Rickets and vitamin D overview – Lancet 2003
Rickets seminar The Lancet, Volume 362, Issue 9393, 25 October 2003, Pages 1389–1400
Prof Brian Wharton, FRCPCH a, bwharton@ich.ucl.ac.uk
Prof Nick Bishop, FRCPCH b
a MRC Childhood Nutrition Research Centre, Institute of Child Health, London WC1N 1EH, UK
b Academic Unit of Child Health, Sheffield Children's Hospital, University of Sheffield, Sheffield
Rickets, once thought vanquished, is reappearing. In some less developed countries it hardly went away. This seminar reviews the effects of genes, stage of development, and environment on clinical expression of the disease. Rickets can be secondary to disorders of the gut, pancreas, liver, kidney, or metabolism; however, it is mostly due to nutrient deficiency and we concentrate on this form. Although calcium deficiency contributes in communities where little cows' milk is consumed, deficiency of vitamin D is the main cause .
There are three major problems:
the promotion of exclusive breastfeeding for long periods without vitamin D supplementation, particularly for babies whose mothers are vitamin D deficient;
reduced opportunities for production of the vitamin in the skin because of female modesty
- and fear of skin cancer; and the
- high prevalence of rickets in immigrant groups in more temperate regions.
A safety net of extra dietary vitamin D should be re-emphasised, not only for children but also for pregnant women.
The reason why many immigrant children in temperate zones have vitamin D deficiency is unclear.
We speculate that in addition to differences in genetic factors, sun exposure, and skin pigmentation, iron deficiency may affect vitamin D handling in the skin or gut or its intermediary metabolism.
Figure 1. Radiograph of wrist showing rickets Classic features of rickets include cupping, fraying, and splaying of the metaphysis. The ulna (which grows more quickly at its distal end) is more severely affected. Widening of the growth plates is not shown because the secondary ossification centres of the radius and ulna are not yet apparent.
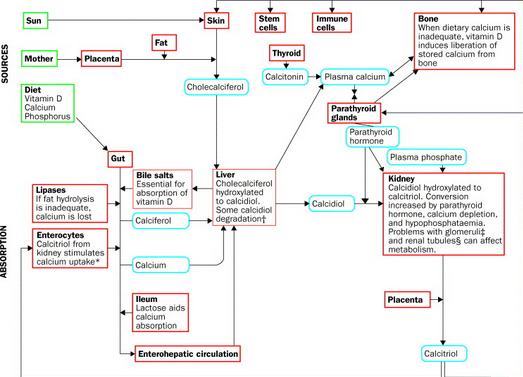
Figure 2. Nutritional handling of calcium, phosphorus, and vitamin D, and the causes of rickets*Enterocyte abnormality (eg, coeliac disease) can inhibit vitamin D and calcium absorption; transport out of the cell is reduced if carrier proteins are inadequate (eg, abetalipoproteinaemia or hypobetalipoproteinaemia34). †Degradation of calcidiol is increased by certain anticonvulsants and in hyperparathroidism (primary or secondary to limited amounts of absorbed calcium35) via the action of calcitriol. Hepatic/bile-duct disease limits bile-acid secretion.36 ‡Any cause of glomerular failure leads to retention of phosphorus with reciprocal hypocalcaemia and secondary hyperparathyroidism.37 §Tubular disorders can lead to excessive phosphaturia.38 Substances produced by some tumours induce phosphaturia leading to rickets before the tumour is clinically obvious.
Figure 3. Developmental changes in boys (conception to 18 years) relevant to mineralised tissuesNote that age scale is not continuous. For teeth development: G=tooth germ fully formed; D=dentine formation begins; C=crown formation complete; E=eruption. Abstracted from various sources: weight velocity,51 skeletal maturity,52 body calcium accretion,53 and 54 calcium concentration in femur,55 tooth development.56
Figure 4. Dietary reference values (DRV), observed intakes, and food contributions to these intakes of vitamin D and calcium in older infants, toddlers, and pubertal boys in the UKDRV=dietary reference values from UK Department of Health report 1991.123 LRNI=lower reference nutrient intake (values below this are almost certainly inadequate for most individuals). EAR=estimated average requirement. RNI=reference nutrient intake (intakes above this amount will almost certainly be adequate for almost all individuals). NS=not stated. White segments indicate all other sources. *Over age 3 years RNI in the UK for vitamin D is stated as O for “a normal lifestyle”; if “confined indoors” the reference nutrient intake is 10 μg. †Observed intakes, median (3rd–97th centile), abstracted from various UK government reports on representative national samples of the population.124, 125 and 126
Rickets diagnosis chart from unknown publication
See also VitaminDWiki
Rickets in 30 percent of infants in India who had low vitamin D – March 2011
Vitamin D, Cod-Liver Oil, Sunlight, and Rickets: A Historical Perspective – 2003
Osteopenia in preterm infants – May 2012 = Rickets Lite?
Black Sudanese children 350X more likely to have rickets than other Australians – April 2012
Turkey gave 400 IU vitamin D to all infants and reduced Rickets by 60X - 2011
Group is giving only 200 IU of Vitamin D to 70 million women and children to prevent Rickets
Rickets in England – huge recent increase – Feb 2014 also Lancet