Multiple Sclerosis incidence is still associated with latitude
Latitude continues to be significantly associated with the prevalence of multiple sclerosis: an updated meta-analysis.
J Neurol Neurosurg Psychiatry. 2019 Nov;90(11):1193-1200. doi: 10.1136/jnnp-2018-320189
Simpson S Jr1,2, Wang W3,4, Otahal P2, Blizzard L2, van der Mei IAF2, Taylor BV2.
#00F: Download the PDF from
Sci-Hub via VitaminDWiki
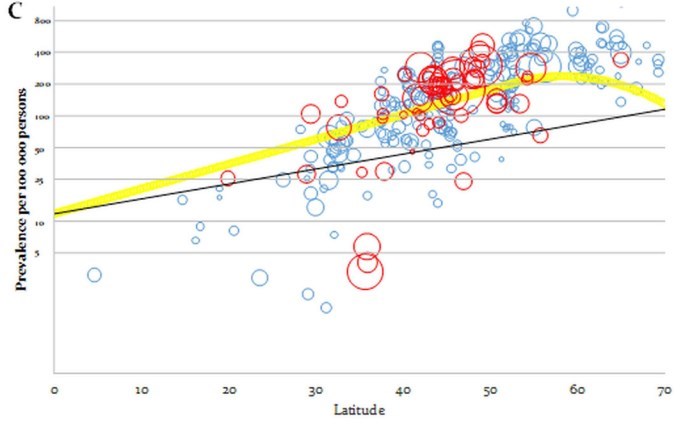
points in blue are the prevalence points from the original study,
while those in red are those from the present study.
size of bubbles is proportionate to the inverse of the sample variance. (Bigger = Better? = less variance)
Map

Speculation by VitaminDWiki - people living >60 latitude probalby consume more oily fish. cod liver oil, or Vit D supplements
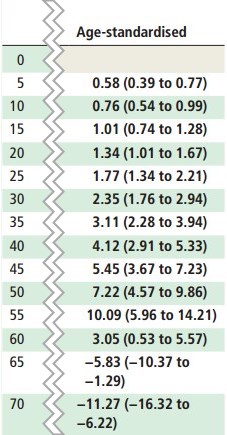
Estimated change in prevalence per 100 000 persons per degree latitude
at 5-unit increments of latitude, estimated at 2018
(# is proportional to the slope of the curve, not the prevalence)
OBJECTIVES:
Previous studies have demonstrated a strong latitudinal gradient in multiple sclerosis (MS) prevalence. Herein, we present a meta-analysis of the latitudinal gradient of MS prevalence including studies published since our 2011 review, seeking to assess the latitudinal gradient and whether it has changed since our previous analysis.
METHODS:
Studies published up to December 2018 were located via Embase, Web of Knowledge and PubMed, using standardised search terms; data were extracted from peer-reviewed studies and these studies added to those from our previous analysis. Where age-specific data were available, prevalence estimates were age-/sex-standardised to the 2009 European population. Prevalence estimates were adjusted for study prevalence year and ascertainment methods. The latitudinal association with MS prevalence was assessed by meta-regression.
RESULTS:
A total of 94 studies met inclusion criteria, yielding 230 new prevalence points and 880 altogether with those from the prior study. There was a significant positive gradient in time-corrected MS prevalence with increasing latitude (5.27/100 000 per degree latitude), attenuating slightly to 4.34/100 000 on age-standardisation, these associations persisting on adjustment for ascertainment method. Of note, the age-standardised gradient was consistently significantly enhanced from our previous study, regardless of whether it was as-measured, time-corrected or adjusted for ascertainment methods. Certain areas, such as the Scandinavian and Atlantic Coast/Central Europe regions, showed changes in MS prevalence gradient over time, but other regional gradients were similar.
CONCLUSIONS:
This new meta-analysis confirms that MS prevalence is still strongly positively associated with increasing latitude and that the gradient is increasing, suggesting that potentially modifiable environmental factors, such as sun exposure, are still strongly associated with MS risk.