandemic worldwide and WHO has predicted that by 2030 the number of diabetes patients will become twice the current figure of 170 million (World Health Organisation-The Diabetes Program 2004).VDD and T2DM are highly prevalent in the elderly population worldwide and is currently a topic of immense importance among all ages, races, socio-economic strata and geographical regions (Griz M et. al , 2004). Since 1980, there have been studies on mouse models trying to establish a correlation between VDD and T2DM. The identification of 1,25(OH)2D receptors and 1-a-hydroxylase expression in pancreatic beta cells, indicates the role of vitamin D in the pathogenesis of T2DM. Vitamin D deficiency leads to glucose intolerance and ultimately causes type 2 diabetes mellitus.
Increased insulin resistance, increased hepatic glucose production and p-cell failure are the key factors in T2DM. It is suggested that vitamin D modulates insulin receptor gene expression with the help of vitamin D responsive elements (VDRE) identified on the promoter region of insulin receptor gene. It works by increasing insulin sensitivity and expression of insulin receptor gene expression. Thus in deficient levels vitamin D acts as an environmental candidate contributing in the pathogenesis of T2DM (Ortleep JR, 2003)
On the other hand, it is also suggested that vitamin D plays a role in insulin resistance by the renin-angiotensin-aldosterone system. Glucose uptake is decreased when there is increased insulin resistance due to the inhibition in the action of insulin in vascular tissue and skeletal muscle. Angiotensisn II, a major contributor in the inhibition pathway is synthesized when VDD occurs and the RAS pathway gets activated.
Fig 1: Schematic representation of Vitamin D deficiency causing Type 2 Diabetes Mellitus
Vitamin D and Hypothyroid
Early stage of hypothyroidism when serum TSH increases but thyroid hormones remain normal is known as subclinical hypothyroidism. Thyrocytes are known to be influenced by vitamin D. It stimulates iodide uptake and growth by atteneuating TSH directly. The effect of T3, T4, and TSH on renal metabolism of vitamin D has been proved by mouse model studies (Sowers JR, 2004; Jonklaas J, 2013). Thus when VDD occurs, TSH levels rises as it does not get enough vitamin D to metabolize, or when TSH level rises vitamin D gets metabolized in large amount causing VDD. It is not yet clear which one predisposes the other, but the inverse relationship is clear. Mackaway et,al. showed the inverse relationship between serum vitamin D and TSH (the hormonal marker of hypothyroidism) (Kivity S, 2011)
Chronic autoimmune thyroiditis is also one of the contributors in the increase of Hypothyroid cases. It is characterized by subclinical serum TSH level (>4.52 - <10.0) with positive anti TPO antibody with or without the presence of goiter. Halder et. al., 2016 showed a significant negative correlation between serum Vitamin D levels and anti- TPO and TSH levels in a study conducted on 132 patients from West Bengal. The triggers of autoimmune thyroiditis may be genetic or environmental. The vitamin D receptor gene polymorphism causes VDD which leads to the infiltration of T and B cells into the thyroid gland. This causes the production of auto antibodies and upsurge in cytokine release. These cumulatively manifests in apoptosis of thyrocytes finally causing autoimmune thyroiditis.
Fig 2 : Schematic representation of HPT axis - any deregulation of hormones secreted by HPT causes Hypothyroid
Vitamin D and Hypertension
An intricate association is observed between vitamin D deficiency and high blood pressure levels and it is believed to predispose HTN (Kivity S, 2011; Halder T, et al, 2016; Tietz NW, 1995; Baynes KC, et al,1997; Scragg R et al, 1995; Chiu C et al, 2004). In vitro studies revealed the function of 1,25(OH)D as a negative endocrine regulator of renin - angiotensin system.[14] Studies suggest that vitamin D acts as a renin suppressor (Harburg E et al, 1978) and decreases angiotensin II sensibility (Hidayat R, et al, 2010) of the renin angiotensin system. The detrimental overproduction of renin is counterbalanced by vitamin D which functions as a gatekeeper in cAMP signal transduction pathway (Brown AJ, et al, 2002).When VDD occurs, there is no control on the production of renin in the juxtaglomerular cells. This also increases angiotensin II and the RAS pathway becomes activated which in due course causes hypertension. This mechanism has been proved by Li et al in genetically engineered VDR knockout mice. There was an increase in BP due to the activation of RAS pathway (Harburg E, et al, 1978)
Fig 3 : Schematic representation of Vitamin D deficiency causing Hypertension through the activation of RAS pathway
Coexistence of VDD, T2DM, Hypothyroid, Hypertension
It has already been stated that VDD is intriguingly related to T2DM, hypothyroid and HTN. Vitamin D and its analogs act as a negative endocrine regulator by inhibiting renin activity of the renin - angotensin system (Li YC,et al, 2002; Qiao G, et al, 2005)This renin-angitensin system is intricately involved in the pathogenesis of T2DM, hypothyroid and HTN - thereby establishing VDD as one of the markers for all these diseases. Again the polymorphism of vitamin D receptor modulates cytokines and immune cells to cause hypothyroidism, insulin resistance manifesting to T2DM and oxidative stress leading to HTN (Bur- gaz A, et al 2011). It has always been widely said and accepted that T2DM and hypothyroid predispose each other but the real reason behind it was never clinically established. May be it is time to unravel the mystery behind this. These three diseases have been most frequently seen to coexist in elderly population along with VDD. So vitamin D deficiency might be attributed to the causation of all diseases. Though there is a dearth of work in this area on Indian population. Association of VDD and HTN is relatively a much recent research topic in India. There is no published work on the Eastern Indian population more specifically on West Bengal population to the best of our knowledge relating these three metabolic and lifestyle diseases to vitamin D deficiency (Zhang H et al, 2000)
Aim :
The aims of the retrospective study were :
To analyse the prevalence of Vitamin D deficiency among the patient attending Ramakrishna Mission Seva Pratishthan.
To study the prevalence of T2DM, Hypothyroid and HTN either individually or in combination in the Vitamin D deficient group of people.
Study design and population :
All patients who had their serum 25(OH)D checked from Jan 2014 to May 2015 were included in the study. Data regarding clinical and laboratory characteristics were also collected from hospital records. Patients on Vitamin D supplementation were excluded from the study. This study was ethically approved by the Institutional Ethics Committee of RKMSP.
Biochemical Analysis:
Total 25(OH) vitamin D were measured by Cobas e-600 Immuno assay autoanalyzer and other biochemical tests were carried out in Vitrous 5,1FS (Orthochemical diagnostics) autoanalyser in Department of Biochemistry, RKMSP. The guidelines of The Endocrine Society, USA were followed to define Vitamin D deficiency (The Endocrine Society. Endocrine Society Guidelines 2011)
Results :
Vitamin D deficiency was observed in 82.2% (1682/2044) of the study population which includes 71.5% (1203/1682) vitamin D deficiency (serum Vitamin D level <20ng/ml) and 28.4% (479/1682) vitamin D insufficiency (serum Vitamin D level 20 -<30 ng/ml).
Fig 4 : Stacked Venn diagram representing the levels of Vitamin D deficiency in the total population studiedFig 5: Venn diagram showing the coexistence of Type 2 Diabetes Mellitus, Hypothyroid and Hypertension in Vitamin D deficient population
A comparative study of Diabetic, Hypothyroid and Hypertensive patients was carried out with their respective control subjects in the Vitamin D deficient population (Table 2,3,4) .
Discussion :
From the study it is clearly indicated that females are at higher risk to T2DM, hypothyroid and hypertension as compared to their male counterparts. Though these diseases are noted mainly in elderly population but the younger generation are also at high risk to the metabolic syndrome and lifestyle disorders due to stress and sedentary life style. Role of vitamin D deficiency in the causation of these diseases has been emphasized in many recent studies (Li YC,et al, 2002) which is in accordance with the results found in our study.
In the comparative study of the different groups in the vitamin D deficient population, serum 25(OH)vitamin D levels were found to be much lower in diabetic, hypothyroid and hypertensive patients as compared to their non DM, non hypothyroid and non hypertensive counterparts (Table 2,3&4). Vitamin D deficient Bangladeshi immigrants living in London was more likely to have T2DM compared to their vitamin D sufficient counterparts (Boucher, et al, 1995). It was demonstrated that insulin sensitivity was improved by 60% when vitamin D supplements were used (Pittas AG, et al, 2007; Aljabri KS et al, 2010). Scragg et. al in 2004 stated that T2DM risk decreased as serum 25(OH)D concentration increased in white, black and Mexican Americans. Pancreatic insulin secretion was inhibited by VDD which induces glucose intolerance (Cade C, et al, 1986).
The association between VDD and hypothyroid have long been studied worldwide (Jonklaas J,et al, 2013; Kivity S, et al 2011) with conflicting results. A negative correlation of VDD and anti- TPO was reported by Goswami et. al, in New Delhi, India which is in accordance with the study conducted by our group (Halder T et al, 2016). Also there exists a complex interplay between TSH and Vitamin D, as one increases, the other one decreases. Thus VDD has a key role in the pathogenesis of hypothyroid including autoimmunity.
Though HTN is a primary risk factor of cardiovascular disease it is often ignored and its relation with VDD have not yet been fully understood. An inverse correlation between ultra violet radiation and blood pressure have been indicated by clinical stud- ies.[29] A surrogate marker of vitamin D synthesis - ultra violet B radiation lowers blood pressure but no prospective study has been conducted so far to validate the facts. Inverse correlation between VDD and HTN was illustrated in numerous publications globally (Borissova AM, et al, 2003; Ruan H, et al, 2003;
Marcherri P et al,2006)
The observations of our study are compatible with the previous results published in eminent scientific journals worldwide which clearly indicates that vitamin D deficiency predisposes to type 2 diabetes mellitus, hypothyroid and hypertension.
Conclusion :
Lots of evidences from studies conducted worldwide since 1980 on mouse models and human point towards VDD causing glucose intolerance and predisposing t2dm, inflation of cytokines and auto antibodies causing hypothyroidism and oxidative stress causing hypertension. But there is no published work yet which would assimilate the scattered data related to all the three diseases and reach a common end point in West Bengal, Eastern India. Our study gives a comprehensive report on the prevalence of T2DM, HTN and hypothyroid in a large number of 1682 (82.2%) vitamin D deficient people of West Bengal. An already existing fact has been validated by our study on a larger vitamin D deficient population of West Bengal. Although the effect of vitamin D supplementations on these subjects has not been followed up in this study, which can be considered as one of the limitations of the study. It can be suggested that screening of vitamin D deficiency should be initiated at different levels to prevent the adverse outcome of the diseases.
References in PDF