Review of Vitamin D Deficiencies in developing countries
Hypovitaminosis D in developing countries —prevalence, risk factors and outcomes
Asma Arabi, Rola El Rassi and Ghada El-Hajj Fuleihan
Calcium Metabolism and Osteoporosis Program, Division of Endocrinology, Department of Internal Medicine, American University of Beirut, PO Box 11-0236, Riad El Solh 1107 2020, Beirut, Lebanon, G. El-Hajj Fuleihan gf01@aub.edu.lb
Nature Reviews: Endocrinology
Abstract | Hypovitaminosis D is a prevalent disorder in developing countries. Clinical manifestations of hypovitaminosis D include musculoskeletal disorders, such as nonspecific muscle pain, poor muscle strength and low BMD, as well as nonmusculoskeletal disorders, such as an increased risk of respiratory infections, diabetes mellitus and possibly cardiovascular diseases. In developing countries, the prevalence of hypovitaminosis D varies widely by and within regions; prevalence ranges between 30-90%, according to the cut-off value used within specific regions, and is independent of latitude. A high prevalence of the disorder exists in China and Mongolia, especially in children, of whom up to 50% are reported to have serum 25-hydroxyvitamin D levels <12.5 nmol/l. Despite ample sunshine throughout the year, one-third to one-half of individuals living in Sub-Saharan Africa and the Middle East have serum 25-hydroxyvitamin D levels <25 nmol/l, according to studies published in the past decade. Hypovitaminosis D is also prevalent in children and the elderly living in Latin America. Risk factors for hypovitaminosis D in developing countries are similar to those reported in Western countries and include extremes of age, female sex, winter season, dark skin pigmentation, malnutrition, lack of sun exposure, a covered clothing style and obesity. Clinical trials to assess the effect of vitamin D supplementation on classical and nonclassical clinical outcomes in developing countries are needed.
📄 Download the PDF from VitaminDWiki
See also VitaminDWiki
Reasons for vitamin D Deficiency especially Air Conditioning
Published Recommendations of Vitamin D both IU and ng
Following text, with a few figures, are extracted to ease translation to other languages
Introduction
Vitamin D may be obtained from food, but its most important source is skin synthesis upon exposure to ultraviolet B radiation (UVB). The distance that sunlight travels to the earth's atmosphere is the least in regions nearest the equator. Thus, UVB rays are the most intense and vitamin D synthesis is possible all year long in zones extending between latitudes 23.5°N and 23.5°S to the equator (the tropics). In latitudes higher than the tropics, the angle of light striking the earth is such that UVB intensity becomes insufficient for vitamin D synthesis.1 In temperate zones (23.5°-66.5°), people lack sufficient UVB to synthesize vitamin D for 1 month of the year, whereas those nearer to the poles do not get enough UVB radiation for vitamin D synthesis for most of the year (Figure 1).1,2 Vitamin D—synthesized by the skin or obtained by food—is metabolized by the liver into 25-hydroxyvitamin D, which is hydroxylated in the kidney by the enzyme 25-hydroxyvitamin D-1a hydroxylase (encoded by the gene CYP27B1) to the active form 1,25-dihydroxyvitamin D. The actions of 1,25-dihydroxyvitamin D in multiple target tissues are mediated by the nuclear vitamin D receptor (VDR), a phosphoprotein that binds the hormone with high affinity (Figure 2).3,4 Serum 25-hydroxyvitamin D level is the best marker of whole-body vitamin D status.3,4 The cut-off to define vitamin D deficiency has been a matter of debate during the past decade; some consider levels >75 nmol/l to define sufficiency,5,6 while others consider 50 nmol/l an adequate cut-off level.7
Hypovitaminosis D is a widespread disorder across all age groups in developing countries and is, in addition to infectious diseases and malnutrition, among the most prevalent childhood health disorders in such countries.8 The high prevalence of hypovitaminosis D in a number of developing countries exists despite the fact that a large number of these countries lie in zones that have sufficient sunlight for vitamin D synthesis for most if not all of the year. The objectives of this article are to review the prevalence of hypovitaminosis D across the lifecycle in individuals from developing countries and discuss the risk factors and health outcomes associated with hypovitaminosis D. This Review used the World Bank classification of developing countries, which considers all low-income and middle-income countries as developing. In its most recent classification, a total of 144 countries were considered developing. These countries are located in East Asia and the Pacific, Europe and Central Asia, Latin America and the Caribbean, Sub-Saharan Africa, South Asia, and the Middle East and North Africa.
Information on the prevalence of hypovitamino-sis D, risk factors and effects on health were available from 23 developing countries and are reviewed herein (Figure 1). However, the reader is alerted to limitations inherent to the nature of the studies, namely that studies were mostly descriptive; population-based studies were scarce, and methodological standardization of measurement was lacking. In addition, a wide range of cut-off values were used to define vitamin D insufficiency or deficiency in the studies.
Prevalence of hypovitaminosis D
Countries within each region are introduced by order of latitude, starting with the countries that extend furthest from the equator. Studies quoted in Table 1 are those that included information on predictors of hypovitaminosis D.
East Asia and Pacific
Nutritional rickets is highly prevalent in Mongolia and China. In a study assessing the nutritional status of preschool children living in Ulaanbaatar in Mongolia in the 1990s, 50% of 342 randomly selected children had serum 25-hydroxyvitamin D levels <18 nmol/l.9 Furthermore, a pilot study including 46 schoolchildren aged 9-11 years in 2008 showed that 32% had serum 25-hydroxyvitamin D levels <37.5 nmol/l.10 The prevalence of rickets in China is reported to be among the highest in the world. In a study that included 250 infants (aged 12-24 months) living in Shanxi Province, the prevalence of rickets (defined as 25-hydroxyvitamin D <30 nmol/l) was 29% in springtime.11 Furthermore, Specker et al. reported a mean cord concentration of 25-hydroxyvitamin D of 27.5 nmol/l in 256 full-term Chinese babies in the 1990s.12 Lastly, in a study of 1,277 randomly selected healthy girls aged 12-14 years living in Beijing, serum 25-hydroxyvitamin D levels of <12.5 nmol/l were reported in 45% and 7% of the girls in winter and summer, respectively.13 Low vitamin D levels were associated with low calcium intake and limited sunlight exposure in Chinese and Mongolian populations.13,14
Key points
Hypovitaminosis D is a widespread disorder in developing countries, regardless of their latitude
The disorder is highly prevalent in China, Mongolia, Sub-Saharan Africa, the Middle East and Latin America, especially in children, the elderly and women
Risk factors are similar to those reported in Western countries and include extremes of age, female sex, winter season, low socioeconomic status, malnutrition, covered clothing style and dark skin
Clinical manifestations of hypovitaminosis D are not limited to musculoskeletal disorders, but may also include an increased risk of respiratory infections, diabetes mellitus and possibly cardiovascular diseases
Public health-awareness campaigns, as well as food fortification with vitamin D are efficacious and affordable means to prevent vitamin D deficiency
Clinical trials are needed to assess the effect of vitamin D supplementation on the burden of both communicable and noncommunicable diseases in developing countries
Hypovitaminosis D has been reported in women of all age groups living in the Philippines, Malaysia and Indonesia. This situation is surprising in view of the location near the equator of these southeastern Asian countries. In a study evaluating postmenopausal women living in Manila, the Philippines (n = 60) and Jakarta, Indonesia (n = 60), 20% and 73%, respectively, had a serum 25-hydroxyvitamin D level <50 nmol/l.15 Encouragingly, the study also found that fortified milk supplementation reduced these percentages to 22% in Indonesian women and to 0% in Filipino women. In a study of 103 Malay women aged 50-65 years from Kuala Lumpur, 71% were found to have serum 25-hydroxyvitamin D levels <50 nmol/l. Ethnicity, fat mass and BMI were associated with vitamin D status.16 In addition, over 60% of 504 women aged 18-40 years living in Kuala Lumpur or Jakarta in Indonesia were reported in 2008 to have serum 25-hydroxyvitamin D levels <50 nmol/l; ethnicity and dress style predicted serum 25-hydroxyvitamin D values.17 Another report in 2008 found that 35% of 74 Indonesian elderly women living in institutionalized care units in Jakarta or Bekasi in Indonesia had 25-hydroxyvitamin D levels <75 nmol/l.18
In summary, hypovitaminosis D is prevalent in children and women in this region of the world.
The highest prevalence is in China and Mongolia, where up to 50% of children have serum 25-hydroxyvitamin D levels <12.5 nmol/l.
Figure 1
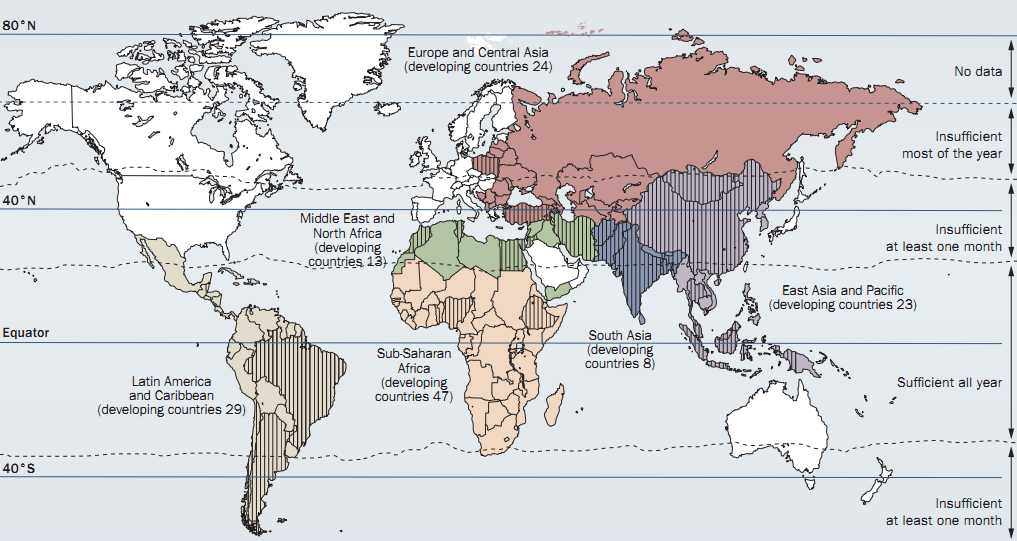
World map indicating developing countries as classified by World Bank criteria in color and relating latitude by geographic regions to skin ability to synthesize vitamin D as estimated from information provided in an article by Tavera-Mendoza and White.1 Developed countries are shown in white. Information on the prevalence of hypovitaminosis D, risk factors and effect on health was available from 23 developing countries that are indicated as shaded areas on the map.
Figure 2 is in PDF file
Figure 2 | Metabolism of 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D for nonskeletal functions. When monocytes and macrophages are stimulated by an infectious agent, the expression of vitamin D receptor and 25-hydroxyvitamin D-1a hydroxylase is upregulated, so that more 25-hydroxyvitamin D is converted to 1,25-dihydroxyvitamin D. This shift increases the expression of cathelicidin, which induces destruction of the infectious agent. 1,25-dihydroxyvitamin D also has a role in immunomodulation. The 1,25-dihydroxyvitamin D produced locally in tissues such as the breast, colon and prostate regulates some genes involved in proliferation, angiogenesis, differentiation and apoptosis. Locally produced 1,25-dihydroxyvitamin D also inhibits the expression and synthesis of parathyroid hormone. The 1,25-dihydroxyvitamin D produced in the kidney downregulates renin production and stimulates pancreatic p-cell insulin secretion. Abbreviations: 1-OHase, 25-hydroxyvitamin D-1a hydroxylase; 25(OH)D, 25-hydroxyvitamin D; 1,25(OH)2D, 1,25-dihydroxyvitamin D; RXR, retinoid X receptor; TLR, toll-like receptor; vDR, vitamin D receptor. Reproduced from Holick, M. F. vitamin D deficiency. N. Engl. J. Med. 357, 266-281 (2007) with permission, © 2007 Massachusetts Medical Society. All rights reserved.
Europe and Central Asia
Vitamin D deficiency is a common European problem. Nevertheless, relevant published studies from the 24 countries classified as developing by the World Bank in the region Europe and Central Asia are scarce. The discussion in this Review is, therefore, limited to findings in Turkey and Poland. In a study of 8,532 postmenopausal women with a mean age of 74.2 years from nine European countries, 30% of 1,544 women from Poland had hypovitaminosis D defined as serum 25-hydroxyvitamin D levels of <50 nmol/l; this prevalence level was similar to that found overall for the whole nine-country cohort.19 By use of the same cut-off value of 50 nmol/l, a prevalence of hypovitaminosis D of 83% was reported in winter among 274 women aged 60-90 years living in Warsaw, Poland.20 In a survey of 54 neonates and their mothers in Ankara, Turkey, 46% of the mothers and 80% of the neonates had 25-hydroxyvitamin D levels <25 nmol/l.
Table 1 | Prevalence and predictors of hypovitaminosis D in developing countries
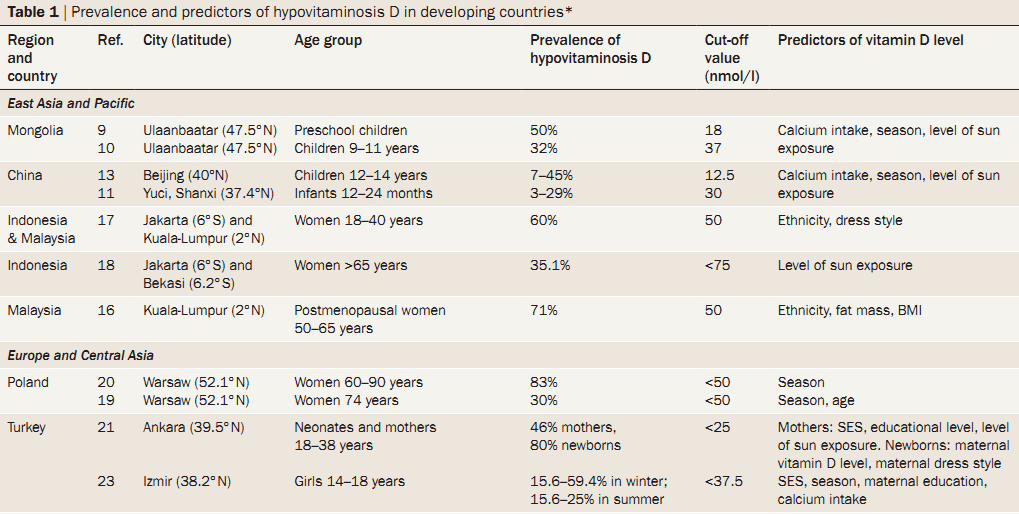
The table includes studies identified for the review that included predictors of hypovitaminosis D. Abbreviation: SES, socioeconomic status.
Predictors of low maternal vitamin D levels in mothers were low socioeconomic status, low educational level and reduced sun exposure as a result of a covered clothing style, and for neonates the predictors were a low maternal serum 25-hydroxyvitamin D level and a mother with a covered clothing style.21 In Erzurum province in Eastern Turkey, the incidence of rickets with serum 25-hydroxyvitamin D levels <12.5 nmol/l was 6% in preschool children in 1998, but this prevalence dropped to 0.09% when the Ministry of Health initiated a free nationwide vitamin D supplementation campaign targeting all infants in 2005.22 In 64 adolescent girls living in Izmir, the prevalence of hypovitaminosis D was 16-59% in winter and 16-25% in summer. The report, published in 2006, identified risk factors including end-of-winter period, low socioeconomic status, illiteracy of mothers and low calcium intake.23 In a case-control study of 50 male coal-miners and 50 surface workers in Zonguldak, Turkey, that aimed to determine the effect of underground work on vitamin D levels, mean serum 25-hydroxyvitamin D levels were low in both groups, 35 nmol/l and 24.5 nmol/l, respectively. Calcium intake was also low in both groups.24
Vitamin D deficiency is prevalent in this region, according to the evidence discussed above.
Hypovitaminosis D seemed to affect all age groups and both sexes in the studies from Turkey and to be prevalent in postmenopausal women in Poland.
Latin America and the Caribbean
Hypovitaminosis D has been widely reported in Argentina over the past decade.25-28 In a group of 42 children (mean age 8.5 years) living in Ushuaia, the southernmost city in the World, mean serum 25-hydroxyvitamin D levels were <50 nmol/l in summer and <25 nmol/l in winter.26 The levels were similar in children with fair or dark skin in winter but were higher in children with fair skin compared to those with dark skin in the summer.26 In seven different regions of Argentina, 57% of 386 elderly individuals had serum 25-hydroxyvitamin D levels <50 nmol/l at the end of winter.27 Serum 25-hydroxyvitamin D levels correlated with average sunshine hours, temperature and latitude. In Santiago, Chile, 60% of 60 ambulatory, postmenopausal women were found to have serum 25-hydroxyvitamin D levels <50 nmol/l.29 Old age, winter season and low calcium intake were independent predictors for low serum 25-hydroxyvitamin D levels.
In Brazil, studies in the past few years have revealed a high prevalence of hypovitaminosis D in different age groups and both sexes. Serum 25-hydroxyvitamin D levels were <50 nmol/l in 60% of 136 healthy students (64 boys and 72 girls) aged 16-20 years in Sao Paulo,30 and in 57% of 73 young resident physicians of a general hospital in Porto Alegre.31 In a cohort of 102 healthy elderly individuals with a mean age of 77 years from south Brazil, 86% had 25-hydroxyvitamin D levels <50 nmol/l.32 Serum 25-hydroxyvitamin D levels were not associated with age, sex or sun exposure in this study.32
The prevalence of hypovitaminosis D seemed to be the highest in this region of the world,
although the high prevalence might in part be explained by the relatively higher cut-off value of 50 nmol/l used in most studies from this region.
Sub-Saharan Africa
Rickets is common in children in Sub-Saharan Africa, but is mostly attributed to severe mixed calcium and vitamin D deficiencies rather than isolated vitamin D deficiency. Indeed, Nigerian children with rickets had a better response to calcium alone or in combination with vitamin D than vitamin D alone.33,34 Vitamin D deficiency rickets has also been described in Ethiopian children; predisposing factors included protein-energy malnutrition and lack of exposure to sunlight.35
South Asia
The South Asia region has UVB radiation levels that are sufficient for vitamin D synthesis for 11 to 12 months of the year, but serum 25-hydroxyvitamin D levels of <25 nmol/l have been reported in more than 50% of the infants, children and women studied. For example, in Kabul, Afghanistan, 73% of 107 preschool children randomly sampled in winter had 25-hydroxyvitamin D levels <20 nmol/l.36
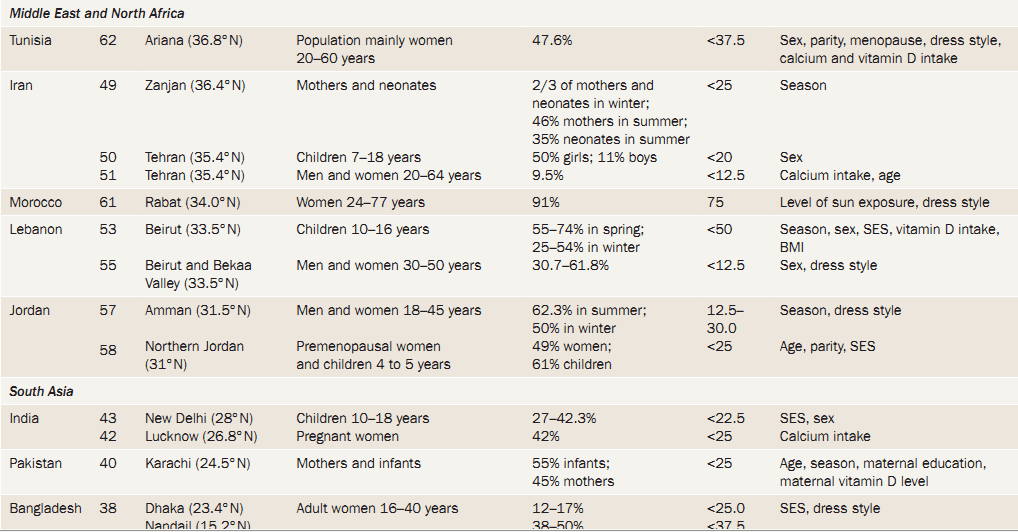
Rickets is commonly reported in Bangladesh, but nutritional calcium deficiency plays a major part. In a case-control study published in 1999 that included 14 children with rickets and 13 without rickets, 70% of children with active rickets had no evidence of hypovitaminosis D.37 Also in Bangladesh, suboptimal serum 25-hydroxyvita-min D levels (<25 nmol/l) were described in 189 women living in Dhaka or in Nandail cities, with high prevalence in lactating women of low socioeconomic status and those wearing the Shari that exposes only the face and hands to sunlight.38 In another survey of women aged 18-60 years in Dhaka, serum 25-hydroxyvitamin D levels were <40 nmol/l in 78% of 36 university students and in 83% of 30 veiled women. Predictors of low vitamin D included low parity and lack of time spent outdoors.39
In Pakistan, 55% of 62 infants and 45% of their nursing mothers who attended private and public well-baby clinics in Karachi were reported to have serum 25-hydroxyvitamin D levels <25 nmol/l.40 Infants <6 months of age had the lowest levels. Season, maternal education and maternal serum 25-hydroxyvitamin D levels correlated with serum 25-hydroxyvitamin D levels in infants.40 In the same city, 62% of a cohort of 119 ambulatory clinic patients with a mean age of 44 years were found to have serum 25-hydroxyvitamin D levels <20 nmol/l.41
In India, similar to Pakistan, nutritional factors and vitamin D status of mothers during pregnancy explains hypovitaminosis D in infants. High prevalence of hypo-vitaminosis D has been reported among Indian pregnant women (n = 207) from a maternity hospital in Lucknow: 42% had serum 25-hydroxyvitamin D values <25 nmol/l.42 Maternal vitamin D status correlated with that of their newborns (r = 0.79, P <0.001).42 In healthy adolescents in Delhi, 25-hydroxyvitamin D levels were <22.5 nmol/l in 27% and 42% of children of high and low socioeconomic status, respectively; boys had higher levels than girls.43 Lastly, in a study of 132 individuals, including people with depigmented skin, physicians, nurses, soldiers and pregnant women and their newborns living in Delhi, serum 25-hydroxyvitamin D levels were suboptimal in all groups except soldiers. Serum 25-hydroxyvitamin D levels were related to direct sunlight exposure and skin pigmentation.44
The Middle East and North Africa
The Middle East
In an international study of women with osteoporosis, the highest prevalence of hypovitaminosis D was reported in the Middle East.45
Within the Middle East, this finding was independent of national income.
Indeed, developed Arab Gulf countries carry a high prevalence of hypo-vitaminosis D, a finding possibly explained by cultural practices and skin pigmentation.46
A number of studies have reported vitamin D status in Iranian cohorts in the past decade. In a study of 88 newborns and their mothers in Isfahan, Iran, 25-hydroxyvitamin D levels were <50 nmol/l in 6% of mothers and <31 nmol/l in 5% of newborns.47 Eighty percent of 50 mothers in Tehran and 46% of 67 mothers in Zanjan had serum 25-hydroxyvitamin D <25 nmol/l, and low levels of serum 25-hydroxyvitamin D were found in neonates (mean 4.9 nmol/l and 16.7 nmol/l in Tehran and Zanjan, respectively).48,49 Serum 25-hydroxyvitamin D levels <20 nmol/l were common in a study of 963 schoolchildren in Tehran, and these levels were five times more prevalent in girls than in boys (50% versus 11%, respectively).50 In another study in Tehran, levels of serum 25-hydroxyvitamin D <12 nmol/l were reported in 10% of 1,210 healthy men and women aged 20-64 years; calcium intake and age correlated with vitamin D levels.51
Vitamin D status has been extensively studied among Lebanese schoolchildren living in Beirut in the past decade,52,53 with reported serum 25-hydroxyvitamin D levels of <25 nmol/l in 32% of 90 girls and 9% of 83 boys aged 10-16 years in fall.52 Studies in Lebanese adults also reported levels of <25 nmol/l in 60% of 465 women aged 20-59 years in summer.54 In another study, levels of serum 25-hydroxyvitamin D <12 nmol/l were reported in 31% of men and women aged 30-50 years (n = 316) and in 62% of the veiled women.55 Finally, a population-based study of 460 elderly individuals revealed that only 5% had serum 25-hydroxyvitamin D levels >50 nmol/l.56
In healthy Jordanians aged 18-45 years (22 men and 124 women) living in Amman, serum 25-hydroxyvitamin D levels <30 nmol/l were reported in 62% in summer and 50% in winter,57 predictors of serum 25-hydroxyvitamin D levels being season and dress style. Similarly, serum 25-hydroxyvitamin D levels <20 nmol/l were reported in 49% of young women (n = 93) and 61% of their preschool children living in northern Amman. Predictors were socioeconomic status in children, and age and parity, but not dress style, in mothers.58
In a study of 54 rachitic children and 28 healthy controls <3 years of age in Cairo, Egypt, mean 25-hydroxyvitamin D levels were 9 nmol/l and 25 nmol/l, respectively.59 In another case-control study of 98 rachitic and 58 healthy children aged 6-48 months recruited from university and community outpatient hospitals in Egypt and Turkey, 71% of rachitic patients and 42% of controls had 25-hydroxyvitamin D levels <37.5 nmol/l.60
The findings in the Middle Eastern population were similar to those of populations living in South Asian developing countries, with almost half of the population having serum 25-hydroxyvitamin D levels <25 nmol/l. Females, newborns and children were particularly at risk.
North Africa
Of 415 women aged 24-77 years living in Rabat, Morocco, 91% had 25-hydroxyvitamin D levels <75 nmol/l.61 Lack of sun exposure and veiled clothing style were the most important predictors61. In a study of 389 healthy Tunisians aged 20-60 years, living in Ariana, 48% had serum 25-hydroxyvitamin D levels <37.5 nmol/l. Predictors of low serum 25-hydroxyvitamin D levels included female sex, multiparity, menopause, veiling and low calcium and vitamin D intake.62
Risk factors for hypovitaminosis D
Several risk factors are associated with hypovitamino-sis D in developing countries. Female sex and particular age groups (neonates, preschool children or the elderly) were the most consistently reported risk factors for hypovitaminosis D (Table 1).29,40,43,51,52,58,62 Obesity is an emerging endemic health problem, which is rapidly increasing in developing countries.63 Vitamin D levels negatively correlate with BMI and fat mass in Pacific Island populations,16 findings that are compatible with the long-standing concept that adipose tissue is a storage site for vitamin D.64
Skin pigmentation may affect vitamin D synthesis, and evidence in support of this hypothesis is available in South Asian populations.44,65 Melanin acts as a natural sunscreen and reduces the production of previtamin D in human skin during sunlight exposure.66 Lo et ul.67 showed that Asian Indians and Pakistanis have similar capacity as white individuals to produce vitamin D in their skin but need longer exposure to produce a similar response. A concealing clothing style was a consistent predictor of low vitamin D levels in the Middle East, East Asia and North Africa.17,21,23,38,55,61,62
Season and latitude affect vitamin D synthesis in the skin.3,4 Lower serum 25-hydroxyvitamin D levels are reported in winter and spring compared to summer and fall in studies from temperate regions in the developing world.13,23,26,27,29,40,57 Paradoxically, studies from Gulf areas show that mean vitamin D levels are lower in the summer than in winter because people avoid going outdoors owing to the intolerable heat of that season.46
Latitude affects vitamin D synthesis in the skin and, therefore, low vitamin D levels are expected at high latitudes in the absence of vitamin D supplementation. However, such trends were not possible to establish in this Review (Table 1). Low vitamin D levels in the Middle East, North Africa and South Asia may reflect cultural dress customs that limit skin exposure.38,55,57,61,62 Furthermore, government public health interventions and guidelines on vitamin D supplementation to improve vitamin D levels are lacking in countries in these regions.
Individuals with hypovitaminosis D were mostly of low socioeconomic status and were reported to have low daily intake of calcium, namely in East Asia, Latin America, Sub-Saharan Africa and North Africa.13,14,21,23,24,27,29,35,40,43,46,51,58,62 Malnutrition and protein deficiency cause a decrease in the vitamin D binding protein in blood, which diminishes the ability of the body to conserve 25-hydroxyvitamin D.68 Low calcium intake was reported as a predictor or a determinant of low vitamin D in some studies; however, low calcium intake is probably associated with low vitamin D levels rather than being a causative factor.
Atmospheric pollution has been suggested to be a cause of reduced vitamin D synthesis in the skin. Agarwal et ul.69 showed that the higher the atmospheric pollution, the lower the amount of UVB light reaching ground level. They also showed that children living in an area with high levels of atmospheric pollution had lower mean serum total 25-hydroxyvitamin D concentrations (31 nmol/l) than those living in similar types of housing but in a less polluted area of Delhi (68 nmol/l).69
Finally, a few studies showed an association between VDR gene polymorphisms and 25-hydroxyvitamin D levels in Egyptian and Turkish children,60 but not in Lebanese individuals.70 Whether genetic factors interacting with environmental factors increase the predisposition to low vitamin D levels in some populations needs to be further investigated.
In summary, nutritional status, obesity, skin pigmentation, clothing style and seasonal variation affect vitamin D levels in developing countries.
Females and individuals at the extremes of age are most affected.
However, these risk factors have already been described in Western populations and, therefore, are not unique to developing countries.
Musculoskeletal outcomes
Data linking any health outcomes to hypovitaminosis D in developing countries are scarce, suffer from multiple limitations and have led to inconsistent results. Musculoskeletal disorders associated with low vitamin D status start in utero. Maternal vitamin D status affects intrauterine skeletal mineralization, bone growth and muscle development.71,72 Hypovitaminosis D causes rickets in children and osteomalacia in adults. In the elderly, the disorder decreases muscle strength and BMD and increases the risk of falls and osteoporotic fractures.73,74 Studies in Arab and Indo-Pakistani patients have shown a high prevalence of hypovitaminosis D among patients suffering from nonspecific muscle pain.75
Serum 25-hydroxyvitamin D levels correlate with lean body mass and with BMD at multiple skeletal sites in healthy adolescent Lebanese girls aged 10-17 years53 and, similarly, in elderly Lebanese individuals.56 In addition, in 301 healthy Chinese adolescent girls, those with poor vitamin D status have lower muscle strength and bone mass at the total body and forearm than those with adequate vitamin D status.76
The effect of 25-hydroxyvitamin D on bone mass may be mediated by parathyroid hormone (PTH) levels.56 Indeed, in a prospective population-based study assessing bone loss and fractures in 195 ambulatory Lebanese individuals (65 men and 130 women) aged 65-85 years who were followed-up for a median of 4 years, PTH but not 25-hydroxyvitamin D levels predicted bone-loss rates, which suggests that vitamin D osteopathy is partially mediated by PTH.56,77 Conversely, total-body bone mineral content and BMD measured during the first 24 h of life were not related to the 25-hydroxyvitamin D level of 100 neonates or their mothers in Turkey.78 Furthermore, 25-hydroxyvitamin D level did not correlate with BMD in 245 healthy, free-living postmenopausal Iranian women aged 40-80 years,79 nor with BMD and physical performance in a cohort of healthy ambulatory, premenopausal (n = 108, mean age 42 years) and postmenopausal (n = 307, mean age 56 years) women from Morocco.61
Nonmusculoskeletal outcomes
VDR is widely expressed in over 30 tissues and organs, and the enzyme 25-hydroxyvitamin D-1a hydroxylase is expressed in some of these tissues.
This knowledge has led to the recognition of the varied nonclassical physiologic activities of vitamin D (Figure 2).
Thus, hypo-vitaminosis D has emerged as a potential risk factor for infections and chronic diseases.3,4,80
Studies to show the associations between hypo-vitaminosis D and nonmusculoskeletal health disorders, and those evaluating the effect of vitamin D supplementation on the prevalence and/or the course of these diseases have mainly been conducted in populations from Western countries. Probably, these associations can be extrapolated to developing countries; however, genetic and/or modifiable factors influencing these associations have not been demonstrated and, therefore, these associations need to be investigated in developing countries.
Infectious diseases
Acute respiratory infections cause 4.5 million deaths among children per year in developing countries.
These infections are the leading cause of morbidity and mortality in preschool children in developing countries.81,82
Exposure of monocytes and macrophages to Mycobacterium tuberculosis leads to the production of catheli-cidin, a peptide capable of destroying M. tuberculosis and other infectious agents.83 This capacity to produce catheli-cidin is inhibited when serum 25-hydroxyvitamin D levels fall below 50 nmol/l.84 Strong associations between hypovitaminosis D and M. tuberculosis infection and acute lower respiratory tract infections have been reported in Indian, Turkish and Sub-Saharan African populations.85-87 In a hospital-based, case-control study of 25 neonates with acute lower respiratory tract infections and 15 healthy neonates in Turkey, mean serum 25-hydroxyvitamin D concentrations in the study group were lower than those of the control group (22.5 nmol/l and 40.7 nmol/l, respectively). Mothers of the study group also had lower mean serum 25-hydroxyvitamin D concentrations than those in the control group (33.2 nmol/l and 56.7 nmol/l, respectively).88 Moreover, radiological evidence of rickets was associated with an increased risk of wheezing bronchitis in a case-control study in Iraqi infants.89
Autoimmune diseases
Autoimmune diseases are less prevalent in developing than developed countries,90,91 but VDR is widely expressed in most immune cell types, such as the antigen-presenting cells—T cells and B cells (Figure 2).80 Vitamin D has a major role in determining the immune responses involved in autoimmune diseases. In the Framingham study, the development and progression of osteoarthritis was related to vitamin D levels.92 Similar observations have been made for rheumatoid arthritis.93 Vitamin D also seems to have a protective role against the development of type 1 diabetes mellitus.94 Evidence linking hypovitaminosis D to autoimmune disorders in developing countries is lacking. However, the link between autoimmunity and hypovitaminosis D may contribute to the change in the global epidemiology of such conditions in these regions if left unaddressed.
The metabolic syndrome
The prevalence of obesity and the metabolic syndrome has risen rapidly in developing countries in the past few decades.63 Even if individuals are not obese by conventional BMI classification, some people in South Asia have high abdominal adiposity and thick truncal subcutaneous fat that contributes to insulin resistance, hyperglycemia, dyslipidemia and inflammation.95 Obesity alters the release of vitamin D into the circulation and decreases its bioavail-ability because of deposition in adipose tissue compartments.16,64 The consequent hypovitaminosis D may predispose individuals to cardiovascular disease through associations with type 2 diabetes mellitus, hypertension, dyslipidemia and increased inflammatory markers.96
Pancreatic (3 cells express VDR, and hypovitaminosis D induces insulin resistance and ((-cell dysfunction.96-98 In a cohort of 246 Thai individuals with a mean age of 62 years, 25-hydroxyvitamin D levels negatively correlated with HOMA-IR (homeostasis model assessment of insulin resistance) and mean serum 25-hydroxyvitamin D levels were slightly lower in participants with abnormal than those with normal glucose tolerance (52.5 versus 55.25 nmol/l).99 Similarly, serum 25-hydroxyvitamin D levels were inversely correlated with fasting blood glucose levels and HOMA-IR in a cohort of 381 Lebanese university students.100 This correlation persisted with fasting blood glucose levels but not with HOMA-IR after adjustment for sex and BMI.100 Conversely, no correlation was found between serum 25-hydroxyvitamin D levels and fasting blood glucose levels, HbA1c or lipid profile in 119 Iranian patients with a mean age of 55 years with type 2 diabetes mellitus.101 In addition, serum 25-hydroxyvitamin D levels measured at 30 weeks of gestation in 559 Indian women showed that hypovitamino-sis D was common (66% with serum 25-hydroxyvitamin D <50 nmol/l) but not associated with the incidence of gestational diabetes mellitus.102
Vitamin D is a potent suppressor of renin biosynthesis, and blood pressure follows an inverse relationship with vitamin D levels.103 In Western countries, serum 25-hydroxyvitamin D levels inversely correlate with cholesterol and triglyceride levels104 and lipid profile improves with the consumption of oily fish.105 Hypovitaminosis D was associated with increased levels of C-reactive protein and interleukin 6 and with increased overall mortality, including cardiovascular mortality, in a 7.7-year prospective cohort of 3,258 patients (mean age 62 years) undergoing coronary angiography. Lowest quartiles of 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D levels were associated with a doubling of all-cause mortality and cardiovascular mortality risks compared with highest quartiles. These effects were independent of coronary artery disease, physical activity level and New York Heart Association class.106
In healthy Lebanese university students, 25-hydroxy-vitamin D levels correlated negatively with LDL cholesterol and positively with HDL cholesterol. The inverse correlation with LDL cholesterol persisted after adjustment for sex, BMI and exercise.100 In a study of 170 healthy British Bangladeshi individuals aged 35-65 years, serum 25-hydroxyvitamin D level was an independent predictor for apolipoprotein A-I, but not for other components of the fasting lipid profile, after adjustment for glycemia, dietary and lifestyle risk factors,107 which suggests that individuals with low vitamin D status might be at an increased risk of cardiovascular disease independent of risk of type 2 diabetes mellitus.107 25-Hydroxyvitamin D level correlated with levels of C-reactive protein and cardiovascular disease risk, but not with fasting blood glucose levels, in Iranian women, which suggests that inflammatory markers contribute to the association between low vitamin D level and cardiovascular disease risk.101
Cancer
Cancer is a major cause of mortality throughout the world.
Developing countries account for more than half of the global cancer burden and it is estimated that by 2020, 60% of new cases will occur in these nations.108
VDR regulates genes in the breast, prostate, colon and other tissues. The local production of 1,25-dihydroxy-vitamin D in prostate, breast and colon tissues inhibits the growth of cancer cells by induction of expression of the tumor suppressor genes p21 and p27 and inhibition of the expression of other genes such as the cyclin-dependent kinase 2 gene, which results in control of cell proliferation and the transformation of cells to a more differentiated phenotype.80 Studies conducted in Western countries have shown that 25-hydroxyvitamin D levels <50 nmol/l are associated with an increased risk of breast, prostate and colon cancer and a decreased survival rate in these cancers.109-111
No studies, to the best of the authors' knowledge, have assessed the relationship between vitamin D and cancer in developing countries. However, in view of the documented association between vitamin D and cancer and the high prevalence of hypovitaminosis D in developing countries, low vitamin D levels might explain, at least in part, the occurrence of cancers at younger ages than in developed countries, even after adjusting for life expectancy. The high prevalence of hypovitaminosis D might also explain the more aggressive nature of cancers in developing countries. Indeed, almost half of all women with breast cancer in Arab countries are <50 years of age—median age 49-52 years compared with median age 63 years in industrialized nations.112 Cancer survival is also lower in developing than in developed countries, whether there is an association with low vitamin D levels needs to be investigated.113
Effect of vitamin D supplementation
Musculoskeletal parameters
Studies conducted in Western countries clearly demonstrate the efficacy of vitamin D supplementation in improving muscle strength, reducing falls and decreasing the incidence of fractures.74,114 The evidence from developing countries is scarce. However, regimens including daily, weekly or monthly use of oral or injectable forms of vitamin D have been shown to be efficacious.115
The incidence of rickets dropped from 6% in 1998 to 0.099% in 2008 in a study conducted in Turkey.22 During a 1-year period (2007-2008), out of 39,133 children aged 0-3 years who were brought to different pediatric outpatient clinics in Erzurum, Turkey, only 39 (0.099%) were diagnosed with vitamin D-dependent rickets.22 This low rate was attributed to a free national vitamin D supplementation campaign initiated by the Ministry of Health in Turkey in 2005 to eradicate vitamin D-dependent rickets. Furthermore, in a randomized, placebo-controlled trial to assess the effect of vitamin D supplementation on musculoskeletal health in 179 healthy adolescent Lebanese girls aged 10-17 years who were randomly allocated to receive placebo (n = 58), 1,400 IU vitamin D per week (n = 62) or 14,000 IU vitamin D per week (n = 59) for 1 year, both doses of vitamin D supplementation increased lean mass, bone area, BMC and BMD at several skeletal sites.53 Lastly, in a case-control study, 4 months of consumption of vitamin D-fortified milk improved serum 25-hydroxyvitamin D levels and decreased bone turnover in 120 healthy postmenopausal Indonesian and Filipino women with a mean age of 58 years.15
In conclusion, scarce but optimistic data on the effect of vitamin D supplementation on musculoskeletal health in developing countries exists that needs to be confirmed by long-term studies.
Nonmusculoskeletal parameters
Almost all studies that have assessed the effect of vitamin D therapy on chronic and infectious diseases have been conducted in Western countries.
Vitamin D supplementation may offer protection against the development of type 1 diabetes mellitus in infancy.95,116 In a birth cohort study conducted in Finland that included 12,058 live births followed-up for 11 years, vitamin D supplementation with 2,000 IU daily during the first year of life was associated with a decreased risk of type 1 diabetes mellitus (relative risk 0.12).94 A single, large dose of oral vitamin D (100,000 IU) improved endothelial function in 87 patients from Scotland with type 2 diabetes mellitus and vitamin D insufficiency.117 Moreover, a meta-analysis that identified 18 studies from developed countries with a total of 57,311 participants, showed that dietary supplementation with daily doses of vitamin D varying between 300-2,000 IU decreased total mortality rate by 7%.118 However, in the Women's Health Initiative, calcium plus vitamin D supplementation over 7 years did not reduce blood pressure or the risk of developing hypertension119 or type 2 diabetes mellitus120 in postmenopausal women. Vitamin D supplementation also did not decrease the incidence or severity of upper respiratory tract infections during winter in 162 healthy adults living in New York who were randomly allocated to receive 2,000 IU vitamin D per day or placebo for 12 weeks.121
In developing countries, vitamin D supplementation did not improve clinical outcome or mortality in a randomized controlled trial in 367 adult patients with tuberculosis from Guinea-Bissau.122 However, administration of 0.5 ug alfacalcidol daily with insulin for 1 year preserved islet (-cell function better than insulin alone in a randomized controlled trial in a group of 35 Chinese adult patients with late autoimmune diabetes.123
Conclusions
Hypovitaminosis D is highly prevalent across age groups in developing countries. Consistent risk factors include female sex, extremes of age, covered clothing styles, low socioeconomic background and winter season. Evidence regarding the effect of hypovitaminosis D on musculo-skeletal and nonmusculoskeletal health outcomes in developing countries is scarce and the effect of VDR gene polymorphisms on these clinical manifestations is unclear. Adequately designed randomized controlled trials that aim to establish the optimum dose, duration and effect of vitamin D supplementation on multiple health outcomes in populations living in such countries are needed.
The need for nutritional public health-awareness campaigns about the importance of vitamin D is pressing, specifically in countries where the prevalence of hypovitaminosis D is very high. Evidence from developed countries of the safety and efficacy of vitamin D supplementation for the improvement of musculo-skeletal outcomes related to low vitamin D levels renders the institution and implementation of national health policies in developing countries mandatory. These policies would, however, require further revisions based on evidence from locally conducted studies.
Review criteria
Developing countries were identified using the World Bank Classification. A PubMed search was then conducted entering the key term "developing countries" with the term "hypovitaminosis D", and by entering the individual names of the countries of interest identified as described above with the terms "vitamin D or hypovitaminosis D". The search was limited to English language articles published between 1990 and 2010. The content of the abstracts of identified articles were checked and the papers of interest that could be retrieved were included in this Review. References of identified papers were also checked for relevant reports. Finally, reviews and publications on hypovitaminosis D available in the authors' library files were also used.
Tavera-Mendoza, L. E. & White, J. H. Cell defenses and the sunshine vitamin. Sci. Am. 297, 68-70 (2007).
Mithal, A. et al. Global vitamin D status and determinants of hypovitaminosis D. Osteoporos. Int. 20, 1807-1820 (2009).
Holick, M. F. Vitamin D deficiency. N. Engl. J. Med. 357, 266-281 (2007).
DeLuca, H. F. Overview of general physiologic features and functions of vitamin D. Am. J. Clin. Nutr. 80, 1689S-1696S (2004).
Dawson-Hughes, B. et al. Estimates of optimal vitamin D status. Osteoporos. Int. 16, 713-716 (2005).
Holick, M. F. 25-OH-vitamin D assays. J. Clin. Endocrinol. Metab. 90, 3128-3129 (2005).
Lips, P. Vitamin D status and nutrition in Europe and Asia. J. Steroid Biochem. Mol. Biol. 103, 620-625 (2007).
Papandreou, D., Malindretos, P, Karabouta, Z. & Rousso, I. Possible health implications and low vitamin D status during childhood and adolescence: An updated mini review. Int. J. Endocrinol. 2010, 472173 (2010).
Kachondham, Y., Dhanamitta, S., Oyunbileg, M. & Brown, L. Child health and nutritional status in Ulaanbaatar, Mongolia: a preliminary assessment. Asia Pac. J. Public Health 6, 226-232 (1992-1993).
Ganmaa, D. et al. Effects of vitamin D fortified milk on vitamin D status in Mongolian school age children. Asia Pac. J. Clin. Nutr. 17, 68-71 (2008).
Strand, M. A. et al. Diagnosis of rickets and reassessment of prevalence among rural children in Northern China. Pediatr. Int. 49, 202-209 (2007).
Specker, B. L. et al. Prospective study of vitamin D supplementation and rickets in China. J. Pediatr. 120, 733-739 (1992).
Du, X. et al. Vitamin D deficiency and associated factors in adolescent girls in Beijing. Am. J. Clin. Nutr. 74, 494-500 (2001).
Fraser, D. R. Vitamin D-deficiency in Asia. J. Steroid Biochem. Mol. Biol. 89-90, 491 495 (2004).
Kruger, M. C. et al. The effect of a fortified milk drink on vitamin D status and bone turnover in post-menopausal women from South East Asia Bone 46, 759-767 (2010).
Rahman, S. A., Chee, W. S., Yassin, Z. & Chan, S. P Vitamin D status among Postmenopausal Malaysian women. Asia Pac. J. Clin. Nutr. 13, 255-260 (2004).
Green, T. J. et al. Vitamin D status and its association with parathyroid hormone concentrations in women of child-bearing age living in Jakarta and Kuala Lumpur. Eur. J. Clin. Nutr. 62, 373-378 (2008).
Setiati, S. Vitamin D status among Indonesian elderly women living in institutionalized care units. Acta Med. Indones. 40, 78-83 (2008).
Bruyere, O., Malaise, O., Neuprez, A., Collette, J. & Reginster, J. Y. Prevalence of vitamin D inadequacy in European postmenopausal women. Curr. Med. Res. Opin. 23, 1939-1944 (2007).
Napiorkowska, L. et al. Prevalence of low serum vitamin D concentration in an urban population of elderly women in Poland. Pol. Arch. Med. Wewn. 119, 699-703 (2009).
Andiran, N., Yordam, N. & Ozon, A. Risk factors for vitamin D deficiency in breast-fed newborns and their mothers. Nutrition 18, 47-50 (2002).
Ozkan, B. et al. Prevalence of vitamin D deficiency rickets in the eastern part of Turkey. Eur. J. Pediatr. 168, 95-100 (2009).
Olmez, D., Bober. E., Buyukgebiz, A. & Cimrin, D. The frequency of vitamin D insufficiency in healthy female adolescents. Acta Paediatr. 95, 1266-1269 (2006).
Sarikaya, S. et al. Effect of underground working on vitamin D levels and bone mineral densities in coal miners: a controlled study. J. Int. Med. Res. 34, 362-366 (2006).
Duran, P, Mangialavori, G., Biglieri, A., Kogan, L. & Abeya Gilardon, E. [Nutrition status in Argentinean children 6 to 72 months old: results from the National Nutrition and Health Survey (ENNyS)]. Arch. Argent Pediatr. 107, 397-404 (2009).
Oliveri, M. B., Ladizesky, M., Mautalen, C. A., Alonso, A. & Martinez, L. Seasonal variations of 25 hydroxyvitamin D and parathyroid hormone in Ushuaia (Argentina), the southernmost city of the world. Bone Miner. Res. 20, 99-108 (1993).
Oliveri, B. et al. High prevalence of vitamin D insufficiency in healthy elderly people living at home in Argentina. Eur. J. Clin. Nutr. 58 337-342 (2004).
Portela, M. L. et al. Comparative 25-OH-vitamin D level in institutionalized women older than 65 years from two cities in Spain and Argentina having a similar solar radiation index. Nutrition 26, 283-289 (2010).
Gonzalez, G. et al. High prevalence of vitamin D deficiency in Chilean healthy postmenopausal women with normal sun exposure: additional evidence for a worldwide concern. Menopause 14, 455-461 (2007).
Peters, B. S., dos Santos, L. C., Fisberg, M., Wood, R. J. & Martini, L. A. Prevalence of vitamin D insufficiency in Brazilian adolescents. Ann. Nutr. Metab. 54, 15-21 (2009).
Premaor, M. O. et al. Hypovitaminosis D and secondary hyperparathyroidism in resident physicians of a general hospital in southern Brazil. J. Endocrinol. Invest. 31, 991-995 (2008).
Scalco, R., Premaor, M. O., Froehlich, P. E. & Furlanetto, T. W. High prevalence of hypovitaminosis D and secondary hyperparathyroidism in elders living in nonprofit homes in South Brazil. Endocrine 33, 95-100 (2008).
Okonofua, F. et al. Rickets in Nigerian children: a consequence of calcium malnutrition. Metabolism 40, 209-213 (1991).
Pfitzner, M. A. et al. Absence of vitamin D deficiency in young Nigerian children. J. Pediatr. 133, 740-744 (1998).
Lulseged, S. & Fitwi, G. Vitamin D deficiency rickets: socio-demographic and clinical risk factors in children seen at a referral hospital in Addis Ababa. East Afr. Med. J. 76, 457-461 (1999).
Manaseki-Holland, S., Zulf Mughal, M., Bhutta, Z. & Qasem Shams, M. Vitamin D status of socio-economically deprived children in Kabul, Afghanistan. Int. J. Vitam. Nutr. Res. 78, 16-20 (2008).
Fischer, P R. et al. Nutritional rickets without vitamin D deficiency in Bangladesh. J. Trop. Pediatr. 45, 291-293 (1999).
Islam, M. Z. et al. Vitamin D deficiency: a concern in premenopausal Bangladeshi women of two socio-economic groups in rural and urban region. Eur. J. Clin. Nutr. 56, 51-56 (2002).
Islam, M. Z., Akhtaruzzaman, M. & Lamberg-Allardt, C. Hypovitaminosis D is common in both veiled and nonveiled Bangladeshi women. Asia Pac. J. Clin. Nutr. 15, 81-87 (2006).
Atiq, M., Suria, A., Nizami, S. Q. & Ahmed, I. Vitamin D status of breastfed Pakistani infants. Acta Paediatr. 87, 737-740 (1998).
Zuberi, L. M., Habib, A., Haque, N. & Jabbar, A. Vitamin D deficiency in ambulatory patients. J. Pak. Med. Assoc. 58, 482-484 (2008).
Sachan, A. et al. High prevalence of vitamin D deficiency among pregnant women and their newborns in northern India. Am. J. Clin. Nutr. 81, 1060-1064 (2005).
Marwaha, R. K. et al. Vitamin D and bone mineral density status of healthy schoolchildren in Northern India. Am. J. Clin. Nutr. 82, 477-482 (2005).
Goswami, R. et al. Prevalence and significance of low 25-hydroxyvitamin D concentrations in healthy subjects in Delhi. Am. J. Clin. Nutr. 72, 472-475 (2000).
Lips, P et al. The prevalence of vitamin D inadequacy amongst women with osteoporosis: an international epidemiological investigation. J. Intern. Med. 260, 245-254 (2006).
Saadi, H. F. et al. Predictors and relationships of serum 25 hydroxyvitamin D concentration with bone turnover markers, bone mineral density, and vitamin D receptor genotype in Emirati women. Bone 39, 1136-1143 (2006).
Salek, M. et al. Vitamin D deficiency among pregnant women and their newborns in Isfahan, Iran. Exp. Clin. Endocrinol. Diabetes 116, 352-356 (2008).
Bassir, M. et al. Vitamin D deficiency in Iranian mothers and their neonates: a pilot study. Acta Paediatr. 90, 577-579 (2001).
Kazemi, A., Sharifi, F., Jafari, N. & Mousavinasab, N. High prevalence of vitamin D deficiency among pregnant women and their newborns in an Iranian population. J. Womens Health (Larchmt) 18, 835-839 (2009).
Rabbani, A. et al. Vitamin D insufficiency among children and adolescents living in Tehran, Iran. J. Trop. Pediatr. 55, 189-191 (2009).
Hashemipour, S. et al. Vitamin D deficiency and causative factors in the population of Tehran. BMC Public Health 25, 38 (2004).
El-Hajj Fuleihan, G. et al. Hypovitaminosis D in healthy schoolchildren. Pediatrics 107, E53 (2001).
El-Hajj Fuleihan, G. et al. Effect of vitamin D replacement on musculoskeletal parameters in school children: a randomized controlled trial. J. Clin. Endocrinol. Metab. 91, 405-412 (2006).
Fuleihan, G. E. & Deeb, M. Hypovitaminosis D in a sunny country. N. Engl. J. Med. 340, 1840-1841 (1999).
Gannage-Yared, M. H., Chemali, R., Yaacoub, N. & Halaby, G. Hypovitaminosis D in a sunny country: relation to lifestyle and bone markers. J. Bone Miner. Res. 15, 1856-1862 (2000).
Arabi, A. et al. Hypovitaminosis D osteopathy: is it mediated through PTH, lean mass, or is it a direct effect? Bone 39, 268-275 (2006).
Mishal, A. A. Effects of different dress styles on vitamin D levels in healthy young Jordanian women. Osteoporos. Int. 12, 931-935 (2001).
Gharaibeh, M. A. & Stoecker, B. J. Assessment of serum 25(OH)D concentration in women of childbearing age and their preschool children in Northern Jordan during summer. Eur. J. Clin. Nutr. 63, 1320-1326 (2009).
Lawson, D. E. et al. Etiology of rickets in Egyptian children. Hum. Nutr. Clin. Nutr. 41, 199-208 (1978).
Baroncelli, G. I. et al. Rickets in the Middle East: role of environment and genetic predisposition. J. Clin. Endocrinol. Metab. 93,
Allali, F. et al. High prevalence of hypovitaminosis D in Morocco: relationship to lifestyle, physical performance, bone markers, and bone mineral density. Semin. Arthritis Rheum. 38, 444-451 (2009).
Meddeb, N. et al. Vitamin D deficiency in Tunisia. Osteoporos. Int. 16, 180-183 (2005).
Misra, A. & Khurana, L. Obesity and the metabolic syndrome in developing countries. J. Clin. Endocrinol. Metab. 93 (Suppl. 1), S9-S30 (2008).
Wortsman, J., Matsuoka, L. Y., Chen, T. C., Lu, Z. & Holick, M. F. Decreased bioavailability of vitamin D in obesity. Am. J. Clin. Nutr. 72, 690-693 (2000).
Masood, S. H. & Iqbal, M. P Prevalence of vitamin D deficiency in South Asia. Pak. J. Med. Sci. 24, 891-897 (2008).
Clemens, T. L., Adams, J. S., Henderson, S. L. & Holick, M. F. Increased skin pigment reduces the capacity of skin to synthesize vitamin D3. Lancet 9, 74-76 (1982).
Lo, C. W., Paris, PW. & Holick, M. F. Indian and Pakistani immigrants have the same capacity as Caucasians to produce vitamin D in response to ultraviolet irradiation. Am. J. Clin. Nutr. 44, 683-685 (1986).
Laing, C. J. & Fraser, D. R. Changes with malnutrition in the concentration of plasma vitamin D binding protein in growing rats. Br. J. Nutr. 88, 133-139 (2002).
Agarwal, K. S. et al. The impact of atmospheric pollution on vitamin D status of infants and toddlers in Delhi, India. Arch. Dis. Child. 87, 111-113 (2002).
Arabi, A., Mahfoud, Z., Zahed, L., El-Onsi, L. & El-Hajj Fuleihan, G. Effect of age, gender and calciotropic hormones on the relationship between vitamin D receptor gene polymorphisms and bone mineral density in the Lebanese. Eur. J. Clin. Nutr. 64, 383-391 (2010).
Javaid, M. K. et al. Maternal vitamin D status during pregnancy and childhood bone mass at age 9 years: a longitudinal study. Lancet 367, 36-43 (2006).
Pawley, N. & Bishop, N. J. Prenatal and infant predictors of bone health: the influence of vitamin D. Am. J. Clin. Nutr. 80, 1748S-1751S (2004).
Bischoff-Ferrari, H. A. et al. Effect of vitamin D on falls: a meta-analysis. JAMA 291, 1999-2006 (2004).
Collins, D., Jasani, C., Fogelman, I. & Swaminathan, R. Vitamin D and bone mineral density. Osteoporos. Int. 8, 110-114 (1998).
Badsha, H., Daher, M. & Ooi Kong, K. Myalgias or non-specific muscle pain in Arab or Indo-Pakistani patients may indicate vitamin D deficiency. Clin. Rheumatol. 28, 971-973 (2009).
Foo, L. H. et al. Low vitamin D status has an adverse influence on bone mass, bone turnover, and muscle strength in Chinese adolescent girls. J. Nutr. 139, 1002-1007 (2009).
Arabi, A., Baddoura, G. & El-Hajj Fuleihan, G. PTH and not vitamin D predicts age-related bone loss in the elderly: A prospective population based study. Am. Soc. Bone Miner. Res. 23 (Suppl. 1), M178 (2008).
Akcakus, M. et al. The relationship between birthweight, 25-hydroxyvitamin D concentrations and bone mineral status in neonates. Ann. Trop. Paediatr. 26, 267-275 (2006).
Hosseinpanah, F., Rambod, M., Hossein-Nejad, A., Larijani, B. & Azizi, F. Association between vitamin D and bone mineral density in Iranian postmenopausal women. J. Bone Miner. Metab. 26, 86-92 (2008).
Nagpal, S., Na, S. & Rathnachalam, R. Noncalcemic actions of vitamin D receptor ligands. Endocr. Rev. 26, 662-687 (2005).
Berman, S. Epidemiology of acute respiratory infections in children of developing countries. Rev. Infect. Dis. 13 (Suppl. 6), S454-S462 (1991).
Savitha, M. R. et al. Modifiable risk factors for acute lower respiratory tract infections. Indian J. Pediatr. 74, 477-482 (2007).
Liu, PT., Stenger, S., Tang, D. H. & Modlin, R. L. Cutting edge: vitamin D-mediated human antimicrobial activity against Mycobacterium tuberculosis is dependent on the induction of cathelicidin. J. Immunol. 15, 2060-2063 (2007).
Liu, P T. et al. Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science 311, 1770-1773 (2006).
Gibney, K. B. et al. Vitamin D deficiency is associated with tuberculosis and latent tuberculosis infection in immigrants from sub-Saharan Africa. Clin. Infect. Dis. 46, 443-446 (2008).
Wayse, V., Yousafzai, A., Mogale, K. & Filteau, S. Association of subclinical vitamin D deficiency with severe acute lower respiratory infection in Indian children under 5 years. Eur. J. Clin. Nutr. 58, 563-567 (2004).
Nnoaham, K. E. & Clarke, A. Low serum vitamin D levels and tuberculosis: a systematic review and meta-analysis. Int. J. Epidemiol. 37, 113-119 (2008).
Karatekin, G., Kaya, A., Salihoglu, O., Balci, H. & Nuhoglu, A. Association of subclinical vitamin D deficiency in newborns with acute lower respiratory infection and their mothers. Eur. J. Clin. Nutr. 63, 473-477 (2009).
El-Radhi, A. S., Majeed, M., Mansor, N. & Ibrahim, M. High incidence of rickets in children with wheezy bronchitis in a developing country. J. R. Soc. Med. 75, 884-887 (1982).
Selmi, C. & Tsuneyama, K. Nutrition, geoepidemiology, and autoimmunity. Autoimmun. Rev. 9, A267-A270 (2010).
Mody, G. M. & Cardiel, M. H. Challenges in the management of rheumatoid ar thritis in developing countries. Best Pract. Res. Clin. Rheumatol. 22, 621-641 (2008).
McAlindon, T. E. et al. Relation of dietary intake and serum levels of vitamin D to progression of osteoarthritis of the knee among participants in the Framingham Study. Ann. Intern. Med. 125, 353-359 (1996).
Merlino, L. A. et al. Vitamin D intake is inversely associated with rheumatoid arthritis: results from the Iowa Women's Health Study. Arthritis Rheum. 50, 72-77 (2004).
Hypponen, E., Laara, E., Reunanen, A., Jarvelin, M. R. & Virtanen, S. M. Intake of vitamin D and risk of type 1 diabetes: a birth-cohort study. Lancet 358, 1500-1503 (2001).
Ruderman, N., Chisholm, D., Pi-Sunyer, X. & Schneider, S. The metabolically obese, normal-weight individual revisited. Diabetes 47, 699-713 (1998).
Pittas, A. G., Lau, J., Hu, F. B. & Dawson-Hughes, B. The role of vitamin D and calcium in type 2 diabetes. A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 92, 2017-2029 (2007).
Chiu, K. C., Chu, A., Go, V. L. & Saad, M. F. Hypovitaminosis D is associated with insulin resistance and beta cell dysfunction. Am. J. Clin. Nutr. 79, 820-825 (2004).
Boucher, B. J., Mannan, N., Noonan, K., Hales, C. N. & Evans, S. J. Glucose intolerance and impairment of insulin secretion in relation to vitamin D deficiency in east London Asians. Diabetologia 38, 1239-1245 (1995).
Nimitphong, H., Chanprasertyothin, S., Jongjaroenprasert, W. & Ongphiphadhanakul, B. The association between vitamin D status and circulating adiponectin independent of adiposity in subjects with abnormal glucose tolerance. Endocrine 36, 205-210 (2009).
Gannage-Yared, M. H. et al. Vitamin D in relation to metabolic risk factors, insulin sensitivity and adiponectin in a young Middle-Eastern population. Eur. J. Endocrinol. 160, 965-971 (2009).
Bonakdaran, S. & Varasteh, A. R. Correlation between serum 25 hydroxyvitamin D3 and laboratory risk markers of cardiovascular diseases in type 2 diabetic patients. Saudi Med. J. 30, 509-514 (2009).
Farrant, H. J. et al. Vitamin D insufficiency is common in Indian mothers but is not associated with gestational diabetes or variation in newborn size. Eur. J. Clin. Nutr. 63, 646-652 (2009).
Witham, M. D., Nadir, M. A. & Struthers, A. D. Effect of vitamin D on blood pressure: a systematic review and meta-analysis. J. Hypertens. 27, 1948-1954 (2009).
Rejnmark, L., Vestergaard, P, Heickendorff, L. & Mosekilde, L. Simvastatin does not affect vitamin D status, but low vitamin D levels are associated with dyslipidemia: results from a randomized, controlled trial. Int. J. Endocrinol. 2010, 957174 (2010).
Stanner, S. New thinking about diet and cardiovascular disease. J. Fam. Health Care 16, 71-74 (2006).
Dobnig, H. et al. Independent association of low serum 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D levels with all-cause and cardiovascular mortality. Arch. Intern. Med. 168, 1340-1349 (2008).
John, W. G., Noonan, K., Mannan, N. & Boucher, B. J. Hypovitaminosis D is associated with reductions in serum apolipoprotein A-I but not with fasting lipids in British Bangladeshis. Am. J. Clin. Nutr. 82, 517-522 (2005).
World Health Organisation (WHO). Cancer: Diet and Physical Activity's Impact [online], http:// www.who.int/dietphysicalactivity/publications/ facts/cancer/en/ (2010).
Gorham, E. D. et al. Vitamin D and prevention of colorectal cancer. J. Steroid Biochem. Mol. Biol. 97, 179-194 (2005).
Hanchette, C. L. & Schwartz, G. G. Geographic patterns of prostate cancer mortality. Evidence for a protective effect of ultraviolet radiation Cancer 70, 2861-2869 (1992).
Hines, S. L., Jorn, H. K., Thompson, K. M. & Larson, J. M. Breast cancer survivors and vitamin D: a review. Nutrition 26, 255-262 (2010).
El Saghir, N. S. et al. Trends in epidemiology and management of breast cancer in developing Arab countries: a literature and registry analysis. Int. J. Surg. 5, 225-233 (2007).
Parkin, D. M., Bray, F., Ferlay, J. & Pisani, P. Global cancer statistics, 2002. CA Cancer J. Clin. 55, 74-108 (2005).
Bischoff-Ferrari, H. A. et al. Fracture prevention with vitamin D supplementation: a meta-analysis of randomized controlled trials. JAMA 293, 2257-2264 (2005).
El-Hajj Fuleihan, G. In Vitamin D: Physiology, Molecular Biology and Clinical Applications 2nd edn Ch. 24 (ed. Holick, M.) 469-494 (Humana Press, New Jersey, New York, 2009).
Zipitis, C. S. & Akobeng, A. K. Vitamin D supplementation in early childhood and risk of type 1 diabetes: a systematic review and meta-analysis. Arch. Dis. Child. 93, 512-517 (2008).
Sugden, J. A., Davies, J. I., Witham, M. D., Morris, A. D. & Struthers, A. D. Vitamin D improves endothelial function in patients with type 2 diabetes mellitus and low vitamin D levels. Diabetes Med. 25, 320-325 (2008).
Autier, P. & Gandini, S. Vitamin D supplementation and total mortality: a meta-analysis of randomized controlled trials. Arch. Intern. Med. 167, 1730-1737 (2007).
Margolis, K. L. et al. Effect of calcium and vitamin D supplementation on blood pressure: the Women's Health Initiative Randomized Trial. Hypertension 52, 847-855 (2008).
de Boer, I. H. et al. Calcium plus vitamin D supplementation and the risk of incident diabetes in the Women's Health Initiative. Diabetes Care 31, 701-707 (2008).
Li-Ng, M. et al. A randomized controlled trial of vitamin D3 supplementation for the prevention of symptomatic upper respiratory tract infections. Epidemiol. Infect. 137, 1396-1404 (2009).
Wejse, C. et al. Vitamin D as supplementary treatment for tuberculosis: a double-blind, randomized, placebo-controlled trial. Am. J. Respir. Crit. Care Med. 179, 843-850 (2009).
Li, X. et al. Protective effects of 1-alpha-hydroxyvitamin D3 on residual beta-cell function in patients with adult-onset latent autoimmune diabetes (LADA). Diabetes Metab. Res. Rev. 25, 411-416 (2009).
Author contributions
A. Arabi, R. El Rassi and G. El-Hajj Fuleihan researched the data for the article, provided a substantial contribution to discussions of the content and reviewed and/or edited the manuscript before submission. A. Arabi and G. El-Hajj Fuleihan wrote the article.
NATURE REVIEWS | ENDOCRINOLOGY; © 2010 Macmillan Publishers Limited. All rights reserved; VOLUME 6 | OCTOBER 2010 | 561