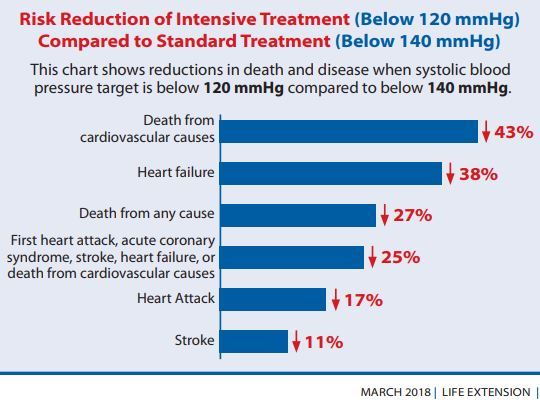
Off Topic – Hypertension in 42 percent of adults (new definition: 130 mm Hg)
Redefining Hypertension — Assessing the New Blood-Pressure Guidelines
George Bakris, M.D., and Matthew Sorrentino, M.D.
N Engl J Med 2018; 378:497-499, DOI: 10.1056/NEJMp1716193
Like physical guidelines designed to ensure that hikers stay on the safest path through tricky terrain, expert medical guidelines aim to steer clinicians toward best practices. The new Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults issued by the American College of Cardiology (ACC) and the American Heart Association (AHA)1 tries to accomplish this task by extending the Seventh Report of the Joint National Committee (JNC7) and the Expert Panel Report to include updated data from clinical trials and by accentuating previously underemphasized sections of the 2003 and 2013 reports.2
Since 2013, two studies have compared an approach to care that includes self-measured blood pressure (SMBP) with usual care. The ACC/AHA Task Force on Practice Guidelines recognized the need for an independent committee review of SMBP to inform recommendations about its potential use in evaluation and management of hypertension.1 The committee conducted a meta-analysis to assess whether SMBP without other augmentation is superior to office-measured blood pressure either for achieving blood-pressure control or for preventing adverse clinical outcomes.1
The new guideline quickly generated intense discussion and controversy. Though it addresses various topics, it focuses particularly on proper blood-pressure measurement and encourages home blood-pressure monitoring and initial combination medications for lowering blood pressure.
It makes clear that failure to
position patients and their arms appropriately,
utilize the proper cuff size, or
allow time to rest before performing three blood-pressure readings
can result in falsely elevated readings. In addition, proper instruction of patients in measuring their blood pressure at home is critical, as is annual validation of their machines. And use of initial single-pill combination medications for patients with blood pressures either 20 mm Hg above the systolic target or 10 mm Hg above the diastolic target is strongly supported. Renin–angiotensin blockers with either diuretics or calcium antagonists are preferred initial combinations.1
Unlike previous guidelines, the 2017 guideline emphasizes individualized cardiovascular risk assessment and aggressive management of blood pressure at levels of 140/90 mm Hg or higher in patients with a 10-year risk of cardiovascular events of more than 10%. Patients with blood pressures of 130 to 139/80 to 89 mm Hg would still receive nonpharmacologic treatment, unless they had a 10-year risk above 10%; in that case, a single antihypertensive agent is recommended, in concert with lifestyle changes.
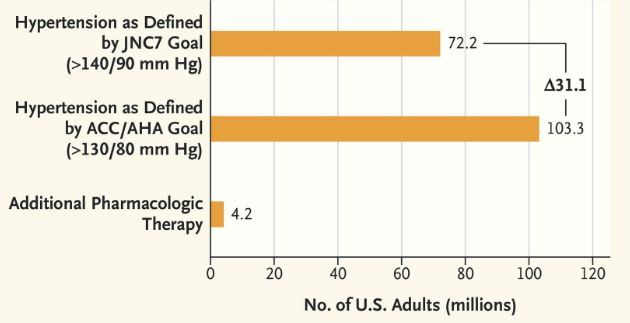
The area of greatest controversy involves the new blood-pressure categories, especially the lowered threshold for hypertension, which would greatly expand the number of Americans with this diagnosis (see graph).3 The guideline defines normal blood pressure as below 120/80 mm Hg and elevated blood pressure as 120 to 129 mm Hg systolic with a diastolic pressure below 80 mm Hg. Stage 1 hypertension is defined as 130 to 139 mm Hg systolic or 80 to 89 mm Hg diastolic, and stage 2 hypertension as 140/90 mm Hg or higher (the old definition of hypertension).
What is now called stage 1 hypertension was previously labeled “prehypertension” — a term meant to alert patients and to prompt physicians to provide lifestyle education to help delay development of hypertension. The term’s original intent was to reduce therapeutic inertia but, paradoxically, less care was delivered.
By reclassifying people formerly considered to have prehypertension as having hypertension, the guideline creates a new level of disease affecting people previously deemed healthy . According to this definition, about 46% of U.S. adults have hypertension, as compared with about 32% under the previous definition . It is hoped that reliance on the new definition of stage 1 hypertension, coupled with the focus on cardiovascular risk reduction as assessed with the atherosclerotic cardiovascular disease risk calculator, will result in earlier intervention and ultimately lower cardiovascular event rates. Note, however, that lifestyle modification is still the initial treatment recommended for people with stage 1 hypertension and 10-year cardiovascular risk below 10%.1
Although there are positive aspects of targeting higher-risk people with lower blood pressure for risk-factor modification, there is concern that a new disease designation can become a mandate for pharmacologic treatment without consideration of the patient’s risk level.
While emphasizing lifestyle modification for lower-risk people, the guideline recommends daily sodium intake of less than 1500 mg — a goal that’s difficult for many people to achieve and that was derived from short-term studies in which diets were controlled but minimal outcome data were collected. Though reducing sodium intake is desirable for people with hypertension, the data supporting daily intake of 2300 to 2400 mg are very robust, and further reduction has minimal additional effect on blood pressure.
Another concern is the 10% 10-year-risk designation, which is not based on randomized, controlled trials; moreover, the blood-pressure goal of less than 130/80 mm Hg is higher than that used in the Systolic Blood Pressure Intervention Trial (SPRINT). SPRINT was a study of blood-pressure lowering for primary prevention in high-risk patients, who were randomly assigned to a target systolic blood pressure of either less than 120 mm Hg or less than 140 mm Hg. High-risk patients were defined as having a 10-year risk of cardiovascular events of 15% or higher as indicated by their Framingham risk score. A more evidence-based approach to guideline development would have been to use the risk levels delineated by clinical trials. In contrast, given that systolic blood pressure is 10 to 15 mm Hg higher in practice than in SPRINT, it was prudent to select 130/80 mm Hg rather than 120/80 mm Hg as the target.
The guideline authors note that calculation of absolute risk as a guide to prescribing pharmacologic therapy has yielded mixed results. With a universal recommended blood-pressure goal, decision making regarding therapy can be simplified. Although we appreciate this concept, a one-size-fits-all blood-pressure goal is problematic.
Although the new guideline lowers the blood-pressure goal for people over 65, it suggests that 30-year-olds and 80-year-olds should have the same goal. Achieving that goal is impossible for many people, especially those with poor vascular compliance (i.e., pulse pressures above 80 to 90 mm Hg), who typically have dizziness and poor mentation as their systolic blood pressure approaches 140 mm Hg. In addition, the new guideline does not consider isolated systolic hypertension, which is a major problem among many people over 70. And it focuses only on the systolic-blood-pressure goal of less than 130 mm Hg, ignoring diastolic pressure and its management. It is reasonable to omit guidance regarding lower diastolic blood pressure, especially in people with diabetes, and to simply recommend use of clinical judgment. However, data from multiple studies both in patients with diabetes and those with documented coronary disease link diastolic blood pressures below 60 mm Hg to higher risk of ischemic heart disease and progressive kidney disease.4
The primary change in recommendations regarding pharmacologic therapy is the elimination of beta-blockers from first-line therapy for patients with primary hypertension and no coexisting conditions that require beta-blocker therapy. Though hypertension-outcome trials using beta-blockers have not shown a mortality benefit, the agent chosen, atenolol, requires twice-daily dosing, and these trials used only once-daily dosing. Some (generally younger) patients are more hyperadrenergic than others, as manifested in high heart rates, and may have an excellent blood-pressure response with appropriately used beta-blockers.
An individualized approach to hypertension can help determine the best choice for first-line therapy. For example, patients with volume expansion may be best treated initially with a long-acting thiazide-like diuretic; patients who are obese or have metabolic syndrome or diabetes, with a renin–angiotensin blocker or calcium antagonist; and those who are hyperadrenergic, with a heart-rate–limiting calcium antagonist such as diltiazem or a beta-blocker. Though a detailed discussion of individualized therapy may be beyond the scope of general guidelines, it’s possible to consider general patient profiles in recommending more efficient ways to lower blood pressure.5
Ultimately, although the guidelines expand on JNC7 in useful ways, it is problematic to shift the threshold for hypertension to 130/80 mm Hg. Some people with blood pressures of 130 to 139/80 to 89 mm Hg who are at higher cardiovascular risk may benefit from earlier intervention, but though such a broad-brush approach may be fine from a public health perspective, it could overburden our primary care physician workforce. Proper blood-pressure measurement is critical but time consuming. The unintended consequence may be that many people, now labeled as patients with hypertension, receive pharmacologic therapy that’s unlikely to provide benefit given their low absolute risk, and they may therefore experience unnecessary adverse events.
Finally, absolute risk is an important determinant of the need for treatment. It’s reasonable to consider more aggressive treatment goals in the highest-risk patients, as SPRINT showed. But while a blood-pressure treatment target of less than 130/80 mm Hg makes sense for high-risk patients, for everyone else it seems more reasonable to continue defining hypertension as a blood pressure of 140/90 mm Hg or higher.
Authors
From the Department of Medicine, ASH Comprehensive Hypertension Center (G.B.), the Section of Endocrinology, Diabetes, and Metabolism (G.B.), and the Section of Cardiology (M.S.), University of Chicago Medicine, Chicago.
Audio Interview: Interview with Dr. George Bakris on new blood-pressure guidelines from the American College of Cardiology and the American Heart Association.
References
Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCN A guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2017 November 13 (Epub ahead of print).
Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003;42:1206-1252.
Muntner P, Carey RM, Gidding S, et al. Potential US population impact of the 2017 ACC/AHA high blood pressure guideline. Circulation 2018;137:109-118.
. de Boer IH, Bangalore S, Benetos A, et al. Diabetes and hypertension: a position statement by the American Diabetes Association. Diabetes Care 2017;40:1273-1284.
Sorrentino MJ, Bakris GL. Approach to difficult to manage primary hypertension. In: Bakris GL, Sorrentino MJ, eds. Hypertension: a companion to Braunwald’s heart disease. 3rd ed. Philadelphia: Elsevier, 2018:281-8.