Sarcoidosis (rare) problems when taking vitamin D - many studies
Summary: 1 in 100,000 people have Sarcoidosis AND problems with Vitamin D & Calcium
Should perhaps reduce Calcium intake or increase Vitamin K
People with Sarcoidosis (1 in 10,000) should perhaps not take 4,000 IU of Vitamin D for a year – Oct 2022
Hypercalcemia worsened after vitamin D supplementation in a sarcoidosis patient: A case report
Medicine (Baltimore). 2022 Oct 7;101(40):e30883. doi: 10.1097/MD.0000000000030883.
Kimito Mio 1 , Kotaro Haruhara, Akihiro Shimizu, Kentaro Oshiro, Rena Kawai, Masato Ikeda, Takashi Yokoo
Rationale: There are many causes of hypercalcemia, with hyperparathyroidism and malignancy accounting for 90% of cases. Sarcoidosis and the intake of vitamin D supplements may also cause hypercalcemia, although the occurrence rate is low if only one is involved. We herein report a sarcoidosis patient who developed hypercalcemia after taking cholecalciferol (vitamin D supplement) for a year.
Patient concern: A 62-year-old Japanese man presented with hypercalcemia and acute kidney injury along with symptoms of fatigue and appetite loss while being followed up for sarcoidosis.
Diagnoses: We determined that a combination of cholecalciferol supplementation and sarcoidosis had led to hypercalcemia for several reasons. First, hypercalcemia had not been noted when this patient had first been admitted due to sarcoidosis-related respiratory failure several years earlier, which we presumed that was the highest sarcoidosis disease activity. Second, low serum 25-OH Vit.D3 and high 1,25-(OH)2 Vit.D3 levels were noted despite cholecalciferol supplementation for a year, suggesting that 1-α-hydroxylase overexpression caused by sarcoidosis accelerated the conversion from 25-OH Vit.D3 to 1,25-(OH)2 Vit.D3.
Interventions: Although initially resistant to preservative management, the hypercalcemia promptly improved after starting corticosteroid treatment.
Outcomes: Hypercalcemia and acute kidney injury were normalized after corticosteroid treatment.
Lessons: We should be aware of patients' medications, especially in patients with granulomatosis disease. The concomitant measurement of 25-OH Vit.D3 and 1,25-(OH)2 Vit.D3 levels is useful for determining the cause of hypercalcemia.
📄 Download the PDF from VitaminDWiki
Still unsure of the role of Vitamin D in sarcoidosis – Nov 2020
Role of vitamin D in sarcoidosis
Review Fac Rev . 2020 Nov 18;9:14. doi: 10.12703/b/9-14. eCollection 2020
Fabiola Gianella 1, Connie Cw Hsia 1 2, Khashayar Sakhaee 3 2
Higher Vitamin D levels do not statistically increase Calcium levels


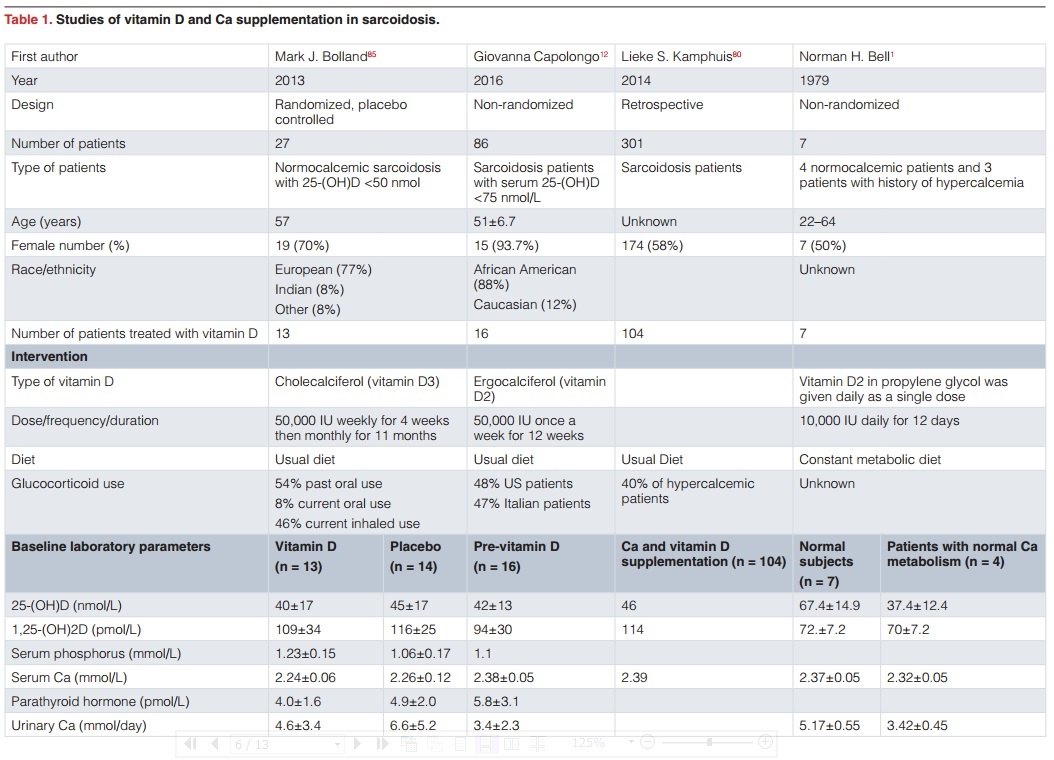
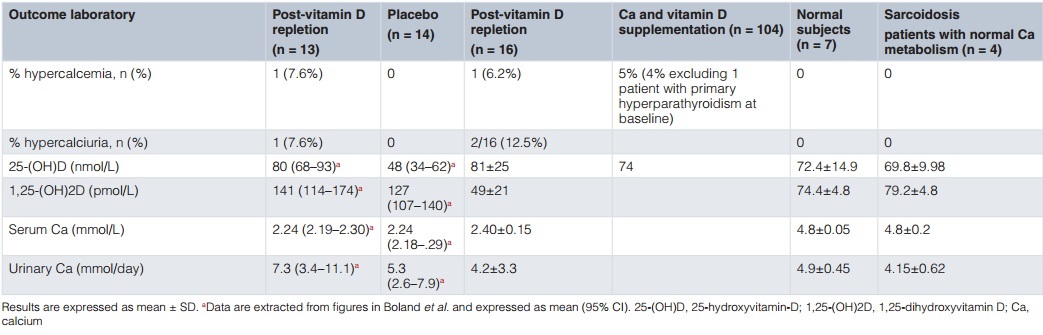
After the initial description of extrarenal synthesis of 1,25-dihydroxyvitamin D (1,25-(OH)2D) three decades ago, extensive progress has been made in unraveling the immunomodulatory roles of vitamin D in the pathogenesis of granulomatous disorders, including sarcoidosis. It has been shown that 1,25-(OH)2D has dual effects on the immune system, including upregulating innate immunity as well as downregulating the autoimmune response. The latter mechanism plays an important role in the pathogenesis and treatment of sarcoidosis. Vitamin D supplementation in patients with sarcoidosis has been hampered owing to concerns about the development of hypercalcemia and hypercalciuria given that extrarenal 1-α hydroxylase is substrate dependent. Recently, a few studies have cast doubt over the mechanisms underlying the development of hypercalcemia in this population. These studies demonstrated an inverse relationship between the level of vitamin D and severity of sarcoidosis. Consequently, clinical interest has been piqued in the use of vitamin D to attenuate the autoimmune response in this disorder. However, the development of hypercalcemia and the attendant detrimental effects are real possibilities. Although the average serum calcium concentration did not change following vitamin D supplementation, in two recent studies, hypercalciuria occurred in one out of 13 and two out of 16 patients. This review is a concise summary of the literature, outlining past work and newer developments in the use of vitamin D in sarcoidosis. We feel that larger-scale placebo-controlled randomized studies are needed in this population. Since the current first-line treatment of sarcoidosis is glucocorticoids, which confer many systemic adverse effects, and steroid-sparing immunosuppressant treatment options carry additional risks of adverse effects, adjunct management with vitamin D in combination with potent anti-osteoporotic medications could minimize the risk of glucocorticoid-induced osteoporosis and modulate the immune system to attenuate disease activity in sarcoidosis.
📄 Download the PDF from VitaminDWiki
Sarcoidosis WIKIPEDIA
Vitamin D dysregulation
Sarcoidosis frequently causes a dysregulation of vitamin D production with an increase in extrarenal (outside the kidney) production.[25] Specifically, macrophages inside the granulomas convert vitamin D to its active form, resulting in elevated levels of the hormone 1,25-dihydroxyvitamin D and symptoms of hypervitaminosis D that may include fatigue, lack of strength or energy, irritability, metallic taste, temporary memory loss or cognitive problems. Physiological compensatory responses (e.g., suppression of the parathyroid hormone levels) may mean the patient does not develop frank hypercalcemia. This condition may be aggravated by high levels of estradiol and prolactin such as in pregnancy, leading to hypercalciuria and/or compensatory hypoparathyroidism.[26] High levels of Vitamin D are also implicated in immune-system dysfunctions which tie into the sarcoid condition.
Epidemiology – fewer than 2 in 10,000
Sarcoidosis most commonly affects young adults of both sexes, although studies have reported more cases in females.
Incidence is highest for individuals younger than 40 and peaks in the age-group from 20 to 29 years; a second peak is observed for women over 50.[37][51]
Sarcoidosis occurs throughout the world in all races with an average incidence of 16.5/100,000 in men and 19/100,000 in women.
The disease is most prevalent in Northern European countries, and the highest annual incidence of 60/100,000 is found in Sweden and Iceland.
In the United States, sarcoidosis is more common in people of African descent than Caucasians, with annual incidence reported as 35.5 and 10.9/100,000, respectively.[52] Sarcoidosis is less commonly reported in South America, Spain, India, Canada, and the Philippines.
The Marshall protocol , developed by an electrical engineer diagnosed with sarcoidosis Trevor Marshall, hypothesizes that bacteria lacking cell walls can live inside immune cells and thus evade detection and elimination by the immune system. The theory is not accepted by most doctors, and is supported only through anecdotal evidence.[27]
Vitamin D REDUCES the probability of Sarcoidosis Hypercalcemia - Nov 2014
Calcium and Vitamin D in Sarcoidosis: Is Supplementation Safe?
Journal of Bone and Mineral Research, Volume 29, Issue 11, pages 2498–2503, November 2014
Lieke S Kamphuis1,2,*, Femke Bonte-Mineur3, Jan A van Laar1,2, P Martin van Hagen1,2 andPaul L van Daele1,2
Article first published online: 20 OCT 2014
DOI: 10.1002/jbmr.2262
© 2014 American Society for Bone and Mineral Research
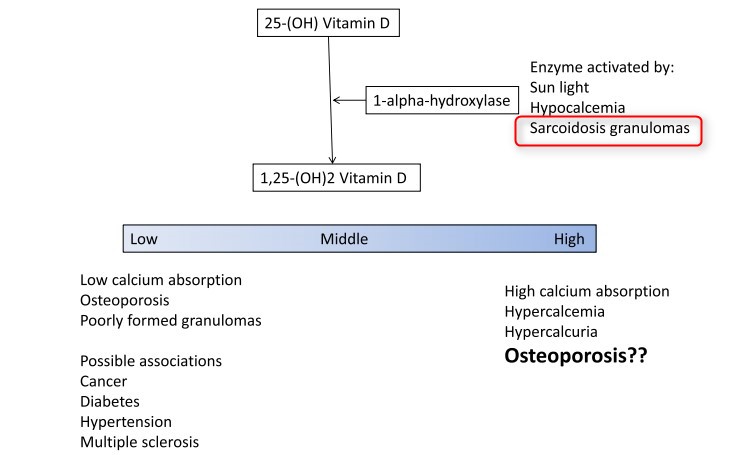
Granulomas in sarcoidosis express high levels of 1α-hydroxylase, an enzyme that catalyzes the hydroxylation of 25-OH vitamin D to its active form, 1,25(OH)2 vitamin D. Overproduction of 1α-hydroxylase is held responsible for the development of hypercalcemia in sarcoidosis patients. Corticosteroids are used as first-line treatment in organ-threatening sarcoidosis. In this light, osteoporosis prevention with calcium and vitamin D (CAD) supplementation is often warranted. However, sarcoidosis patients are at risk for hypercalcemia, and CAD supplementation affects the calcium metabolism. We studied calcium and vitamin D disorders in a large cohort of sarcoidosis patients and investigated if CAD supplementation is safe. Retrospectively, data of 301 sarcoidosis patients from July 1986 to June 2009 were analyzed for serum calcium, 25-hydroxy vitamin D (25-(OH)D), 1,25-dihydroxy vitamin D (1,25(OH)2D), and use of CAD supplementation. Disease activity of sarcoidosis was compared with serum levels of vitamin D. Hypercalcemia occurred in 8%. A significant negative correlation was found between 25-(OH)D and disease activity of sarcoidosis measured by somatostatin receptor scintigraphy. In our study, 5 of the 104 CAD-supplemented patients developed hypercalcemia, but CAD supplementation was not the cause of hypercalcemia. Patients without CAD supplementation were at higher risk for developing hypercalcemia . During CAD supplementation, no hypercalcemia developed as a result of supplementation. Hypovitaminosis D seems to be related with more disease activity of sarcoidosis and, therefore, could be a potential risk factor for disease activity of sarcoidosis. Thus, vitamin D–deficient sarcoidosis patients should be supplemented
publisher charges $5 to rent the PDF
Very very rare for a person to have sarcoidosis AND problems with Calcium+Vitamin D (1 in 100,000)
About 1 in 10 patients with Sarcoidosis had problems with combination of Calcium and Vitamin D
Calcium and Vitamin D in Sarcoidosis: Is Supplementation Safe? JBMR April 2014
Marshal Protocol
Marshal Protocol Knowledgebase by 2011 he appears to be talking about many other causes and effects - not just Vitamin D
Opposition to Marshal protocol - Vasquez April 2015
📄 Download the PDF from VitaminDWiki
Heart Lung Blood Institute of NIH February 2009
What Is Sarcoidosis?
Sarcoidosis (sar-koy-DO-sis) is a disease of unknown cause that leads to inflammation.
It can affect various organs in the body.
Normally, your immune system defends your body against foreign or harmful substances.
For example, it sends special cells to protect organs that are in danger.
These cells release chemicals that recruit other cells to isolate and destroy the harmful substance.
Inflammation occurs during this process. Once the harmful substance is destroyed, the cells and the inflammation go away.
In people who have sarcoidosis, the inflammation doesn't go away.
Instead, some of the immune system cells cluster to form lumps called granulomas (gran-yu-LO-mas) in various organs in your body.
Overview
Sarcoidosis can affect any organ in your body. However, it's more likely to occur in some organs than in others.
The disease usually starts in the lungs, skin, and/or lymph nodes (especially the lymph nodes in your chest).
The disease also often affects the eyes and the liver. Although less common, sarcoidosis can affect the heart and brain, leading to serious complications.
If many granulomas form in an organ, they can affect how the organ works.
This can cause signs and symptoms. Signs and symptoms vary depending on which organs are affected.
Many people who have sarcoidosis have no symptoms or mild symptoms.
Lofgren's syndrome is a classic set of signs and symptoms that is typical in some people who have sarcoidosis.
Lofgren's syndrome may cause fever, enlarged lymph nodes, arthritis (usually in the ankles), and/or erythema nodosum (er-i-THE-ma no-DO-sum).
Erythema nodosum is a rash of red or reddish-purple bumps on your ankles and shins. The rash may be warm and tender to the touch.
Treatment for sarcoidosis also varies depending on which organs are affected.
Your doctor may prescribe topical treatments and/or medicines to treat the disease.
Not everyone who has sarcoidosis needs treatment.
Outlook
The outcome of sarcoidosis varies. Many people recover from the disease with few or no long-term problems.
More than half of the people who have sarcoidosis have remission within 3 years of diagnosis.
"Remission" means the disease isn't active, but it can return.
Two-thirds of people who have the disease have remission within 10 years of diagnosis.
People who have Lofgren's syndrome usually have remission. Relapse (return of the disease) 1 or more years after remission occurs in less than 5 percent of patients.
Sarcoidosis leads to organ damage in about one-third of the people diagnosed with the disease.
Damage may occur over many years and involve more than one organ. Rarely, sarcoidosis can be fatal.
Death usually is the result of complications with the lungs, heart, or brain.
Poor outcomes are more likely in people who have advanced disease and show little improvement from treatment.
Certain people are at higher risk for poor outcomes from chronic (long-term) sarcoidosis.
This includes people who have lung scarring, heart or brain complications, or lupus pernio (LU-pus PAR-ne-o).
Lupus pernio is a serious skin condition that sarcoidosis may cause.
Research is ongoing for new and better treatments for sarcoidosis.
- - - - did not copy a section - - - -
Common Signs and Symptoms
In both adults and children, the disease most often affects the lungs.
If granulomas (inflamed lumps) form in your lungs, you may wheeze, cough, feel short of breath, or have chest pain. Or, you may have no symptoms at all.
Some people who have sarcoidosis feel very fatigued (tired), uneasy, or depressed.
Night sweats and weight loss are common symptoms of the disease.
Common signs and symptoms in children are fatigue, loss of appetite, weight loss, bone and joint pain, and anemia.
Children who are younger than 4 years old may have a distinct form of sarcoidosis.
It may cause enlarged lymph nodes in the chest (which can be seen on a chest x ray), skin lesions, and eye swelling or redness.
Other Signs and Symptoms
Sarcoidosis may affect your lymph nodes. The disease can cause enlarged lymph nodes that feel tender.
Sarcoidosis usually affects the lymph nodes in your neck and chest.
However, the disease also may affect the lymph nodes under your chin, in your armpits, or in your groin.
Sarcoidosis can cause lumps, ulcers, or areas of discolored skin.
They may itch, but they don't hurt. These signs tend to appear on your back, arms, legs, and scalp.
Sometimes they appear near your nose or eyes. These signs usually last a long time.
Sarcoidosis may cause a more serious skin condition called lupus pernio.
Disfiguring skin sores may affect your nose, nasal passages, cheeks, ears, eyelids, and fingers.
These sores tend to be ongoing. They can return after treatment is over.
Sarcoidosis also can cause eye problems. If you have sarcoidosis, it's important to have an annual eye exam.
If you have changes in your vision and can't see as clearly or can't see color, call 9–1–1 or have someone drive you to the emergency room.
You should call your doctor if you have any new eye symptoms, such as burning, itching, tearing, pain, or sensitivity to light.
Signs and symptoms of sarcoidosis also may include an enlarged liver, spleen, or salivary glands.
Although less common, sarcoidosis can affect the heart and brain.
This can cause a number of symptoms, such as abnormal heartbeats, shortness of breath, headaches, and vision problems.
If sarcoidosis affects the heart or brain, serious complications can occur.
- - - - did not copy a section - - - - -
Key Points
Sarcoidosis is a disease of unknown cause that leads to inflammation. It can affect various organs in the body.
Sarcoidosis is more likely to occur in some organs than in others. The disease usually starts in the lungs, skin, and/or lymph nodes (especially the lymph nodes in your chest). The disease also often affects the eyes and the liver.
In people who have sarcoidosis, immune system cells cause inflammation and cluster to form lumps called granulomas.
If many granulomas form in an organ, they can affect how the organ works. This can cause signs and symptoms. Signs and symptoms vary depending on which organs are affected. Many people who have sarcoidosis have no symptoms or mild symptoms.
Some researchers think that sarcoidosis develops when your immune system responds to a trigger, such as bacteria, viruses, dust, or chemicals. Genetics also may play a role in sarcoidosis.
Sarcoidosis affects people of all ages and races. In the United States, the disease affects African Americans somewhat more often and more severely than Whites. The disease also is slightly more common in women than in men. It usually develops between the ages of 20 and 50.
In both adults and children, the disease most often affects the lungs. If granulomas form in your lungs, you may wheeze, cough, feel short of breath, or have chest pain. Some people who have sarcoidosis feel very fatigued (tired), uneasy, or depressed. Night sweats and weight loss are common symptoms of the disease.
Lofgren's syndrome is a classic set of signs and symptoms that appear in some people when they first develop sarcoidosis. Signs and symptoms may include fever, enlarged lymph nodes, arthritis, and erythema nodosum (a rash of red or reddish-purple bumps on your ankles).
Your doctor will diagnose sarcoidosis based on your medical history, a physical exam, and the results from tests. He or she will look for granulomas (inflamed lumps) in your organs. Your doctor also will try to rule out other causes of your symptoms.
Whether you need treatment and what type of treatment you need depend on your signs and symptoms, which organs are affected, and whether those organs are working well.
Your doctor may prescribe topical treatments and/or medicines to treat the disease. Not everyone who has sarcoidosis needs treatment. In some cases, the disease goes away on its own.
If the disease affects certain organs, such as your eyes, heart, or brain, you may need treatment even if you don't have any symptoms.
Sarcoidosis has no cure. However, you can take steps to manage the disease. Get ongoing care and follow a healthy lifestyle. Talk to your doctor if you're pregnant or planning a pregnancy.
Getting ongoing care is important, even if you don't take medicine for your sarcoidosis. New symptoms can occur at any time. Also, your condition can slowly worsen without your noticing.
The outcome of sarcoidosis varies. Many people recover from the disease with few or no long-term problems.
Rarely, sarcoidosis can be fatal. Death usually is the result of complications with the lungs, heart, or brain. Poor outcomes are more likely in people who have advanced disease and show little improvement from treatment.
Hypercalcaemia in asymptomatic sarcoidosis unmasked by a vitamin D loading dose.
Eur Respir J. 2011 Feb;37(2):470-1.
Amrein K, Schilcher G, Fahrleitner-Pammer A.
Division of Endocrinology and Metabolism, Dept of Internal Medicine, Medical University of Graz, Auenbruggerplatz 15, A-8036 Graz, Austria. E-mail: karin.amrein@medunigraz.at. PMID: 21282814
Note from the PDF: about 2% of the people with Sarcoidosis have excessive Calcium = 2% of 2 in 10,000 = 4 in 1 million people
[tiki-download_file.php?fileId=1663]
Editorial: 10-20 ng appears best for rare patients with Sarcoidosis - May 2014
Goldilocks, vitamin D and sarcoidosis.
Arthritis Res Ther. 2014 May 23;16(3):111. [Epub ahead of print]
Baughman RP, Lower EE.
While low levels of vitamin D can increase the risk for osteoporosis, excessive amounts of vitamin D may also be problematic. Hypercalcemia and hypercalciuria due to increased vitamin D activity occur in a significant proportion of sarcoidosis patients. Saidenberg-Kermanac'h and colleagues compared vitamin D levels with bone fragility fractures in their sarcoidosis clinic. They found that a 25-(OH) vitamin D level between 10 and 20 ng/ml was associated with the lowest risk of bone fractures and paradoxically higher levels increased the risk of bone fractures. Using less vitamin D supplementation may simultaneously lower the risk for bone fracture and hypercalcemia in sarcoidosis.
PMID: 25166268
PDF is attached at the bottom of this page
Vitamin D concentration and patient reported outcomes in sarcoidosis - Sept 2015
European Respiratory Journal
Branislav S. Gvozdenovic, Violeta Vucinic, Mira Vukovic, Mihailo Stjepanovic
DOI: 10.1183/13993003.congress-2015.PA3687 Published 1 September 2015
Sarcoidosis patients frequently have low inactive Vitamin D form levels accompanied with the increased levels of the active form due to its autonomic conversion in sarcoid granulomas.
The aim of our study was to evaluate the influence of lower serum Vitamin D3 concentration on subjective disease outcomes – fatigue and depression.
In the cross-sectional study the degree of fatigue and depression was measured in 400 (27.3% males) patients with pulmonary sarcoidosis.
Fatigue was measured by standardized Fatigue Assessment Scale (FAS). Depression was assessed by CES-D instrument.
Mean age of patients was 50.5±11 years; average duration of the disease 6.1±6.1 years; mean Vitamin D3 level was 14.2±10.2 µg/L.
Mean FAS score was 21.9±6.3. Fatigue (FAS scores ≥ 22) was present in 186 (46.5%) patients.
Mean CES-D score was 14.4±8.4. Clinically defined depression (CES-D scores ≥ 16) had 128 patients (32%).
We found a significant correlation between mean Vitamin D3 levels and physical and mental components of fatigue (p=0.017 and p=0.018, respectively), but the correlation with the total FAS scores was absent. We also noticed a significant correlation between mean Vitamin D levels and CES-D scores (p=0.044). FAS score, Vitamina D3 and symptoms score were highly significant independent predictors of the depression in sarcoidosis patients. A highly significant canonic discriminative function (Wilks' Lambda=0.642; χ2=145.22; p<0.001) was found. These predictors explained 81.5% of variance of the categorical variable depression present – yes/no.
It is very important to regularly measure serum Vitamin D3 levels in sarcoidosis patients since it can significantly influence subjective disease outcomes, the depression in particular.
See web
The role of vitamin D in sarcoidosis - Nov 2020. doi: 10.12703/b/9-14 FREE PDF
Vitamin D status in sarcoidosis: a cross-sectional study - Aug 2018 doi: 10.36141/svdld.v35i2.6199
Vitamin D Supplementation in Sarcoidosis: A Double-Edged Sword - 2022 DOI: 10.1055/s-0041-1736280 📄 PDF
- 1 person with Sarcoidosis taking 60,000 IU of vitamin D weekly
Hypercalcemia in sarcoidosis unmasked by treatment with Vitamin D - 2022 10.1530/endoabs.81.EP168
- Sarcodisis got worse with a vitamin D loading dose (3 doses of 40,000 IU weekly)
See VitaminDWiki
Sarcoidosis – low on vitamin D3 but OK or high level of D2– Feb 2011
Boron and Granulomas (TB, Rheumatoid arthritis, Crohn's, Rheumatic Fever etc.) - 2015