Vitamin D and multiple sclerosis (technical, outline only)
Journal of Clinical Neuroscience; Available online 26 March 2013
Sarah Hewer a,
Robyn Lucas b,
Ingrid van der Mei c,
Bruce V. Taylor c, bruce.taylor@utas.edu.au
a Royal Hobart Hospital, Department of Neurology, Hobart, Tasmania, Australia
b National Centre for Epidemiology and Population Health, The Australian National University, Canberra, Australian Capital Territory, Australia
c Menzies Research Institute Tasmania, University of Tasmania, Locked Bag 23, Hobart, Tasmania 7000, Australia
The role of vitamin D supplementation in preventing multiple sclerosis (MS) and/or treating MS progression is an area of significant research interest. We detail the current status of the ongoing research in this field, and note the lack of class 1 evidence from well-conducted, large, double-blind, placebo-controlled studies of vitamin D supplementation in the prevention and/or treatment of MS. We have been able to provide some guidelines for practitioners based on the substantial burden of supportive evidence for the use of vitamin D in MS as summarised here. These guidelines may provide some support to those clinicians who treat people with MS and their families.
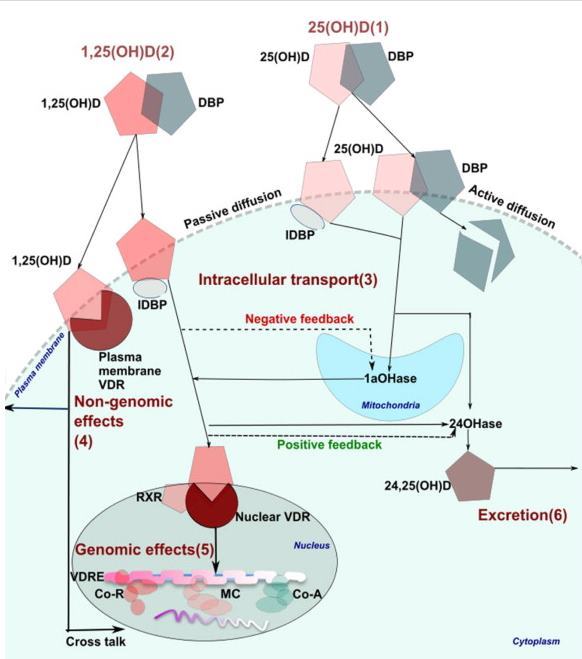
Fig. 1.
Cellular pathways of 25-hydroxyvitamin D (25(OH)D) and 1,25-dihydroxyvitamin D (1,25(OH)2D) in cell and gene regulation (after Simpson Greenhill 2011100).
(1) The 25(OH)D and 1,25(OH)2D are predominantly transported in plasma bound to vitamin D binding protein (VDBP). A small proportion (0.04% of 25(OH)D and 0.4% of 1,25(OH)2D) are transported unbound in the plasma and this fraction has traditionally been assumed to enter cells via passive diffusion. VDBP-bound 25(OH)D is now recognized to be internalized via receptor-mediated membrane transport.
(2) Once in the cell, 25(OH)D is transported to the mitochondria where it undergoes hydroxylation to 1,25(OH)2D; 1,25(OH)2D can also enter the cell directly.
(3) The movement of 25(OH)D and 1,25(OH)2D from the cell membrane to their intracellular destinations is a highly ordered process involving a chain of intracellular vitamin D binding proteins (IDBP).
(4) Non-genomic effects occur on binding of 1,25(OH)2D to the cell membrane vitamin D receptor (VDR) and take place at the plasma membrane and in the cytoplasm.
(5) Genomic effects of 1,25(OH)2D primarily occur within the cell nucleus. The VDR forms a heterodimer with retinoid X receptor (RXR), and this complex preferentially binds 1,25(OH)2D. The resulting complex binds vitamin D response element (VDRE) on target genes, resulting in dissociation of corepressor (CoR) protein and recruitment of coactivator (CoA) proteins. The VDR–CoA interaction facilitates recruitment of mediator complexes (MC) that build a bridge between the VDRE and the transcription machinery to affect expression of multiple genes.
(6) The 25(OH) D and 1,25(OH)2D are catabolized by the enzyme vitamin D-24-hydroxylase (24OHase) to the inactive, water-soluble form 24,25-dihydroxycholecalciferol (24,25(OH)2D) for renal excretion.
Reproduced with permission from Remedica Medical Education and Publishing.
Rest of the article is behind a paywall
Outline of the paper
- Introduction
1.1. What is Vitamin D?
1.2. Vitamin D metabolic pathway
1.3. Vitamin D: effects on immune function
1.3.1. Innate immunity
1.3.2. Cell-mediated immunity
1.3.3. Humoral immunity
- Evidence that vitamin D is linked to MS
2.1. Variation in MS according to latitude
2.2. Month of birth in people with MS
2.3. Observational epidemiological studies
2.4. Trial evidence
2.5. Vitamin D or UV radiation?
Genetics of MS
Genetic interactions
Clinical implications for vitamin D as therapy in MS
Conclusions
References