Consultation to medical professionals on Vitamin D Testing
Pathology Consultation on Vitamin D Testing
Matthew D. Krasowski, MD, PhD Pathology Consultation / Special Article
Key Words: Calcitriol; Calcium metabolism disorders; Osteoporosis; Reference standards; Reference values; Vitamin D
DOI: 10.1309/AJCPB50USETUOQDZ
See also VitaminDWiki
- All items in category Test for D 40 items as of Oct 2011
- Many on variation between tests: different days, different testing methods
One vitamin D blood test said toxic the other said normal – Aug 2010
Vitamin D blood test uncertainty about 15 percent – Aug 2010
Vitamin D measurements of individuals vary considerably within 6 days – June 2011
(The following is the text extracted from the PDF at the bottom of this page)
Upon completion of this activity you will be able to:
describe the potential health consequences of vitamin D deficiency or excess.
analyze the 2 main methods (immunoassay, liquid chromatography/ tandem mass spectrometry) used for measuring 25-hydroxyvitamin D serum/plasma concentrations
- and how they may produce different results (including obtaining fractionated vs total 25-hydroxyvitamin D concentrations).
- define the indications for assessing 1,25-dihydroxyvitamin D (most biologically active form of vitamin D).
The ASCP is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The ASCP designates this journal-based CME activity for a maximum of 1 AMA PRA Category 1 Credit™ per article. Physicians should claim only the credit commensurate with the extent of their participation in the activity. This activity qualifies as an American Board of Pathology Maintenance of Certification Part II Self-Assessment Module.
The authors of this article and the planning committee members and staff have no relevant financial relationships with commercial interests to disclose.
Questions
What testing is appropriate for assessment of vitamin D nutritional status, and which patients should have vitamin D testing?
What do the data in the published literature show with regard to association of vitamin D deficiency with disease?
What laboratory values raise concern for risk of serious complications such as secondary hyperparathyroidism or osteoporosis-related bone fractures?
How are 25-hydroxyvitamin D reference ranges (or target values) established, and how do they vary across marketed assays and reference laboratories?
If 25-hydroxyvitamin D2 and D3 serum concentrations are separately measured and reported as compared with receiving only a total 25-hydroxyvitamin D concentration,
- how do the additional fractionated data for vitamin D2 and D3 aid clinical interpretation?
What are the methods for measuring 25-hydroxyvitamin D serum concentrations, and how do they differ from one another? Is there standardization across assays?
When is measurement of a 1,25-dihydroxyvitamin D serum concentration clinically indicated?
What are the clinical implications of misordering 1,25-dihydroxyvitamin D in place of 25-hydroxy-vitamin D?
Exam is located at www.ascp.org/ajcpcme.
Abstract
The last decade has seen a substantial increase in clinical interest in vitamin D deficiency and of laboratory testing for vitamin D status.
Many clinical laboratories in the United States have seen requests for vitamin D testing increase 100% or more in the last 5 years.
The most common laboratory test to assess vitamin D nutritional status is total 25-hydroxyvitamin D serum concentrations.
Laboratory professionals are often confronted with challenges related to vitamin D testing, including controversy over optimal and target vitamin D concentrations, variable reference ranges across marketed assays and reference laboratories, lack of standardization of vitamin D assays, and misordering of 1,25-dihydroxyvitamin D testing.
This article presents a common clinical case scenario regarding vitamin D and an up-to-date discussion and review of the literature on vitamin D testing.
Case Scenario
A 62-year-old woman was seen in an internal medicine clinic at an academic medical center. She is concerned about osteoporosis, especially because her older sister recently had a hip fracture at the age of 64 years. She is additionally concerned about vitamin D deficiency, having heard this topic discussed on a daytime television talk show. The patient had laboratory testing for vitamin D status 12 months earlier at a community hospital; the test was done by a commercial laboratory and showed a total 25-hydroxyvitamin D serum concentration determined by liquid chromatography/tandem mass spectrometry (LC/ MS/MS) of 26 ng/mL (65 nmol/L; >25 ng/mL [62 nmol/L] defined as "optimal" in the reference range).
At the internal medicine clinic, the physician ordered laboratory tests using the hospital computer order system. To check vitamin D status, the physician selected a vitamin D panel that includes 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D serum levels. The 25-hydroxyvitamin D serum concentration was determined at the medical center central clinical laboratory by enzyme immunoassay, and results were 29 ng/mL (72 nmol/L), which is in the "insufficiency" range according to the reference ranges on the package insert for the assay. The 1,25-dihydroxyvitamin serum concentration was determined by a reference laboratory by LC/MS/MS, and results were 55 pg/mL (143 pmol/L; reference range, 18-72 pg/mL [47187 pmol/L]). The internal medicine physician is perplexed about the results of the laboratory testing and contacts the clinical chemistry director for consultation.
Background
Vitamin D is an essential fat-soluble vitamin that affects nearly every organ system via interactions with the vitamin D receptor, a nuclear hormone receptor that acts as a transcriptional regulator of diverse physiologic processes.1 In the last 2 decades, there has been increasing interest in the biology of vitamin D and a growing recognition that vitamin D insufficiency is common throughout the world.2-4 One consequence of the growing clinical attention to vitamin D has been a substantial increase in laboratory testing for vitamin D. In the United States, many clinical laboratories have experienced increases in vitamin D testing of 100% or more in the last 5 years.5 This increase produces challenges for clinical laboratories, as will be discussed in this review.
Vitamin D was first recognized as a vitamin in the early 20th century as a factor in cod liver oil that prevented the development of rickets, a syndrome of bone weakening in children that can lead to fractures and permanent skeletal deformity.6 The "classic" actions of vitamin D are in the regulation of mineral metabolism, primarily by influencing renal reabsorption of calcium and phosphate and intestinal absorption of calcium.2 Vitamin D and parathyroid hormone (PTH) together serve as the most important physiologic regulators of calcium and phosphorus. Abnormal vitamin D serum or plasma concentrations trigger compensatory changes in PTH levels.7 For example, prolonged vitamin D deficiency can lead to a sustained increase in PTH secretion, a condition known as secondary hyperparathyroidism.
To complement the well-known role of vitamin D in mineral metabolism, research has demonstrated an increasing list of "nonclassic" vitamin D actions, including effects on immune modulation, cell cycle proliferation, and brain health.8,9 Vitamin D deficiency has now been associated with increased risk of multiple sclerosis, certain cancers (especially breast, colorectal, and prostate), and chronic respiratory infections (eg, tuberculosis).2 Consequently, vitamin D deficiency has health implications that extend well beyond skeletal abnormalities.
Nomenclature
The term vitamin D usually refers collectively to vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol), together known as the calciferols.2 Vitamins D2 and D3 are hydroxylated by the enzyme vitamin D 25-hydroxylase in the liver to form 25-hydroxyvitamin D2 or D3. 25-Hydroxyvitamin D (calcidiol) is the main storage form of vitamin D and also the analyte typically measured in serum or plasma to assess vitamin D stores. 25-Hydroxyvitamin D is further hydroxylated in the kidney by 25-hydroxyvitamin D 1a-hydroxylase to form 1,25-dihydroxyvitamin D (calcitriol), which represents the biologically most active form of vitamin D in terms of effects at the vitamin D receptor. 1,25-Dihydroxyvitamin D varies day-to-day much more than 25-hydroxyvitamin D and is, in fact, not a good marker of overall vitamin D nutritional status.2 In fact, it is possible to be profoundly deficient in overall stores of vitamin D yet have a 1,25-dihydroxyvitamin D serum or plasma concentration within the reference range owing to higher levels of PTH that cause greater conversion of 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D.10 As will be discussed, there are few clinical indications to assay serum or plasma 1,25-dihydroxyvitamin D concentration.
Reasons for Vitamin D Deficiency
A number of factors contribute to vitamin D deficiency. The first is decreased endogenous production.11 UV-B rays in sunlight convert 7-dehydrocholesterol in the skin to previtamin D3, which then rapidly converts to vitamin D3. This process requires a UV-B index of greater than 3. In practical terms, optimal endogenous vitamin D3 production in response to sunlight in the northern latitudes requires sunlight exposure in the warmer months and during peak sunlight hours (approximately 10:00 am to 3:00 pm). In the Northern Hemisphere above 35° latitude (roughly that of Atlanta, GA, in the United States), essentially no vitamin D3 is produced endogenously from November to March, even with direct sunlight exposure. Consequently, for many people in the United States during the winter months, the only substantial source of vitamin D is from the diet. Even in climates in lower latitudes that have abundant sunlight, people who reside predominantly indoors during peak daylight hours produce very little vitamin D endogenously. Sunscreen use also dramatically decreases vitamin D production.11 Sunscreens with a sun protection factor of 15 or higher block 99% or more of vitamin D production. The ability to produce vitamin D also decreases as part of the aging process, mainly related to decreased availability of 7-dehydrocholesterol. Skin damage (eg, burns) can also reduce vitamin D production, depending on the extent of injury.12
The second main factor underlying vitamin D deficiency is low dietary intake.2 There are a relatively small number of foods that naturally contain high amounts of vitamin D.13 These include oily fish (eg, mackerel), eggs, and shiitake mushrooms. Animal sources of vitamin D generally contain vitamin D3 (the endogenous compound); however, farm-raised animals may be fed vitamin D2-enriched diets and, thus, have appreciable amounts of vitamin D2 in their tissues.14 Sun-dried shiitake mushrooms contain substantial amounts of vitamin D2, especially when exposed to UV light. The amount of vitamin D in supplements varies considerably.2 Most multivitamins contains 400 IU of vitamin D2 or D3. Vitamin D3 supplements generally contain 400, 800, 1,000, or 2,000 IU. There is a liquid supplement of vitamin D2 that contains 8,000 IU/mL and a vitamin D2 capsule containing 50,000 IU.
To enhance vitamin D intake on a population-wide basis, dairy products (eg, milk, butter) may be supplemented with vitamin D2 or D3.13 Nearly all of the milk sold in the United States is voluntarily fortified with 100 IU vitamin D2 or D3 per cup. With the decreasing intake of milk by children, the list of foods supplemented with vitamin D has expanded to include orange juice, cereals, and some other foods. Canada and the United States mandate fortification of infant formula with vitamin D. It is important to keep in mind that dietary intake of vitamin D is often much less than could be achieved with 30 minutes of direct sunlight.11,15 For example, sunlight equivalent to 1 minimal erythemal dose (just enough to achieve redness of skin in 24 hours) in the summertime can result in 20,000 IU of vitamin D3 production. In contrast, 3.5 ounces of fresh wild salmon contains 600 to 1,000 IU of vitamin D3, while most fortified beverages and foods (eg, milk, orange juice) contain only 100 IU per serving. Breast milk also contains low concentrations of vitamin D, especially in lactating women who themselves are vitamin D-insufficient.2
The third main factor that can contribute to vitamin D deficiency is malabsorption.2 Conditions that can reduce vitamin D absorption include use of bile acid sequestrants (eg, cholestyramine, colesevelam), cystic fibrosis, celiac disease, Whipple disease, Crohn disease, and gastric bypass surgery. Patients with these conditions are also at risk for deficiency in other fat-soluble vitamins (A, E, and K). In patients with these conditions, increased vitamin D supplementation may be indicated. Alternatively, use of tanning beds at subtanning intensities can be highly effective in increasing vitamin D production in the skin.2
Last, a number of other factors can lead to vitamin D deficiency. A group of drugs (eg, carbamazepine, phenobarbital, phenytoin, rifampin, and St John's wort) increase liver expression of cytochrome P-450 enzymes that accelerate clearance of the active forms of vitamin D.16 Vitamin D supplementation is advised in patients receiving extended therapy with such medications, as may occur in conditions such as epilepsy and tuberculosis. Severe liver deficiency impairs 25-hydroxylation of vitamin D2 and D3. Not surprisingly, liver transplant recipients have a high prevalence of severe vitamin D deficiency.17 In nephrotic syndrome, vitamin D binding protein can be lost in the urine along with the bound vitamin D.2 There are also rare inborn errors of the vitamin D synthetic pathway or of the vitamin D binding protein that can cause vitamin D deficiency.18 In primary hyperparathyroidism, increased synthesis of 1,25-dihydroxyvitamin D leads to accelerated catabolism of 25-hydroxyvitamin D.19
Methods for Measuring 25-Hydroxyvitamin D
There are a number of methods for measuring 25-hydroxyvitamin D in serum or plasma, including enzyme immunoassay, radioimmunoassay, high-performance liquid chromatography (HPLC), liquid chromatography-mass spectrometry (LC/MS), and LC/MS/MS.10,20
Radioimmunoassay represented the first reliable technology for measuring total 25-hydroxyvitamin D, although enzyme immunoassay and LC/MS techniques have become more common. LC/MS/MS can readily distinguish 25-hydroxyvitamin D2 and D3, and clinical laboratories using this method can individually quantitate and report both analytes, in addition to providing a total 25-hydroxyvitamin D concentration. The clinical advantages of obtaining "fractionated" 25-hydroxyvitamin D2 and D3 measurements include the ability to assess endogenous vitamin D3 production and to determine compliance with vitamin D2 therapy. For example, a severe deficiency of vitamin D3 indicates lack of endogenous production and dietary intake. However, for most clinical situations, a total 25-hydroxyvitamin D concentration is sufficient.
The explosion of interest in monitoring vitamin D levels has revealed a number of challenges and controversies related to the various methods of determining 25-hydroxyvitamin D serum or plasma concentrations.10,20 One of the main challenges is the need to measure 25-hydroxyvitamin D2 and D3, which is particularly critical in a country such as the United States that heavily uses vitamin D2 in dietary supplements and to fortify food. Most immunoassay methods measure total 25-hydroxyvitamin D owing to antibody cross-reactivity with both 25-hydroxyvitamin D2 and D3.10,20 For these methods, the antibody or antibodies used in the assay ideally would cross-react equally with 25-hydroxyvitamin D2 and D3 (and not with other vitamin D compounds in the serum or plasma) and thereby produce an accurate measurement of total 25-hydroxyvitamin D. In practice, this is challenging to achieve, as revealed by comparisons of immunoassay and mass spectrometry-based measurements.21-23 For example, in 1 study, 2 commercial immunoassays showed significant deviation from linearity and highly variable results in comparison with the reference method of LC/MS/MS.22
Other factors contributing to interassay variability include lack of standardization between methods, varying preanalytic purification schemes, the C-3 epimer issue, and interlaboratory differences in operating procedures.20 Standardization of 25-hydroxyvitamin D measurements has been aided by the development of standard reference material by the National Institute of Standards and Technology (United States)24 and ongoing efforts to standardize immunoassay and LC/MS/MS methods.20 One challenging issue is the discovery that certain patients, mainly infants (younger than 12 months), have high concentrations of a 25-hydroxyvitamin D3 isomer with epimeric variation at carbon-3 (C-3).25 The C-3 epimer can produce considerable problems with vitamin D measurements in infants, and currently only a limited number of reference laboratories have validated LC/MS/MS methods to deal with infant samples. Expert panels associated with the United Kingdom Food Standards Agency26 and the US National Health and Nutrition Examination Survey27 have recommended LC/MS/MS as the reference method for measuring 25-hydroxyvitamin D, with attention to be given to integrating the available standard reference materials and the ability to discriminate the C-3 epimer of 25-hydroxyvitamin D3. These national efforts will likely spur further improvements in 25-hydroxyvitamin D measurements.
Reference Ranges for 25-Hydroxyvitamin D
One of the major areas of discussion in the vitamin D literature is what should be the appropriate reference/target ranges for 25-hydroxyvitamin D.2 There are a number of challenges here. First, population-based reference ranges are problematic owing to the variability of 25-hydroxyvitamin D levels across different ethnic backgrounds, geographic locations, and seasons. Second, there is substantial evidence that vitamin D deficiency is common in the United States and many other countries, making it difficult to define a "normal" population. Last, what defines normal or optimal with regard to vitamin D status is a matter of debate, with some authorities indicating that many people, even people without signs or symptoms of pathology, are deficient or borderline deficient in vitamin D stores.2,4,28
One physiologic approach to define 25-hydroxyvitamin D ranges is to look at the relationship between 25-hydroxyvitamin D and PTH levels. These show an inverse relationship with PTH concentrations rising as the 25-hydroxyvitamin D concentration decreases.7 This is an important physiologic means to maintain calcium homeostasis. PTH begins to increase substantially when 25-hydroxyvitamin D concentrations drop below 30 to 40 ng/mL, suggesting that 25-hydroxyvitamin D levels below this range are not optimal, even though overt disease (eg, rickets, osteomalacia, bone pain) may not be evident. Secondary hyperparathyroidism can be corrected with an average 25-hydroxyvitamin D serum or plasma level of 32 ng/mL (80 nmol/L), and at least 1 reference laboratory uses this value as the lower limit of optimal 25-hydroxyvitamin D serum and plasma concentrations iTable ii.4,7.28-41
An alternative approach to vitamin D reference ranges is to define clinical decision values for 25-hydroxyvitamin D serum and plasma concentrations such as the concentrations below which adverse health outcomes (especially osteoporotic-related bone fractures) increase significantly. This is the approach underlying the World Health Organization definition of vitamin D deficiency as a 25-hydroxyvitamin D serum or plasma concentration less than 20 ng/mL (50 nmol/L), which occurs in approximately 1 billion people worldwide.2 Some reference laboratories define optimal and deficient ranges for 25-hydroxyvitamin D concentrations, often with an insufficient or borderline deficient range in between. Some clinical decision values further delineate a "severe deficiency" range (often >10 ng/mL [10 nmol/L]) that have a high risk of serious skeletal abnormalities and, thus, warrant immediate treatment (Table 1).
Table 1
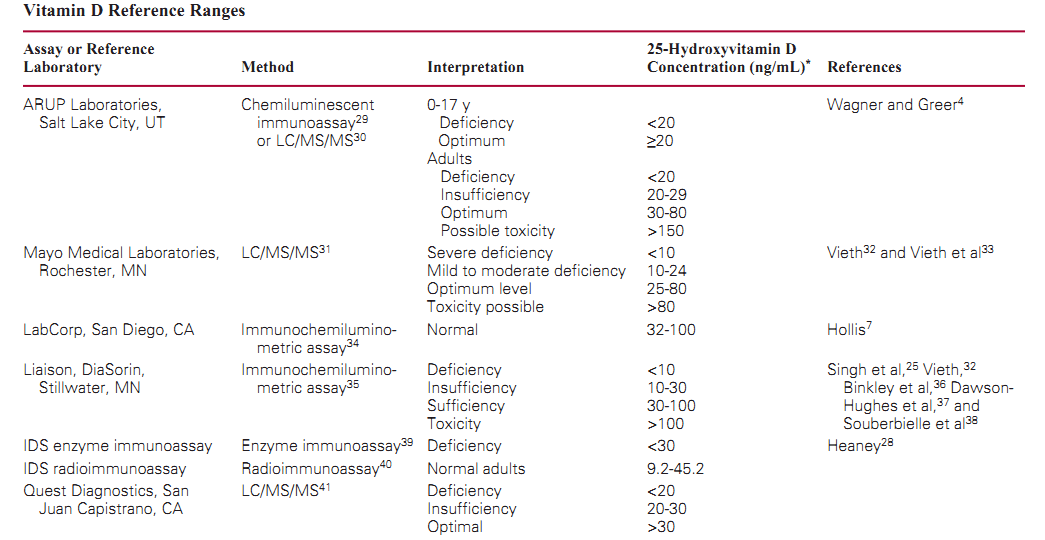
The lack of consensus on 25-hydroxyvitamin D target ranges results in substantial variation in the reference ranges or target values used by reference laboratories and manufacturers of 25-hydroxyvitamin D assays. Table 1 lists the ranges for 4 large reference laboratories in the United States and for 3 marketed immunoassays. Some of the ranges in Table 1 include a toxic concentration threshold that varies from 80 to 180 ng/mL (50-450 nmol/L). Combined with analytic variability in 25-hydroxyvitamin D concentrations across different laboratories and methods (discussed later), the lack of consistency of reference ranges makes it challenging for clinicians to assess multiple 25-hydroxyvitamin D concentrations for a given patient if performed at different laboratories. For example, a 25-hydroxyvitamin serum or plasma concentration of 26 ng/mL (65 nmol/L) could be interpreted as in the lower end of the "optimum" range in one laboratory but could result in the "insufficiency" range for another laboratory. The variety of Table 1 does not include reference ranges used by individual clinical laboratories that have developed their own method (eg, HPLC or LC/MS/MS) and set a reference range based on published literature or some other approach.
Vitamin D Toxic Ranges
Like vitamin A, vitamin D can cause toxic symptoms if taken in overdose.32 Indeed, high doses of vitamin D2 and D3 are used as rodenticides, and hypervitaminosis D can be seen in patients ingesting such compounds.42 However, vitamin D toxicity in humans appears to be rare, especially compared with the frequency of vitamin D deficiency, leading some to argue that the fear of vitamin D toxicity has prevented adoption of more extensive vitamin D supplementation throughout the population.43 Hypervitaminosis D is usually associated with prolonged exposure to very high doses of vitamin D (eg, >10,000 IU/d),32 with a number of case reports documenting vitamin D toxicity from frequent ingestion of supplements containing very high amounts of vitamin D.44-46 Excessive sunlight or exposure to tanning beds does not cause vitamin D toxicity because prolonged UV light exposure degrades vitamin D precursors, preventing excessive formation of vitamin D3.2
A 25-hydroxyvitamin D concentration of 80 ng/mL (200 nmol/L) is the lowest level reported to cause toxicity in patients without primary hyperparathyroidism,32 and some reference laboratories use this value as the lower limit of a potentially toxic 25-hydroxyvitamin D concentration range (Table 1). Patients with renal failure can have 25-hydroxyvitamin D concentrations higher than 80 ng/mL (200 nmol/L) without signs or symptoms of toxicity because conversion of 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D is impaired.2 Other reference laboratories have adopted higher limits for toxicity up to 150 ng/mL (Table 1).
1,25-Dihydroxyvitamin D
Although 1,25-dihydroxyvitamin D is the biologically active form of vitamin D, this analyte is not a good marker of overall vitamin D status for multiple reasons.10 First, the circulating half-life of 1,25-dihydroxyvitamin D is only 4 to 6 hours, contributing to variability in 1,25-dihydroxyvitamin D serum and plasma levels at different times. Second, the concentrations of 1,25-dihydroxyvitamin D in serum and plasma are about 1,000-fold less than 25-hydroxyvitamin D and, thus, can be difficult to measure. Third, and perhaps most important, overall vitamin D deficiency leads to decreased intestinal calcium absorption and a lower ionized calcium level, which, in turn, stimulates increased secretion of PTH. Ultimately, PTH increases the ionized calcium level by multiple mechanisms, including increased renal production of 1,25-dihydroxyvitamin D. Thus, overall vitamin D deficiency can actually lead to an increased 1,25-dihydroxyvitamin D concentration.
Measurement of 1,25-dihydroxyvitamin D is useful in some clinical circumstances, including renal failure (failure to 1a-hydroxylate 25-hydroxyvitamin D), granulomatous disease (eg, sarcoidosis, histoplasmosis), and workup of rare inborn errors of vitamin D metabolism. In granulomatous disease, there is increased conversion of 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D that can lead to hypercalcemia. Studies have shown an association of lower 1,25-dihydroxyvitamin D serum and plasma concentrations and higher mortality in patients with cardiac disease,47,48 HIV,49 and renal failure,50 although it is unclear how to translate this information to clinical decision making.
A survey of vitamin D ordering indicated that many clinical laboratories in the United States have also seen an increase in recent years in 1,25-dihydroxyvitamin D orders, although not usually as dramatic as for 25-hydroxyvitamin D.5 Given the relatively narrow clinical value of measuring 1,25-dihydroxyvitamin D serum and plasma concentrations, this raises the possibility that 1,25-dihydroxyvitamin D levels may be ordered in error. Two possible reasons for misordering include confusion of the 2 forms of vitamin D or a mistaken notion that monitoring the "active" form of vitamin D should be done to assess nutritional status. In addition, clinicians may request measurement of both 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D (perhaps thinking more information from this "panel" is helpful) when measuring only 25-hydroxyvitamin D alone is all that is needed for routine assessment of nutritional stores.
Conclusions
The growing clinical interest in vitamin D has led to dramatic increases in vitamin D testing. Consequently, laboratory professionals are confronted with the dual challenge of increasing testing volumes and helping clinicians navigate the complexities of vitamin D assays. iTable 2i summarizes some of the preanalytic, analytic, and postanalytic issues related to vitamin D testing. Clinical laboratory professionals can guide clinicians in appropriate indications for ordering 25-hydroxyvitamin D and also develop strategies to prevent inappropriate ordering of1,25-dihydroxyvitamin D. Education on 25-hydroxyvitamin D reference ranges can help place the results in a clinical context that can guide therapy and counseling of patients. Last, awareness of the limitations of the various 25-hydroxyvitamin D assays is especially important in comparing results across different assays, especially with the expected marketing of higher-throughput homogeneous immunoassays for 25-hydroxyvitamin D for automated instruments in the near future.
Table 2 Preanalytic, Analytic, and Postanalytic Factors Involved in Vitamin D Testing
Preanalytic Factors
Patient factors
Age
Endogenous vitamin D production
Vitamin D intake (diet, supplements, prescriptions)
Parathyroid disorders
Malabsorption
Liver or kidney dysfunction
Use of liver enzyme-inducing drugs
Other factors (eg, inborn errors, nephrotic syndrome]
Sample collection
Draw time in relation to large bolus dose of vitamin D
Ambient storage >24 h
Gross hemolysis, icterus, or lipemia
Clinician factors
Monitoring of 1,25-dihydroxyvitamin D
Ordering of other laboratory tests (eg, calcium, parathyroid hormone]
Analytic Factors
Method
Enzyme immunoassay Radioimmunoassay
High-performance liquid chromatography Liquid chromatography-tandem mass spectrometry
Calibration and standardization of assays
Immunoassay cross-reactivity with vitamins D2 and D3 Detection of C-3 epimer
Postanalytic Factors
Validation of reference ranges or target values
Misinterpretation of 1,25-dihydroxyvitamin D results
Interpretation of 25-hydroxyvitamin D results in the context of clinical history and other laboratory results
Case Summary
The patient had 2 measurements of 25-hydroxyvitamin D levels approximately 12 months apart, one by LC/MS/ MS at a reference laboratory and the other by enzyme immunoassay at a medical center clinical laboratory. The 2 values (26 and 29 ng/mL [65 and 72 nmol/L]) essentially show no change in the patient's overall vitamin D nutritional status, especially considering the known variability between 25-hydroxyvitamin D assay methods and fluctuations in the 25-hydroxyvitamin D level that may occur over time for any given person. The confusion for clinicians and the patient is mostly related to the different reference ranges associated with the 2 results. Although the first assay result fell (barely) into an "optimal" range in the reference range, the literature shows that 25-hydroxyvitamin D levels between 20 and 30 ng/mL (50-75 nmol/L) fit into a borderline category, more than the recognized deficiency threshold of 20 ng/mL (50 nmol/L) but less than the 25-hydroxyvitamin D levels that avoid a compensatory increase in the PTH level that can lead to secondary hyperparathyroidism. One approach to communicate with clinicians is to say that the patient's 25-hydroxyvitamin D level is not ideal but not yet in the range associated with severe deficiency.
The ordering of 1,25-dihydroxyvitamin D in this case was unnecessary and potentially misleading. For this patient, the 1,25-dihydroxyvitamin D level was within the reference range despite borderline deficient 25-hydroxyvitamin D levels, a situation that can result from increases in the PTH level. The discussion with the clinician can include some information on the lack of necessity of 1,25-dihydroxyvitamin D measurement in many patients and the narrow list of situations that warrant measurement of this active form of vitamin D. If 1,25-dihydroxyvitamin D misordering seems to be common, education of clinicians and, perhaps, review of electronic or paper order sets that allow for ordering of 1,25-dihydroxyvitamin D may be warranted.
From the Department of Pathology, University of Iowa Hospitals and Clinics, Iowa City.
Address reprint requests to Dr Krasowski: Dept of Pathology, University of Iowa Hospitals and Clinics, C671 GH, 200 Hawkins Dr, Iowa City, IA 52242.
References
Holick MF. Evolution and function of vitamin D. Recent Results Cancer Res. 2003;164:3-28.
Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357:266-281.
Lee JH, O'Keefe JH, Bell D, et al. Vitamin D deficiency: an important, common, and easily treatable cardiovascular risk factor? J Am Coll Cardiol. 2008;52:1949-1956.
Wagner CL, Greer FR. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. Pediatrics. 2008;122:1142-1152.
Rollins G. Vitamin D testing: what's the right answer? labs grapple with confusing analytics, evidence. Clin Lab News. July 2009;35:1, 6, 8.
Wharton B, Bishop N. Rickets. Lancet. 2003;362:1389-1400.
Hollis BW. Circulating 25-hydroxyvitamin D levels indicative of vitamin D sufficiency: implications for establishing a new effective dietary intake recommendation for vitamin D. J Nutr. 2005;135:317-322.
Holick MF. Vitamin D: extraskeletal health. Endocrinol Metab Clin North Am. 2010;39:381-400.
Nagpal S, Na S, Rathnachalam R. Noncalcemic actions of vitamin D receptor ligands. Endocr Rev. 2005;26:662-687.
Holick MF. Vitamin D status: measurement, interpretation, and clinical application. Ann Epidemiol. 2009;19:73-78.
Holick MF. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am J Clin Nutr. 2004;80(6 suppl):1678S-1688S.
Klein GL, Chen TC, Holick MF, et al. Synthesis of vitamin D in skin after burns. Lancet. 2004;363:291-292.
Ross AC, Taylor CL, Yaktine AL, et al, eds; Committee to Review Dietary Reference Intakes for Vitamin D and Calcium, Food and Nutrition Board; Institute of Medicine.
Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: National Academies Press; 2010.
Mattila P, Valaja J, Rossow L, et al. Effect of vitamin and D3-enriched diets on egg vitamin D content, production, and bird condition during an entire production period. Poult Sci. 2004;83:433-440.
Holick MF. Sunlight, UV-radiation, vitamin D and skin cancer: how much sunlight do we need? Adv Exp Med Biol. 2008;624:1-15.
Pascussi JM, Robert A, Nguyen M, et al. Possible involvement of pregnane X receptor-enhanced CYP24 expression in drug-induced osteomalacia. J Clin Invest. 005;115:177-186.
Stein EM, Cohen A, Freeby M, et al. Severe vitamin D deficiency among heart and liver transplant recipients. Clin Transplant. 2009;23:861-865.
Holick MF. Defects in the synthesis and metabolism of vitamin D. Exp Clin Endocrinol Diabetes. 1995;103:219-227.
Clements MR, Davies M, Hayes ME, et al. The role of 1,25-dihydroxyvitamin D in the mechanism of acquired vitamin D deficiency. Clin Endocrinol (Oxf). 1992;37:17-27.
Wallace AM, Gibson S, de la Hunty A, et al. Measurement of 25-hydroxyvitamin D in the clinical laboratory: current procedures, performance characteristics and limitations.
Steroids. 2010;75:477-488.
Chen H, McCoy LF, Schleicher RL, et al. Measurement of 25-hydroxyvitamin D3 (25OHD3) and 25-hydroxyvitamin D2 (25OHD2) in human serum using liquid chromatography-tandem mass spectrometry and its comparison to a radioimmunoassay method. Clin Chim Acta. 2008;391: 6-12.
Roth HJ, Schmidt-Gayk H, Weber H, et al. Accuracy and clinical implications of seven 25-hydroxyvitamin D methods compared with liquid chromatography-tandem mass spectrometry as a reference. Ann Clin Biochem. 2008;45:153-159.
van den Ouweland JM, Beijers AM, Demacker PN, et al. Measurement of 25-OH-vitamin D in human serum using liquid chromatography tandem-mass spectrometry with comparison to radioimmunoassay and automated immunoassay. J Chromatogr B Analyt Technol Biomed Life Sci. 2010;878:1163-1168.
Phinney KW. Development of a standard reference material for vitamin D in serum. Am J Clin Nutr. 2008;88:511S-512S.
Singh RJ, Taylor RL, Reddy GS, et al. C-3 epimers can account for a significant proportion of total circulating 25-hydroxyvitamin D in infants, complicating accurate measurement and interpretation of vitamin D status. J Clin Endocrinol Metab. 2006;91:3055-3061.
de la Hunty A, Wallace AM, Gibson S, et al. UK Food Standards Agency Workshop Consensus Report: the choice of method for measuring 25-hydroxyvitamin D to estimate vitamin D status for the UK National Diet and Nutrition Survey. Br J Nutr. 2010;104:612-619.
Yetley EA, Pfeiffer CM, Schleicher RL, et al. NHANES monitoring of serum 25-hydroxyvitamin D: a roundtable summary. J Nutr. 2010;140:2030S-2045S.
Heaney RP. Functional indices of vitamin D status and ramifications of vitamin D deficiency. Am J Clin Nutr. 2004;80(6 suppl):1706S-1709S.
ARUP Laboratories. Vitamin D, 25-hydroxy. ARUP's Laboratory Test Directory Web site. http://www.aruplab.com/ guides/ug/tests/0080379.jsp. Accessed February 1, 2011.
ARUP Laboratories. 25-Hydroxyvitamin D2 and D3 by tandem mass spectrometry, serum. ARUP's Laboratory Test Directory Web site. http://www.aruplab.com/guides/ug/ tests/2002348.jsp. Accessed February 1, 2011.
Mayo Clinic Mayo Medical Laboratories. 25-Hydroxyvitamin D2 and D3, serum. Mayo Medical Laboratories Test Catalog Web site. http://www.mayomedicallaboratories.com/test-catalog/Overview/83670. Accessed February 1, 2011.
Vieth R. Vitamin D supplementation, 25-hydroxyvitamin D concentrations, and safety. Am J Clin Nutr. 1999;69:842-856.
Vieth R, Ladak Y, Walfish PG. Age-related changes in the 25-hydroxyvitamin D versus parathyroid hormone relationship suggest a different reason why older adults require more vitamin D. J Clin Endocrinol Metab. 2003;88:185-191.
LabCorp. Vitamin D, 25-hydroxy. LabCorp Test Menu Web site. Available at https://www.labcorp.com.
LIAISON 25-OH Vitamin D TOTAL [package insert]. Stillwater, MN: DiaSorin; 2007.
Binkley N, Drezner MK, Hollis BW. Laboratory reporting of 25-hydroxyvitamin D results: potential for clinical misinterpretation [letter]. Clin Chem. 2006;52:2124-2125.
Dawson-Hughes B, Heaney RP, Holick MF, et al. Estimates of optimal vitamin D status. Osteoporos Int. 2005;16:713-716.
Souberbielle JC, Fayol V, Sault C, et al. Assay-specific decision limits for two new automated parathyroid hormone and 25-hydroxyvitamin D assays. Clin Chem. 2005;51:395-
400.
25-Hydroxy Vitamin D EIA [package insert]. Fountain Hills, AZ: ImmunoDiagnosticSystems; 2009.
25-Hydroxy Vitamin D RIA [package insert]. Fountain Hills, AZ: ImmunoDiagnosticSystems; 2008.
Quest Diagnostics. Vitamin D, 25-hydroxy, LC/MS/ MS. Quest Diagnostics Test Menu Web site. http://www.questdiagnostics.com/hcp/testmenu/jsp/showTestMenu. jsp?fn=17306.html&labCode;=SJC. Accessed February 1, 2011.
Cullen G. Pesticide poisoning: rodenticides. Emerg Nurse. 2000;8:16-21.
Vieth R. Vitamin D toxicity, policy, and science. J Bone Miner Res. 2007;22(suppl 2):V64-V68.
Kaptein S, Risselada AJ, Boerma EC, et al. Life-threatening complications of vitamin D intoxication due to over-the-counter supplements. Clin Toxicol (Phila). 2010;48:460-462.
Klontz KC, Acheson DW. Dietary supplement-induced vitamin D intoxication [letter]. N Engl J Med. 2007;357:308-309.
Koutkia P, Chen TC, Holick MF. Vitamin D intoxication associated with an over-the-counter supplement [letter]. N Engl J Med. 2001;345:66-67.
Dobnig H, Pilz S, Scharnagl H, et al. Independent association of low serum 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D levels with all-cause and cardiovascular mortality. Arch Intern Med. 2008;168:1340-1349.
Zittermann A, Schleithoff SS, Frisch S, et al. Circulating calcitriol concentrations and total mortality. Clin Chem. 2009;55:1163-1170.
Haug C, Muller F, Aukrust P, et al. Subnormal serum concentration of 1,25-vitamin D in human immunodeficiency virus infection: correlation with degree of immune deficiency and survival. J Infect Dis. 1994;169:889-893.
Wolf M, Shah A, Gutierrez O, et al. Vitamin D levels and early mortality among incident hemodialysis patients. Kidney Int. 2007;72:1004-1013.