A review of the evidence regarding the solar ultraviolet-B-vitamin D-cancer hypothesis
Presented at “Vitamin D — Minimum, maximum, optimum” Warsaw, Poland
William B. Grant, Sunlight, Nutrition, and Health Research Center, San Francisco
A large and growing body of literature addresses how solar ultraviolet-B (UVB) doses and vitamin D reduce the risk of cancer incidence and mortality. This evidence comes from ecological, observational, cross-sectional, and laboratory studies, as well as randomized controlled trials (RCTs). Using the criteria for causality that A. Bradford Hill established, we can evaluate the scientific evidence. The most appropriate criteria for vitamin D and cancer are strength of association, consistency (repeated findings in different populations), biological gradient, plausibility (mechanisms), and experimental verification. Many geography-based ecological studies have reported strong inverse correlations between indices of solar UVB doses and rates of cancer incidence or mortality.
The 13 types of cancer with the strongest evidence - based on number of studies reporting strong inverse correlations - are bladder, female breast, colon, esophageal, gallbladder, gastric, ovarian, pancreatic, prostate, rectal, and renal cancer, as well as lymphoma (Hodgkin's and non-Hodgkin's). Case-control studies of breast and colorectal cancer incidence find pronounced inverse correlations with serum 25-hydroxyvitamin D [25(OH)D] concentrations, with rapid reductions in risk for increases of 25(OH)D concentration at low values and little change above about 100 nmol/l.
Vitamin D reduces the risk of cancer through effects on cellular differentiation and proliferation, epithelial cell binding, metastasis, and angiogenesis around tumors, thus affecting cancer growth at all stages. Experimental verification of the UVB-vitamin D-cancer hypothesis comes from two RCTs, one treatment study, and many "accidental experiments" such as ecological and observational studies.
One RCT found a 77% reduction in all-cancer incidence rates for postmenopausal women taking 1100 IU/d of vitamin D3 plus 1450 mg/d of calcium between the ends of the first and fourth years of the study.
"Accidental experiments" include the findings that (1) those who develop non-melanoma skin cancer may have reduced risk of internal cancers, especially if they live in areas warm enough to expose sufficient body surface area to generate adequate amounts of vitamin D, and (2) that black Americans have lower cancer incidence, survival, and mortality rates, consistent with having about 35% lower serum 25(OH)D concentrations than white Americans.
The available evidence indicates that for optimal cancer risk reduction, serum 25(OH)D concentrations should be above 100 nmol/l and that oral intake without significant vitamin D production from solar UVB irradiance should be 1000-5000 IU/day of vitamin D3.
Introduction
Thirty-two years ago, the brothers Cedric and Frank Garland proposed the ultraviolet-B (UVB)-vitamin D-cancer hypothesis after recognizing an inverse correlation between U.S. colon cancer mortality rates and annual solar radiation doses.1 The hypothesis has support from many ecological,2-5 observational,6 and laboratory studies,7 but from only two randomized controlled trials (RCTs).8,9 The mechanisms whereby vitamin D reduces the risk of cancer are well known.7
As of June 9, 2012, PubMed.gov listed 2774 publications with "vitamin D" and "cancer" in the title or abstract.
Despite the strong scientific support in these studies, health and medicine policy makers have not accepted the hypothesis.10,11 The primary reasons are the limited number of RCTs supporting the hypothesis as well as the conflicting results from observational studies. Although ecological studies strongly support the hypothesis, policy makers generally dismiss them. Both my 2009 report on the International Agency for Research on Cancer Working Group 12 and the 2011 report of Hollis 13 have criticized these reports for bias in selection of studies to include and in interpretation of the findings.
This review summarizes the evidence supporting the UVB-vitamin D-cancer hypothesis and explains studies that have yielded conflicting evidence. I emphasize epidemiological studies and RCTs rather than mechanisms because the mechanisms are generally well documented and accepted, as opposed to the conflicting results from RCTs and ecological or observational studies.
Hill's criteria for causality in a biological system 14 frame this review. The relevant criteria are strength of association, consistency, biological gradient, plausibility (mechanisms), and experimental verification. Previous papers deemed these criteria well satisfied for breast and colorectal cancer, and moderately well satisfied for several other types.15,16
Methods
Representative studies for this review came from searching PubMed.gov for papers that could document the important criteria for causality in a biological system regarding the UVB-vitamin D-cancer hypothesis.
Results
Papers addressing each of the relevant criteria for causality in a biological system follow.
Strength of association
Ecological studies have found highly significant inverse correlations between indices of solar UVB doses and incidence or mortality rates of cancer. In the United States, mortality rates for many types of cancer are highest in the northeast and lowest in the southwest.17 U.S. summertime and annual solar UVB doses are asymmetrical with respect to latitude, with doses generally higher in the western half of the country.18 The western U.S. has higher surface elevation and a thinner ozone layer. Because the inverse correlation between solar UVB doses and cancer mortality rates are readily apparent, one would expect strength of association to be strong.
A U.S. ecological study using cancer mortality rates for approximately 500 state economic areas found significant inverse correlation for 15 types of cancer with solar UVB doses for July 1992.19 That paper presented graphs of solar UVB dose versus mortality rate for several types of cancer. Graphs for female breast and male bladder cancer showed 50% and 80% higher rates, respectively, for low versus high solar UVB doses. Although that study included no other cancer risk-modifying factors, a later study found that the correlation with solar UVB for the 15 types of cancer was largely unaffected when several important cancer risk-modifying factors were added to the model.20 I recently analyzed the evidence for an important role of solar UVB in reducing risk of cancer.5,21
Observational studies also show strong inverse correlations between serum 25(OH)D concentration and both cancer incidence and survival. Case-control studies of breast cancer incidence have yielded the strongest findings.22-26 Figure 1 is a graphical meta-analysis of breast cancer incidence with respect to mean serum 25(OH)D concentrations for quantiles of 25(OH)D for those studies with a power law fit to the data. The odds ratio for breast cancer incidence for concentrations greater than 120 nmol/l is about 30% lower than that for 20 nmol/l. Policy makers sometimes question or dismiss case-control studies because of concern that the disease state would affect serum 25(OH)D concentration.27 However, patients are generally not aware of cancer, especially breast cancer, until diagnosis, so vitamin D from oral intake or UVB irradiance is unlikely to change. Also, no evidence indicates that having cancer affects serum 25(OH)D concentration. That all five sets of data overlap well with the power-law fit to the data supports the contention that prediagnostic cancer did not affect serum 25(OH) D concentrations.
Strong evidence exists for beneficial effects of vitamin D for cancer survival. An indirect indication of a beneficial role of vitamin D is the finding that cancer survival depends on season of diagnosis, with higher survival rates for diagnosis in summer or fall for breast, colon, and prostate cancer as well as Hodgkin's lymphoma.28,29 Other studies have found higher cancer-specific or all-cause survival rates with respect to serum 25(OH)D concentrations for breast cancer,30,31 colorectal cancer,31,32 non-Hodgkin's lymphoma (NHL),31,33 chronic lymphocytic leukemia,34 non-small-cell lung cancer,31,35 and prostate cancer.36 Survival rates were as much as two times higher for high versus low serum 25(OH)D concentrations.31,32
Consistency
Consistency refers to similar findings in different populations. Ecological studies have generally yielded similar findings for cancer incidence or mortality rates with respect to solar UVB doses for many regions: Australia,37 China,38,39 Europe,40,41 Japan,42 the United States,19,20,43 and multiple countries taken together.45,44 The types of cancer with the strongest evidence (based on number of studies reporting strong inverse correlations) were bladder, female breast, colon, esophageal, gallbladder, gastric, ovar -ian, pancreatic, prostate, rectal, and renal cancer, as well as lymphoma (Hodgkin's and non-Hodgkin's).5
A recent study inversely correlated incidence rates of 12 types of cancer with July solar erythemal UV: bladder, colon, kidney, lung, pancreas, pleura, prostate, rectal, thyroid cancer, diffuse large B-cell, T-cell, and NHL.45 Although solar erythemal UV extends to slightly longer wavelengths than UVB, which is associated with vitamin D production, it is nonetheless a good vitamin D production index. That study also found nonsignificant inverse correlations for gallbladder, larynx, small intestine, and stomach cancer as well as follicular lymphoma. Increased risk of lip cancer (nonsignificant) and melanoma and other nonepithelial skin cancer (significant) supported the UV index used. These findings largely support those of many ecological studies.5 Surprisingly, cancers of female organs - breast, ovary, and uterus - did not inversely correlate with the UV index, possibly because women spend less time in the sun than men. Other studies have found significant inverse correlations for solar UVB doses for men but not women, such as an ecological study of cancer mortality rates in California during 1950-1964.46
Personal solar UVB irradiance inversely correlates with incidence of NHL.47 Some studies have associated solar UV with increased risk.
The reason for the increased risk appears to be related to immunosuppression.48
Two sets of observational studies did not inversely correlate serum 25(OH)D concentrations and cancer incidence rates: the Vitamin D Pooling Project of Rarer Cancers and the Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study (ATBC Study) of Finnish men. The Vitamin D Pooling Project of Rarer Cancers found no inverse correlation between prediagnostic serum 25(OH)D concentration and incidence of seven types of cancer: endometrial, kidney, lymphoma, ovarian, pancreatic, and upper gastrointestinal (esophageal and gastric) cancer.49 The mean follow-up time after blood draw was 6.63 years. However, the study included too few cases to detect inverse findings. Because of that limitation, the study found 95% confidence intervals for the highest 25(OH)D quartiles of about 50%. That interval is much larger than the 5%-15% changes found for the highest quantile other than for pancreatic cancer, for which the study did find a significantly increased incidence rate.
To study the effects of alpha-tocopherol and beta-carotene on lung cancer risk, the ATBC Study enrolled men aged 50-69 years who smoked at least five cigarettes per day between 1985 and 1988.50 Many nested case-control studies have used this study's cohort to analyze cancer incidence with respect to serum 25(OH)D concentration at time of enrollment, with follow-up at least until 2005. Results include direct correlations between serum 25(OH) D concentration and incidence of pancreatic cancer.51 Why the pancreatic cancer study found a direct correlation between serum 25(OH)D concentration and incidence of pancreatic cancer is unclear; a similar study in the United States inversely correlated them.52 An ecological study based on solar UVB related to occupation in Nordic countries found a significant inverse correlation between the UVB index and incidence rates for pancreatic cancer. In another paper from the ATBC Study, the 25(OH)D-NHL incidence relation changed from inverse to direct after 7 years of follow up.53
For most other cancers, no significant correlation emerged between serum 25(OH)D concentration and cancer incidence rates. The colorectal cancer study found nonsignificant inverse correlations for serum 25(OH)D concentrations below 25 nmol/l, from 25.0 to less than 37.5 nmol/l, and from 37.5 to 50.0 nmol/l (compared with 50-75.0 nmol/l and >75 nmol/l). Evidently the study had too few cases to find significant inverse correlations. Random changes in serum 25(OH)D concentration over the follow-up period can account for the studies with no significant correlation.54,55
A nested case-control study (from the Health Professionals Follow-Up Study) of males with a 14-year follow-up period found significant inverse correlations with respect to a predicted 25(OH)D concentration for colorectal, esophageal, pancreatic, oral/pharyngeal cancer, and leukemia, and found nonsignificant inverse correlations for bladder, kidney, lung, prostate, stomach cancer, and NHL.56 The predicted 25(OH)D concentration was based on a statistical analysis of serum 25(OH)D concentration with respect to factors related to oral intake and solar UVB production of vitamin D for 1095 men, which were then compared with data from an independent sample of 542 men in the cohort. This study may have succeeded despite the long follow-up time because it used solar UVB doses and recreational time spent outdoors to determine the predicted 25(OH)D concentration.
Two cancers of women, cervical and endometrial cancer, have only modest support in ecological studies. Smoking is an important risk factor for cervical cancer, and separating the effects of smoking from those of UVB irradiance may be difficult. Endometrial cancer mortality rates inversely correlated with solar UVB doses in two U.S. studies.20,43 A third cancer, ovarian cancer, has stronger support,20,44 but not as strong as that for many other types.5 However, an observational study in Finland with a 13-year follow-up pe -riod found a nearly significant inverse correlation between serum 25(OH)D concentration at enrollment and ovarian cancer incidence, as well as a significant inverse correlation with serum calcium concentration.57
Weaker evidence exists for nine other types of cancer: brain, laryngeal, lung, oral/pharyngeal, and thyroid cancer; leukemia; melanoma; and multiple myeloma.5 One reason for weaker evidence is that, for cancers with low mortality rates, the number of cases in each geographical unit is small, increasing the uncertainty of the determination. An U.S. ecological study using approximately 500 state economic areas showed that when the mortality rate during 1950-1969 was less than 8 deaths/100,000/year, the adjusted R2 value of the regression analysis (including four risk-modifying factors: UVB doses, lung cancer mortality rates, alcohol consumption, and urban residence) was often clustered between 0.05 and 0.30. However, for several types of cancer, values were between 0.53 and 0.72, largely because of the association with smoking; for adjusted R2 greater than 8 deaths/100,000/year, the values were between 0.33 and 0.76.58 However, weaker evidence could also mean that vitamin D has little impact on risk of these cancers.
Lung cancer is relatively difficult to study with the eco -logical approach because finding suitable indices for smoking is a challenge; studies often use lung cancer rates as the index of the adverse effects of smoking.20 However, a multicountry study used cigarette consumption by country, finding a significant inverse correlation of lung cancer with solar UVB doses.59
In 2009, Pukkala and colleagues conducted an ecological study based on cancer incidence rates for 54 occupations in the five Nordic countries.60 The solar UVB index they developed was the standardized incidence ratio for lip cancer less that for lung cancer for men because both UV irradiance and smoking are risk factors for lip cancer. Many women wear lipstick, so the researchers could not develop this index separately for women.
For men, the UVB index significantly inversely correlated with
14 types of internal cancers: bladder, breast, colon, gallbladder, kidney, laryngeal, liver, lung, oral, pancreatic, pharyngeal, prostate, rectal, and small intestine .
For women, the same UVB index inversely correlated with bladder, breast, colon, and rectal cancer .61
However, observational studies do not always agree with ecological studies or with each other. Observational studies are of two general types: case-control and nested case-control studies derived from cohort studies. In case-control studies, serum 25(OH)D concentrations are measured at time of diagnosis. In cohort studies, serum 25(OH) D concentrations are measured in blood drawn at time of enrollment. Controls are matched with cases in a nested case-control study from the cohort study. Case-control studies found strong inverse correlations between serum 25(OH)D concentrations and breast cancer incidence. 22-26 Case-control studies are considered inferior to prospective observational studies because the disease state may affect the risk-modifying factors.
No nested case-control study with follow-up time greater than 3 years has found a significant inverse correlation between prediagnostic serum 25(OH)D concentration and breast cancer incidence.54 For both breast and colorectal cancer, the beneficial effect of prediagnostic serum 25(OH) D concentration decreased with longer follow-up time. The regression fit to the data for relative risk (RR) for the studies went from 0.6 at zero years to 0.95 at 7 years. However, for colorectal cancer, significant inverse correlations emerged for follow-up times out to 12 years, although the regression fit went from an RR of 0.4 at 5 years to 0.7 at 14 years. The changes in RR were 0.05/year for breast cancer and 0.033/ year for colorectal cancer. In an analysis of ovarian cancer incidence versus prediagnostic serum 25(OH)D for the four studies in Yin (ovarian),62 which included enough cases that the upper 95% confidence interval (CI) value was below 2.0, the slope was 0.047/year. In a Norway study, the regression coefficient for samples drawn 14 years apart dropped to 0.42,63 falling by 0.04/year. Thus, the three values for cancer agree with what one could expect from the changes of 25(OH)D concentrations with increasing follow-up time. However, the change of cancer RR with time could also reflect the time it takes to go from cancer initiation to detection.
Policy makers generally point to three findings as evidence for inconsistency between observational studies and ecological studies regarding the UVB-vitamin D-cancer hypothesis: the U-shaped relation for prostate cancer,64 the direct correlation between prediagnostic serum 25(OH)D and pancreatic cancer incidence rates in Finland,51 and the failure to find any inverse correlation for seven rarer types of cancer in the Vitamin D Pooling Project.49
Tuohimaa and colleagues reported a U-shaped relation between serum 25(OH)D concentration and prostate cancer incidence.64 Meta-analyses of prostate cancer incidence find essentially no correlation with prediagnostic serum 25(OH)D concentration.6,27 Marshall and colleagues reported that when men biopsy-diagnosed with low-grade prostate cancer took 4000 IU/d of vitamin D3 for 1 year, 55% had biopsy-determined regressions in the number of tumors, compared with 20% in historical control subjects not taking 4000 IU/d.65 Thus, the Tuohimaa study is anomalous. Ideas on why the finding was made include the possibility that dietary sources of vitamin D in Nordic countries may also increase the risk of prostate cancer.
Disagreement exists regarding prediagnostic serum 25(OH)D concentration and incidence of pancreatic cancer. As discussed earlier, a study in Finland found a direct correlation between prediagnostic serum 25(OH)D concentration 51 but a Harvard study involving five cohorts with a 20-year follow-up period did find a significant inverse correlation between predicted 25(OH)D concentrations and incidence of pancreatic cancer.52 Ecological studies generally find inverse correlations between solar UVB doses and pancreatic cancer rates.5
Biological gradient
Ecological studies often find inverse correlations between solar UVB indices and cancer incidence or mortality rates,5,20 and observational studies find inverse correlations between serum 25(OH)D concentrations and cancer incidence.6 The shape of the relation is nonlinear (Figure 1).
Case-control studies offer the strongest observational support for an inverse correlation between serum 25(OH)D concentration and cancer incidence for breast and colorectal cancer.54 A major problem with cohort studies is the long follow-up time after blood draw for measurement of 25(OH)D concentration, during which serum 25(OH)D concentrations vary.54,55 Two U.S. studies of frailty show how serum 25(OH)D concentrations evidently change: men experienced a monotonic decrease in frailty status with increasing serum 25(OH)D concentration,66 whereas for women, a U-shaped relation emerged, with higher frailty status for both low and high serum 25(OH)D concentrations.67 Women are much more likely than men to be diagnosed with osteoporosis in the United States.
Plausibility (mechanisms)
The mechanisms by which vitamin D reduces risk of cancer incidence and increases survival after cancer develops are reasonably well understood. The mechanisms can be grouped as genomic and nongenomic. Genomic mechanisms operate through effects of 1,25-dihydroxyvitamin D [1,25(OH)2D] on gene expression: "By regulating the expression of many genes via several mechanisms, 1,25(OH) 2D3 induces differentiation, controls the detoxification metabolism and cell phenotype, sensitizes cells to apoptosis, and inhibits the proliferation of cultured human colon carcinoma cells".68 Related to this effect is that most organs can convert circulating 25(OH)D to 1,25(OH)2D by virtue of having 25-hydroxyvitamin D(3)-1a-hydroxylase activity.69
Vuolo and colleagues 7 reviewed nongenomic effects, including transport of calcium and activation of "second messenger systems including phospholipase C (PKC), protein kinase C, G protein-coupled receptors, or phosphati-dylinositol-3-kinase (PI3K)." The effects include regulation of cell growth and differentiation and apoptosis.
Garland and colleagues proposed a model for how vitamin D reduces the risk of cancer through strengthening the epithelium: "Its seven phases are disjunction, initiation, natural selection, overgrowth, metastasis, involution, and transition (abbreviated DINOMIT)".70 The basic idea is that vitamin D keeps the cells in the epithelial layer of organs in tight junction. When vitamin D concentrations are low, E-cadherins are downregulated and the cells can start to separate. DNA errors are thus not corrected as well as when vitamin D concentrations are optimal, and cancer growth begins. The discussion then continues through a variety of steps for cancer progression, each of which vitamin D could hinder.
The role of vitamin D in reducing metastasis and an-giogenesis around tumors is also well documented,71 which helps explain why cancer survival rates are higher for those with higher serum 25(OH)D concentrations at time of diagnosis.
Experimental confirmation
Two RCTs have shown that vitamin D reduces the risk of cancer. The first used 1100 IU/d of vitamin D3 and 1450 mg/d of calcium with a group of postmenopausal Nebraska women.8 Mean serum 25(OH)D concentrations for those taking vitamin D plus calcium rose from 72 to 96 nmol/l. The RR between the ends of the first and fourth years for the group taking calcium plus vitamin D was 0.23 (95% CI, 0.09-0.60; p < 0.005), whereas that for calcium alone was 0.59 (95% CI, 0.29-1.21; p = 0.15). Because calcium's effect was not statistically significant, the authors stated that the effect of vitamin D was significant. However, the combination of vitamin D and calcium may have yielded the result observed, because calcium can reduce risk of cancer.72 This study has been criticized on the basis of its cases not having cancer incidence rates as high as expected. However, a comparison of cancer incidence rates for women of that age living in Nebraska finds that those rates were very close to the expected rates.

- Odds ratio
03-Breast cancer 25(OH)D
20 40 60 80 100 120 140 160 25(OH)D (nmol/l) case-control
FIG. 1.
Scatterplot of the odds ratio for breast cancer incidence versus serum 25(OH)D concentration at time of diagnosis, using data from five case-control studies.22-26
The equation for the fit is odds ratio = 10 [25(OH)D]-0.68 (r = 0.92).
The second successful RCT was a reanalysis of the Women's Health Initiative vitamin D and calcium study. The original analysis for those taking vitamin D found no significant effect on risk of cancer after 7 years of supplementation.73 However, compliance was poor, so the effective supplementation was only about 280 IU/d. The reanalysis examined results only for those not taking calcium or vitamin D supplements before enrollment. Taking calcium plus vitamin D "significantly decreased the risk of total, breast, and invasive breast cancers by 14-20% and nonsignificantly reduced the risk of colorectal cancer by 17%. In women taking personal calcium or vitamin D supplements, CaD did not alter cancer risk (HR: 1.06-1.26)".9 An RCT conducted with Japanese schoolchildren found higher inverse correlation between vitamin D supplementation and incidence of type A influenza for those not taking other vitamin D than for those taking vitamin D.74
The idea that the effect of vitamin D on risk of disease should be tested with the same approach as pharmaceutical drugs seems to be a construct of the medical system. Vitamin D is a natural compound derived from solar UVB and is so important that skin pigmentation changed as humans left the African plains for higher latitudes.75 Thus, considering whether alternative experiments could test the UVB-vitamin D-cancer hypothesis is worthwhile. One approach is to make predictions based on basic understandings of vitamin D and then to see whether the data accord.
One possible experiment is observational studies on survival after diagnosis of cancer with respect to serum 25(OH)D concentrations. Several studies have found higher cancer-specific survival rates for seven types of cancer.28-36 These findings led to the hypothesis that serum 25(OH)D concentration differences can account for racial disparities in U.S. cancer survival rates that socioeconomic status, stage at diagnosis, or treatment cannot explain. Black Americans have 35% lower 25(OH)D concentrations than white Americans and have about 15% lower cancer survival rates averaged for 13 types of cancer.76
Another prediction is that people with higher rates of nonmelanoma skin cancer (NMSC) will have lower rates of vitamin D-sensitive cancers. Integrated lifetime UVB irradiance is the most important risk factor for squamous cell carcinoma, which accounts for most NMSC deaths. UV irradiance is the most important risk factor for basal cell carcinoma, which accounts for most NMSC cases. A meta-analysis found several cancers for which incidence rates of second cancers were reduced after diagnosis of basal cell carcinoma or squamous cell carcinoma.77 Moreover, in a record-linkage study, Tuohimaa and colleagues inversely correlated diagnosis of NMSC in sunny countries - where it is warm enough that people can expose sufficient body surface area when in the sun to generate enough vitamin D to reduce the risk of cancer - with incidence of several types of cancer.78 An ecological study in California found significant inverse correlations with NMSC mortality rate in multiple linear regression analyses of the period 1950-1964 for eight types of cancer for males: bladder, brain, colon, gastric, prostate, and rectal cancer; multiple myeloma; and NHL.46 That was a time when people were not concerned about the risk of skin cancer. After that period, NMSC no longer inversely correlated with internal cancers. An ecological study in Spain inversely correlated mortality rates for 17 types of cancer with NMSC mortality rates.41
A third prediction is that black Americans will have higher rates of cancer and poorer survival rates than white Americans. For black Americans, cancer rates are 40% higher for males and 17% higher for females.17 Black Americans also have mortality rates about 25% higher after diagnosis of cancer than white Americans after consideration of socioeconomic status, stage at diagnosis, and treatment. Black Americans have mean serum 25(OH)D concentrations of 40 nmol/l, whereas white Americans have concentrations of about 65 nmol/l.79 On the basis of serum 25(OH)D concentration - cancer incidence rates for breast and colorectal cancer,6 black Americans would have 25% higher cancer rates, similar to the rates found.76
Confounding factors
Most ecological and observational studies include several cancer risk-modifying factors in the model development and analysis. For example, an ecological study of U.S. cancer mortality rates included indices for alcohol consumption, ethnic background (Hispanic Americans are counted as white Americans), smoking, socioeconomic status, and urban/rural residence in addition to July UVB doses.20 Little change was present in the finding for solar UVB compared with when only solar UVB doses were used in a previous study.19
Of possible concern is that the solar UVB index used in many ecological studies is assumed to be an index of vitamin D production. Although using sunlight to reduce the risk of cancer may confer other benefits, such as encouraging more physical activity when it is warm and sunny, ecological studies have proposed no mechanisms other than vitamin D production.
Discussion
The UVB-vitamin D-cancer hypothesis has strong scientific support when the totality of evidence is reviewed. The ecological studies have consistently offered very strong support.5 Case-control studies provide strong evidence for a beneficial effect of vitamin D in reducing risk of breast cancer incidence, especially in light of ecological and laboratory studies. Nested case-control studies also strongly support the hypothesis for breast, colorectal, and ovarian cancer - provided that the studies consider the change of serum 25(OH)D concentration with respect to follow-up time.41 Experimental verification includes positive results from two RCTs,8,9 one treatment study,65 and predictions regarding cancer survival with respect to serum 25(OH) D concentrations at the time of diagnosis - and probably the disparity in cancer survival between black and white Americans after consideration of socioeconomic status, stage at diagnosis, and treatment.76 Table 1 shows how vitamin D as a risk-reduction factor for cancer satisfies Hill's criteria.
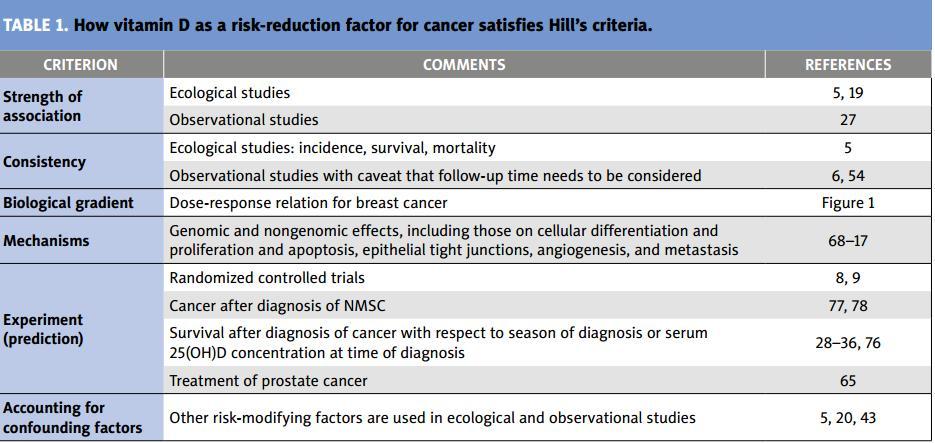
TABLE 1. How vitamin D as a risk-reduction factor for cancer satisfies Hill's criteria.
Strength of association
Ecological studies 5, 19
Observational studies 27
Consistency
Ecological studies: incidence, survival, mortality. 5
Observational studies with caveat that follow-up time needs to be considered, 6, 54
Biological gradient
Dose-response relation for breast cancer. Figure 1
Mechanisms
Genomic and nongenomic effects, including those on cellular differentiation and proliferation and apoptosis, epithelial tight junctions, angiogenesis, and metastasis
68-17
Randomized controlled trials 8, 9
Experiment (prediction)
Cancer after diagnosis of NMSC 77, 78
Survival after diagnosis of cancer with respect to season of diagnosis or serum 25(OH)D concentration at time of diagnosis 28-36, 76
Treatment of prostate cancer 65
Accounting for confounding factors
Other risk-modifying factors are used in ecological and observational studies 5, 20, 43
From the evidence available, it appears that the optimal serum 25(OH)D concentration for cancer risk reduction is above 100 nmol/l. This value is similar to that found for cardiovascular disease and respiratory infections.80 Oral intake without significant vitamin D production from solar UVB irradiance should be 1000-5000 IU/day of vitamin D3. Because 25(OH)D concentrations vary from person to person with respect to oral vitamin D intake,81 measurement of serum 25(OH)D concentrations might be advisable.
Conclusion
On the basis of ecological, observational, and laboratory studies; two RCTs; and one treatment study, strong scientific evidence exists that solar UVB irradiance and vitamin D reduce the risk of many types of cancer. Optimal serum 25(OH)D concentrations for cancer risk reduction are above 100 nmol/l. However, more RCTs are required to convince health policy makers that vitamin D reduces cancer risk. Unfortunately, RCTs with vitamin D have often been conducted improperly and are difficult given the many sources of vitamin D and the fact that serum 25(OH)D concentrations are not often included in the trial design or measured after enrollment.82 Ideally, researchers will incorporate Lappe and Heaney's suggestions for vitamin D RCTs in progress or planned. ?
William B. Grant, Ph.D.
Sunlight, Nutrition, and Health Research Center P.O. Box 641603
San Francisco, CA 94164-1603, USA, [ wbgrant@infionline.net]
Disclosure
I receive funding from the UV Foundation (McLean, VA), Bio-Tech Pharmacal (Fayetteville, AR), the Vitamin D Council (San Luis Obispo, CA), the Vitamin D Society (Canada), and the Sunlight Research Forum (Veldhoven).
References
1 Garland CF, Garland FC. Do sunlight and vitamin D reduce the likelihood of colon cancer? Int J Epidemiol. 1980;9:227-231.
2 Garland CF, Mohr SB, Gorham ED i wsp. Role of ultraviolet-B irradiance and vitamin D in the prevention of ovarian cancer. Am J Prev Med. 2006;31:512-514.
3 Mohr SB. A brief history of vitamin D and cancer prevention. Ann Epidemiol. 2009;19:79-83.
4 Grant WB, Mohr SB. Ecological studies of ultraviolet B, vitamin D and cancer since 2000. Ann Epidemiol. 2009;19:446-454.
5 Grant WB. Ecological studies of the UVB-vitamin D-cancer hypothesis; review. Anticancer Res. 2012;32:223-236.
6 Grant WB. Relation between prediagnostic serum 25-hydroxyvitamin D level and incidence of breast, colorectal, and other cancers. J Photochem Photobiol B. 2010;101:130-136.
7 Vuolo L, Di Somma C, Faggiano A i wsp. Vitamin D and cancer. Front Endocrinol (Lausanne). 2012;3:58.
8 Lappe JM, Travers-Gustafson D, Davies KM i wsp. Vitamin D and calcium supplementation reduces cancer risk: results of a randomized trial. Am J Clin Nutr. 2007;85:1586-1591.
9 Bolland MJ, Grey A, Gamble GD i wsp. Calcium and vitamin D supplements and health outcomes: a reanalysis of the Women's Health Initiative (WHI) limited-access data set. Am J Clin Nutr. 2011;94:1144-1149.
10 IARC Working Group Report 5: Vitamin D and Cancer. IARC, Lyon, France. 2008.
11 Ross AC, Manson JE, Abrams SA i wsp. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J Clin Endocrinol Metab. 2011;96:53-58.
12 Grant WB. A critical review of Vitamin D and Cancer: A report of the IARC Working Group on vitamin D. Dermatoendocrinol. 2009;1:25-33.
13 Hollis BW. Short-term and long-term consequences and concerns regarding valid assessment of vitamin D deficiency: comparison of recent food supplementation and clinical guidance reports. Curr Opin Clin Nutr Metab Care. 2011;14:598-604.
14 Hill AB. The environment and disease: Association or causation? Proc R Soc Med. 1965 ;58:29-300.
15 Grant WB. How strong is the evidence that solar ultraviolet B and vitamin D reduce the risk of cancer? An examination using Hill's criteria for causality. Dermatoendocrinol. 2009;1:17-24.
16 Mohr SB, Gorham ED, Alczraz JE i wsp. Does the evidence for an inverse relationship between serum vitamin D status and breast cancer risk satisfy the Hill criteria? Dermatoendocrinol. 2012;4(2) epub
17 Devesa SS, Grauman DJ, Blot WJ i wsp. Atlas of Cancer Mortality in the United States, 1950-1994. NIH Publication No. 1999;99-4564
18 Fioletov VE, McArthur LJ, Mathews TW i wsp. Estimated ultraviolet exposure levels for a sufficient vitamin D status in North America. J Photochem Photobiol B.
2010;100:57-66.
19 Grant WB. An estimate of premature cancer mortality in the U.S. due to inadequate doses of solar ultraviolet-B radiation. Cancer 2002;94:1867-1875.
20 Grant WB, Garland CF. The association of solar ultraviolet B (UVB) with reducing risk of cancer: multifactorial ecologic analysis of geographic variation in age-adjusted cancer mortality rates. Anticancer Res. 2006;26:2687-2699.
21 Grant WB. Update on evidence that support a role of solar ultraviolet-B irradiance in reducing cancer risk. Anti-Cancer Agents in Medical Chemistry, in press.
22 Lowe LC, Guy M, Mansi JL i wsp. Plasma 25-hydroxy vitamin D concentrations, vitamin D receptor genotype and breast cancer risk in a UK Caucasian population. Eur J Cancer. 2005;41:1164-1169.
23 Abbas S, Linseisen J, Slanger T i wsp. Serum 25-hydroxyvitamin D and risk of postmenopausal breast cancer - results of a large case-control study. Carcinogenesis. 2008;29:93-99.
24 Abbas S, Chang-Claude J, Linseisen J. Plasma 25-hydroxyvitamin D and premenopausal breast cancer risk in a German case-control study. Int J Cancer. 2009;124:250-255.
25 Crew KD, Gammon MD, Steck SE i wsp. Association between plasma 25-hydroxyvitamin D and breast cancer risk. Cancer PrevRes (Phila Pa). 2009;2:598-604.
26 Fedirko V, Torres-Mejia G, Ortega-Olvera C i wsp. Serum 25-hydroxyvitamin D and risk of breast cancer: results of a large population-based case-control study in Mexican women. Cancer Causes Control. 2012;23:1149-1162.
27 Gandini S, Boniol M, Haukka J i wsp. Meta-analysis of observational studies of serum 25-hydroxyvitamin D levels and colorectal, breast and prostate cancer and colorectal adenoma. Int J Cancer. 2011;128:1414-1424.
28 Robsahm TE, Tretli S, Dahlback A i wsp. Vitamin D3 from sunlight may improve the prognosis of breast-, colon- and prostate cancer (Norway). Cancer Causes Control. 2004;15:149-158.
29 Porojnicu AC, Dahlback A, Moan J. Sun exposure and cancer survival in Norway: changes in the risk of death with season of diagnosis and latitude. Adv Exp Med Biol. 2008;624:43-54.
30 Kim HJ, Lee YM, Ko BS i wsp. Vitamin D deficiency is correlated with poor outcomes in patients with luminal-type breast cancer. Ann Surg Oncol. 2011;18:1830-1836.
31 Tretli S, Schwartz GG, Torjesen PA i wsp. Serum levels of 25-hydroxyvitamin D and survival in Norwegian patients with cancer of breast, colon, lung, and lymphoma: a population-based study. Cancer Causes Control. 2012;23:363-370.
32 Ng K, Wolpin BM, Meyerhardt JA i wsp. Prospective study of predictors of vitamin D status and survival in patients with colorectal cancer. Br J Cancer. 2009;101:916-923.
33 Drake MT, Maurer MJ, Link BK i wsp. Vitamin D insufficiency and prognosis in non-Hodgkin's lymphoma. J Clin Oncol. 2010;28:4191-4198.
34 Shanafelt TD, Drake MT, Maurer MJ i wsp. Vitamin D insufficiency and prognosis in chronic lymphocytic leukemia (CLL). Blood. 2011;117:1492-1498.
35 Heist RS, Zhou W, Wang Z i wsp. Circulating 25-hydroxyvitamin D, VDR polymorphisms, and survival in advanced non-small-cell lung cancer. J Clin Oncol. 2008;26:5596-5602.
36 Fang F, Kasperzyk JL, Shui I i wsp. Prediagnostic Plasma Vitamin D metabolites and mortality among patients with prostate cancer. PLoS One. 2011;6:e18625.
37 Astbury A. Non uniformity in cancer mortality in the USA and Australia appears to share a common pathway. Triumf report, TRI-PP-05-01, 2005.
38 Grant WB. Does solar ultraviolet irradiation affect cancer mortality rates in China? Asian Pac J Cancer Prev. 2007;8:236-242.
39 Chen W, Clements M, Rahman B i wsp. Relationship between cancer mortality/ incidence and ambient ultraviolet B irradiance in China. Cancer Causes Control. 2010;21:1701-1709.
40 Grant WB. An ecologic study of cancer mortality rates in Spain with respect to indices of solar UV irradiance and smoking. Int J Cancer. 2007;120:1123-1127.
41 Grant WB. An ecological study of cancer incidence and mortality rates in France with respect to latitude, an index for vitamin D production. Dermatoendocrinol. 2010;2:62-67.
42 Mizoue T. Ecological study of solar radiation and cancer mortality in Japan. Health Phys. 2004;87:532-538.
43 Boscoe FP, Schymura MJ. Solar ultraviolet-B exposure and cancer incidence and mortality in the United States, 1993-2000. BMC Cancer. 2006;6:264.
44 Garland CF, Mohr SB, Gorham ED i wsp. Role of ultraviolet-B irradiance and vitamin D in the prevention of ovarian cancer. Am J Prev Med. 2006;31:512-514.
45 Lin SW, Wheeler DC, Park Y i wsp. Prospective study of ultraviolet radiation exposure and risk of cancer in the U.S. Int J Cancer. 2012 Apr 26. doi:10.1002/ ijc.27619. [Epub ahead of print]
46 Grant WB. An ecological study of cancer mortality rates in California, 1950-64, with respect to solar UVB and smoking indices. Dermatoendocrinol. 2012;4(2) epub
47 Kricker A, Armstrong BK, Hughes AM i wsp. Personal sun exposure and risk of non Hodgkin lymphoma: A pooled analysis from the Interlymph Consortium. Int J Cancer. 2008;122:144-154.
48 Grant WB. Ultraviolet exposure and non-Hodgkin's lymphoma: beneficial and adverse effects? Cancer, Causes Control. 2012;23:653-655.
49 Helzlsouer KJ. For the VDPP Steering Committee. Overview of the Cohort Consortium Vitamin D Pooling Project of Rarer Cancers. Am J Epi. 2010;172:4-9.
50 The ATBC Cancer Prevention Study Group. The Alpha-Tocopherol, Beta-Carotene Lung Cancer Prevention Study: design, methods, participant characteristics, and compliance. Ann Epidemiol. 1994;4:1-10.
51 Stolzenberg-Solomon RZ, Vieth R, Azad A i wsp. A prospective nested case-control study of vitamin D status and pancreatic cancer risk in male smokers. Cancer Res.
2006;66:10213-10219.
52 Wolpin BM, Ng K, Bao Y i wsp. Plasma 25-hydroxyvitamin D and risk of pancreatic cancer. Cancer Epidemiol Biomarkers Prev. 2012;21:82-91.
53 Lim U, Freedman DM, Hollis BW i wsp. A prospective investigation of serum 25-hydroxyvitamin D and risk of lymphoid cancers. Int J Cancer. 2009;124:979-986.
54 Grant WB. Effect of interval between serum draw and follow-up period on relative risk of cancer incidence with respect to 25-hydroxyvitamin D level; implications for meta-analyses and setting vitamin D guidelines. Dermatoendocrinol. 2011;3:199-204.
55 Grant WB. Effect of follow-up time on the relation between prediagnostic serum 25-hydroxyitamin D and all-cause mortality rate. Dermatoendocrinol. 2012;4(2) epub
56 Giovannucci E, Liu Y, Rimm EB i wsp. Prospective study of predictors of vitamin D status and cancer incidence and mortality in men. JNCI. 2006;98:451-459.
57 Toriola AT, Surcel HM, Calypse A i wsp. Independent and joint effects of serum 25-hydroxyvitamin D and calcium on ovarian cancer risk: A prospective nested case-control study. Eur J Cancer. 2010;46:2799-2805.
58 Grant WB. An ecological study of cancer mortality rates in the United States with respect to solar ultraviolet-B doses, smoking, alcohol consumption, and urban/ rural residence. Dermatoendocrinol. 2010;2:68-76.
59 Mohr SB, Garland CF, Gorham ED i wsp. Could ultraviolet B irradiance and vitamin D be associated with lower incidence rates of lung cancer? J Epidemiol Community Health. 2008;62:69-74.
60 Pukkala E, Martinsen JI, Lynge E i wsp. Occupation and cancer - follow-up of 15 million people in five Nordic countries. Acta Oncol 2009;48:646-790.
61 Grant WB. Role of solar UV irradiance and smoking in cancer as inferred from cancer incidence rates by occupation in Nordic countries. Dermatoendocrinol. 2012;4(2) epub.
62 Yin L, Grandi N, Raum E i wsp. Meta-analysis: Circulating vitamin D and ovarian cancer risk. Gynecol Oncol. 2011;121:369-375.
63 Jorde R, Sneve M, Hutchinson M i wsp. Tracking of serum 25-hydroxyvitamin D levels during 14 years in a population-based study and during 12 months in an intervention study. Am J Epidemiol. 2010;171:903-908.
64 Tuohimaa P, Tenkanen L, Ahonen M i wsp. Both high and low levels of blood vitamin D are associated with a higher prostate cancer risk: a longitudinal, nested case-control study in the Nordic countries. Int J Cancer. 2004;108:104-108.
65 Marshall DE, Savage SJ, Garrett-Mayer E i wsp. Vitamin D3 supplementation at 4000 international units per day for one year results in a decrease of positive cores at repeat biopsy in subjects with low-risk prostate cancer under active surveillance. J Clin Endocrinol Metab. 2012 jc.2012-1451 epub.
66 Ensrud KE, Blackwell TL, Cauley JA I wsp. Circulating 25-hydroxyvitamin D levels and frailty in older men: the osteoporotic fractures in men study. J Am Geriatr Soc. 2011;59:101-106.
67 Ensrud KE, Ewing SK, Fredman L i wsp. Circulating 25-hydroxyvitamin D levels and frailty status in older women. J Clin Endocrinol Metab. 2010;95:5266-5273.
68 Pereira F, Larriba MJ, Muhoz A. Vitamin D and colon cancer. Endocr Relat Cancer. 2012 Mar 1. [Epub ahead of print]
69 Cross HS, Bareis P, Hofer H i wsp. 25-Hydroxyvitamin D(3)-1alpha-hydroxylase and vitamin D receptor gene expression in human colonic mucosa is elevated during early cancerogenesis. Steroids. 2001;66:287-292.
70 Garland CF, Gorham ED, Mohr SB i wsp. Vitamin D for cancer prevention: Global perspective. Ann Epi. 2009;19:468-483.
71 Krishnan AV, Trump DL, Johnson CS i wsp. The role of vitamin D in cancer prevention and treatment. Rheum Dis Clin North Am. 2012;38:161-178.
72 Peterlik M, Grant WB, Cross HS. Calcium, vitamin D and cancer. Anticancer Res. 2009;29:3687-3698.
73 Wactawski-Wende J, Kotchen JM, Anderson GL i wsp. Calcium plus vitamin D supplementation and the risk of colorectal cancer. N Engl J Med. 2006;354:684-696.
74 Urashima M, Segawa T, Okazaki M i wsp. Randomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildren. Am J Clin Nutr. 2010;91:1255-1260.
75 Jablonski NG. The evolution of human skin colouration and its relevance to health in the modern world. J R Coll Physicians Edinb. 2012;42:58-63.
76 Grant WB, Peiris AN. Differences in vitamin D status may account for unexplained disparities in cancer survival rates between African and White Americans. Dermatoendocrinol. 2012;4(2) epub
77 Grant WB. A meta-analysis of second cancers after a diagnosis of nonmelanoma skin cancer: additional evidence that solar ultraviolet-B irradiance reduces the risk of internal cancers. J Steroid Biochem Mol. 2007;103:668-674.
78 Tuohimaa P, Pukkala E, Scelo G i wsp. Does solar exposure, as indicated by the non-melanoma skin cancers, protect from solid cancers: Vitamin D as a possible explanation. Eur J Cancer. 2007;43:1701-1712.
79 Ginde AA, Liu MC, Camargo CA Jr. Demographic differences and trends of vitamin D insufficiency in the US population, 1988-2004. Arch Intern Med. 2009;169:626-632.
80 Grant WB. An estimate of the global reduction in mortality rates through doubling vitamin D levels. Eur J Clin Nutr. 2011;65:1016-1026.
81 Garland CF, French CB, Baggerly LL, Heaney RP. Vitamin D supplement doses and serum 25-hydroxyvitamin D in the range associated with cancer prevention. Anticancer Res. 2011;31:617-622.
82 Lappe JM, Heaney RP. Why randomized controlled trials of calcium and vitamin D sometimes fail. Dermatoendocrinol. 2012;4(2) epub.
See also VitaminDWiki
Too much UVB: skin cancer, too little UVB: other cancers due to low vitamin D – April 2012
More UVB is associated with less cancer – study of 450,000 people – April 2012
Review of possible ways that vitamin D fights cancer – Jan 2012
Mechanisms of the Anti-Cancer and Anti-Inflammatory - 2011.PDF
Cancers and Vitamin D Council and Dr. Grant (same author)
Vitamin D and Cancer Treatment and Prevention – presentations May 2011
China has documented that less UV results in more cancer – June 2010 - esophagus, stomach, colon and rectum, liver, lung, breast, and bladder
Brain cancer in 175 countries related to low UVB and low vitamin D – Oct 2010
- Stronger correlation for women than for men
Cloudiness and Breast Cancer PDF file
Breast Cancer vs latitude Gapminder - Great U shaped curve
Need lots of UV AND vitamin D to reduce risk of breast cancer – Jan 2011
Low UVB (thus low Vitamin D) is linked to many diseases – Grant Jan 2016