Importance of Vitamins D and K
Vitamins D and K as pleiotropic nutrients: clinical importance to the skeletal and cardiovascular systems and preliminary evidence for synergy.
Altern Med Rev. 2010 Sep;15(3):199-222.
Kidd PM.
University of California, Berkeley, USA. dockidd@dockidd.com
See also VitaminDWiki
Vitamins D and K are lipid-phase nutrients that are pleiotropic - endowed with versatile homeostatic capacities at the organ, tissue, and cellular levels. Their metabolic and physiologic roles overlap considerably, as evidenced in the bone and cardiovascular systems. Vitamin D? (cholecalciferol, D?) is the prehormone for the vitamin D endocrine system. Vitamin D? undergoes initial enzymatic conversion to 25-hydroxyvitamin D (25D, calcidiol), then to the seco-steroid hormone 1alpha, 25-dihydroxyvitamin D (1,25D, calcitriol). Beyond its endocrine roles in calcium homeostasis, 1,25D likely has autocrine, paracrine, and intracrine effects. At least 17 tissues likely synthesize 1,25D, and 35 carry the vitamin D receptor (VDR). Vitamin D functional deficiency is widespread in human populations. Vitamin K? (phylloquinone) is more abundant in foods but less bioactive than the vitamin K? menaquinones (especially MK-4, menatetrenone). Menadione (vitamin K?) has minimal K activity. Vitamin K compounds undergo oxidation-reduction cycling within the endoplasmic reticulum membrane, donating electrons to activate specific proteins via enzymatic gamma-carboxylation of glutamate groups before being enzymatically re-reduced. Warfarin inhibits this vitamin K reduction, necessitating K supplementation during anticoagulation therapy. Along with coagulation factors (II, VII, IX, X, and prothrombin), protein C and protein S, osteocalcin (OC), matrix Gla protein (MGP), periostin, Gas6, and other vitamin K-dependent (VKD) proteins support calcium homeostasis, facilitate bone mineralization, inhibit vessel wall calcification, support endothelial integrity, are involved in cell growth control and tissue renewal, and have numerous other effects. This review updates vitamin D and K skeletal and cardiovascular benefits and evidence for their synergy of action.
PMID: 21155624
CLICK HERE for PDF
Text extracted from PDF
Review Article
Vitamins D and K as Pleiotropic Nutrients: Clinical Importance to the Skeletal and Cardiovascular Systems and Preliminary Evidence for Synergy
Parris M. Kidd, PhD
Parris M. Kidd, PhD - Cell biology; University of California, Berkeley; contributing editor, Alternative Medicine Review; health educator; biomedical consultant to the dietary supplement industry Correspondence address: 792 Sunset Avenue, Suite 10, Suisun City, CA 94585 Email: dockidd@dockidd.com
Introduction
Vitamins D and K are lipid-phase nutrients that have received intensified attention in recent years. As techniques of genomics, proteomics, and molecular biology continue to rapidly advance, the research on these nutrients has evolved from strictly nutritional toward transcriptional gene regulation, translational and post-translational protein regulation, and receptor-mediated effects. In their most active forms, both vitamins D and K are now known to be relatively pleiotropic factors, due to their diverse mechanisms and consequent broadened clinical scope that eclipses their classic vitamin effects.
This review focuses on the contributions of vitamins D and K to skeletal and cardiovascular health, including evidence that supports synergy of action. It re-examines the criteria for setting deficiency and insufficiency states and discusses the greatly expanded possibilities for supplementing vitamins D and K to improve public health.
Vitamin D: Prohormone for the Vitamin D Endocrine System
Vitamin D was discovered as a dietary constituent (from cod liver oil) that helped cure the bone disease known as rickets.1-5 In humans and other mammals, vitamin D is also made in the skin on exposure to sunshine, hence its nickname "the sunshine vitamin." Since this nutrient does not have to be strictly obtained from the diet, according to traditional definitions it is not really a vitamin, although essential for life.6-8 Vitamin D insufficiency linked to chronic diseases has become a worldwide problem.9 Whether photochemically synthesized in the skin or obtained from the diet, vitamin D is actually a prohormone, the raw material for a hormone that drives an intricate endocrine system.
Circulating vitamin D is the substrate for a two-step enzymatic transformation to a D hormone that drives the highly sophisticated vitamin D endocrine system (VDES).1 However, the classic vitamin D endocrine functions of kidney vitamin D hormone secretion, intestinal calcium absorption, parathyroid hormone secretion, and bone calcium mineralization, are now considerably broadened to encompass a great variety of pro-homeostatic contributions in potentially all tissues.
In healthy humans, most of the body's vitamin D is produced by photochemical production from 7-dehydrocholesterol in the lower epidermal zone of the skin. As ultraviolet B (UVB) irradiates the skin, 7-dehydrocholesterol becomes energized and undergoes a structural transformation.1 This molecule initially has four benzene rings - A, B, C, and D. The B ring is opened by the UVB energy and vitamin D3 is created. This is a steroid compound, technically a "seco-steroid" because the 9,10 carbon-carbon bond of the opened B ring can swivel on its axis. Along with the stereo flexibility of side chain carbon-carbon bonds, this enables the molecule to have multiple three-dimensional conformations with consequent flexibility of action on its receptors (Figure 1).
After vitamin D3 is photochemically produced in the skin, it enters the circulation. Together with vitamin D absorbed from food (whether as D3/ cholecalciferol or D2/ergocalciferol), upon reaching the liver it is subject to the action of a cytochrome-type, 25-hydroxylase enzyme (CYP27A1).1 This converts it to 25-hydroxyvitamin D or 25(OH)D, which can include 25(OH)D2 along with 25(OH)D3. These 25(OH)D molecules are circulated to the kidney, where another cytochrome-type 1alpha-hydroxylase enzyme (CYP27B1) performs another hydroxylation, producing 1alpha, 25-dihydroxyvi-tamin D3 or 1,25(OH)2D, also called calcitriol.1 This is the fully active, seco-steroid D hormone. The complex intermolecular vitamin D relationships are illustrated in Figure 2.
To facilitate the flow of this review, the prehor-mone vitamin D3 produced in the skin will be referred to simply as D3, the prohormone 25(OH) D3 (25-hydroxyvitamin D3, calcidiol) will be 25D, and the fully active hormone 1,25(OH)2D3 will be referred to as 1,25D. Vitamin D2 (ergocalciferol), the less bioactive dietary vitamin D molecule, will be called D .
Organization of the Vitamin D Endocrine System
The 1,25D hormone is the core component of a highly complex vitamin D endocrine system1 that also includes the liver, kidneys, vitamin D receptors (VDRs), and feedback mechanisms that homeostatically regulate hormone output.10 Another component of the VDES is the vitamin D-binding protein, which transports 1,25D to its target organs.11
In the healthy individual the VDES is under stringent homeostatic control, particularly in regard to circulating levels of 1,25D. Typically, its production is modulated according to the body's calcium and other endocrine needs.1 But the VDES system has other major regulatory loops:11-16 > As circulating 1,25D rises above a homeostatic threshold, it down-regulates its own synthesis in the kidney. When its levels dip, this down-regulation ceases and the kidney resumes its 1,25D biosynthesis.
Figure 1. Molecular Structure of 1alpha, 25-dihydroxyvitamin D3 (1,25(OH)2D3; calcitriol), the Fully Activated Vitamin D Hormone
Figure 2. The Absorption and Metabolic Conversion of Vitamin D
There is some evidence that the ultimate regulator of 1,25D hormonal status and the VDES is vitamin D3 from the skin or the diet. The hydroxylase that converts 25D to 1,25D in the kidney does not become rate-limited until serum 25D approaches 40 ng/mL. The liver hydroxylase has similar properties for its substrate 25D, so that essentially the more D3 that reaches the blood, the more 1,25D the kidneys can generate.1
Beyond its traditionally defined liver-kidney-intestine-bone axis, the vitamin D endocrine system extends into virtually all human tissues.15 The revelation of its multiple dimensional biological activities has created a new health paradigm for vitamin D.
The Vitamin D Endocrine System Depends on Vitamin D Receptors
Vitamin D is well known for its fundamental role in calcium and bone homeosta-sis, closely linked to PTH status; hence, the traditional name calcitriol for 1,25D. Being a seco-steroid, 1,25D resembles other steroid hormones, such as estradiol, progesterone, testosterone, cortisol, and aldosterone, by having both direct actions on genes (genomic responses) and more rapid, non-gene actions (so-called rapid responses).1,17 Both types of 1,25D responses are mediated by VDRs.
VDRs are closely related to the classic steroid-sensitive nuclear receptor located in the cell nucleus, but are also distributed outside the cell nucleus.17 VDRs bind 1,25D with high affinity, but can weakly bind 25D (0.1- to 0.3-percent as well as to 1,25D).1,18 Binding of 1,25D can occur in the cytoplasm, nucleus, or inner face of the outer cell membrane,17 to generate both genomic and non-genomic responses.1
Besides serving as 1,25D effectors, VDRs also help manage the balance between bioactivation and degradation of 1,25D by direct feedback on the associated enzymes.17 This is crucial to the homeostasis of the VDES.
From: Peterlik M, Boonen S, Cross HS, Lamberg-Allardt C. Vitamin D and calcium insufficiency-related chronic diseases: an emerging world-wide public health problem. Int J Environ Res Public Health 2009;6:2585-2607. http://www.mdpi.com/1660-4601/6/10/2585/. Used with permission
The Vitamin D Receptor Molecular Ensemble
VDRs are essentially nuclear transcription factors, able to bind directly to stretches of DNA and thereby turn specific genes on or off.17 It has been estimated that the VDR can regulate as many as 500 of the approximately 20,488 genes in the human genome.22 This genome-level versatility of VDRs, coupled with their widespread distribution in the tissues, along with the enzyme that converts 25D to 1,25D, is consistent with the pleiotropic character of vitamin D.
In their inactive state, VDRs are typically located in the cell cytoplasm and on "caveolae," which are infoldings of the outer cell membrane.23 As a 1,25D molecule encounters a VDR, a 1,25D-VDR "ligan-ded complex" is formed.17 This triggers the VDR protein to undergo conformational (shape) changes, which in turn changes its interactions with transport proteins and other cell proteins. The complex may stimulate functional changes at its caveolar location, elsewhere in the cytoplasm, or after translocation to the cell nucleus. There the complex comes into contact with proteins of the gene transcription machinery and activates or deactivates specific genes associated with these proteins.1,17
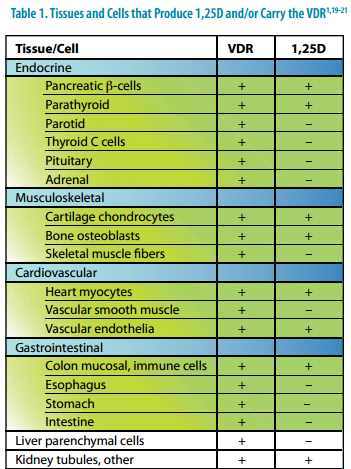
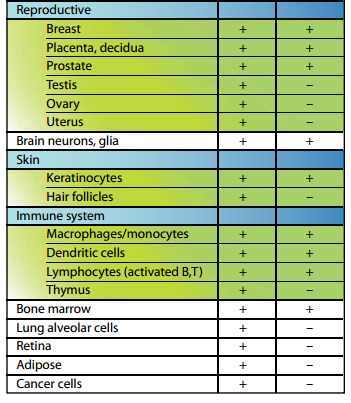
VDRs likely mediate all the classic endocrine actions of 1,25D.17 Their quantity diminishes with age24 and with deterioration of kidney function.25 But the extensive "extra-renal" distributions of VDRs signal a far more global involvement of the VDES in human health than was previously understood. As listed in Table 1, a minimum of 35 cell types carry VDRs and therefore have the potential to produce biological "D hormone" responses, depending on the availability of 1,25D. At least 17 cell types also carry the 1alpha-hydroxy-lase enzyme that converts 25D to 1,25D.
The brain (including the hippocampus26), parathyroid, pancreas (beta-islets), musculoskeletal system, cardiovascular system, gastrointestinal system, kidney, many reproductive tissues, skin, bone marrow, and various cells of the immune system, all possess the capacity to make 1,25D and respond to it with their respective VDRs (Table 1). This scenario is consistent with 1,25D being an autocrine, paracrine, and even an intracrine hormone messenger.27
Table 1. Tissues and Cells that Produce 1,25D and/or Carry the VDR1,19-21
Local Action Scenarios for the Vitamin D Receptor
Hormones most typically circulate with the blood and act on target cells in organs some distance from where they are secreted. But some hormones can act close to where they are produced, sometimes without having to use the circulation.27 An autocrine effect occurs when the hormone/ messenger exits the cell wherein it was produced, then influences that same cell from the outside; a paracrine effect involves influencing cells in the immediate area, without reliance on the circulation for transport; and an intracrine effect occurs when the messenger acts within the same cell that produced it, without first having to exit the cell. The evidence suggests 1,25D likely has all three of these actions.
Intracrine effects for 1,25D are apparent in the immune system. Macrophages have intracrine 1,25D-VDR loops, facilitated by intracellular proteins.5 The cell picks up 25D from the outside, transforms it to 1,25D on the inside (probably in mitochondria), and transfers the 1,25D into the nucleus. There it stimulates intricate gene multiplication effects that are unique to higher primates and facilitate antibacterial immunity, specifically against Mycobacterium tuberculosis. Cannell and Hollis, in their 2008 article in this journal,28 recognized this as a key advance in understanding immunity.
Other Receptors Can Influence the Vitamin D Endocrine System
The steroid and xenobiotic receptor (SXR) is a nuclear receptor evolutionarily related to the VDR.29 It is responsive not just to endogenous steroids and circulating hormones, but to xenobi-otic compounds, including many pharmaceutical agents. The SXR has been dubbed a "xenobiotic sensor" because it is so responsive to xenobiotics.30 This receptor may be a link between certain pharmaceutical drugs and catastrophic loss of bone mineral density (BMD).
Long-term therapy with antiepileptic drugs, such as phenobarbital, phenytoin, and carbamaze-pine, or the antimicrobial agent rifampicin, can cause the metabolic bone disease osteomalacia.29,31 Phenobarbital activates the SXR, which consequently down-regulates CYP2D25, another cytochrome enzyme that has 25-hydroxylase activity and is involved in 1,25D biosynthesis.32 Down-regulation of 1,25D availability by this SXR activation can account for drug-induced osteomalacia.
The SXR also may derange 1,25D metabolism via "crosstalk" with VDR, at least in the kidney, liver, and intestine.29 This has been shown to influence the VDR to promote 1,25D breakdown in the liver. Such SXR-VDR crosstalk could be another, less direct means for either xenobiotics or endogenously produced molecules to influence the VDES.
The membrane associated, rapid response, steroid-binding (MARRS) protein is a newly discovered catalytic protein located at the outer cell surface and able to bind with 1,25D.33 Whether it is a true VDR remains to be determined.
Vitamin D Importance for Bone Health and Fracture Prevention
Bone health rests on the attainment of dense bone matrix and adequate bone mineralization by young adulthood.34 Maximum bone mass is typically achieved in young adults by age 18-25. Past age 40, the balance between bone removal and replacement (called "bone remodeling") tends to shift toward net bone removal.35 As bone loses density, the risk for osteoporosis increases, and with it a heightened risk for bone fracture.
The importance of vitamin D for bone health has been recognized since it was used to eliminate rickets in the 1930s.2 Vitamin D sufficiency is crucial to mobilizing adequate calcium into bone. When vitamin D is sufficient, intestinal calcium absorption can reach 30-40 percent of the dietary intake; but lacking adequate vitamin D the body absorbs no more than 10-15 percent of dietary calcium.2 Knockout mice lacking the VDR develop osteomalacia, which can be reversed using a diet with increased calcium.36
Numerous observational studies, prospective randomized controlled trials (RCTs), and a series of meta-analyses, demonstrate supplementation with vitamin D and calcium reduces the risk for frac-ture.37,38 Those few trials that did not show benefit from vitamin D plus calcium had poor compliance or otherwise failed to achieve a minimum serum 25D level of 30 ng/mL.39-41
The latest meta-analysis reanalyzed raw patient data for 68,500 patients from seven major vitamin D fracture trials in the United States and Europe.37 From extensive analyses, it can be concluded that vitamin D with calcium reduces overall risk of fracture by a maximum 18 percent (hazard ratio 0.82; 95% CI 0.67-0.99; p=0.045).
Vitamin D also Protects against Fracture by Helping Prevent Falls
Vitamin D helps prevent falls by supporting skeletal muscle health. Skeletal muscle weakness (myopathy) is a prominent feature of vitamin D deficiency and likely causes impairment even before adverse bone effects occur.42 This myopathy frequently causes gait instability and can sometimes be reversed by repleting vitamin D.2 Muscle tissue carries VDRs, and mice lacking the VDR show a skeletal muscle phenotype with smaller and variable muscle fibers.43
In humans, correction of vitamin D deficiency also frequently improves postural and dynamic balance, both independent predictors of vulnerability to fall.44 In double-blind RCTs, vitamin D supplementation increased muscle strength and balance and reduced the risk of falling.45
Fracture Risk, Vitamin D, and Autoimmune Conditions
The autoimmune diseases rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE) both are associated with vitamin D deficiency and increased risk of fracture. Glucocorticoid drugs that are frequently used to treat these diseases add further to the risk of fracture, especially when their use is continued beyond three months. Such patients should be closely monitored and their vitamin D supplementation adjusted as required.
Higher vitamin D intake is associated with a decreased incidence of RA.46 Among SLE patients the prevalence of vitamin D deficiency is as high as 67 percent.47 In these patients, renal disease, photosensitivity, and African American decent are strong predictors of low 25D levels (<10 ng/mL).2 Physicians should consider checking 25D status frequently in these patients, especially in those with osteoporosis or other risk factors for falls.
The current knowledge on vitamin D and bone health supports increasing serum 25D to levels above 30 ng/mL. For people with other risk factors for osteoporosis or bone fracture, such as advancing age, achieving a serum 25D of at least 45 ng/ mL would seem prudent.
Vitamin D is Essential to Cardiovascular Health
Vitamin D is crucial for cardiovascular health at all life stages. Vitamin D deficiency is linked to life-threatening heart failure in infants.48 In early childhood, vitamin D deficiency is associated with cardiomyopathy and congestive heart failure.49 In adults, low circulating 25D levels correlate with congestive heart failure.50 Vitamin D insufficiency has been correlated with greater mortality from cardiovascular disease8,51-55 and stroke.56
Vitamin D insufficiency has also been correlated with cardiovascular risk factors such as obesity and metabolic syndrome, as well as cardiovascular conditions such as angina, coronary insufficiency, myocardial infarction, and transient ischemic attack.57 In the most recent National Health and Nutrition Examination Survey (NHANES) that covered 2000-2004, serum 25D <20 ng/mL was associated with increased prevalence of self-reported coronary heart disease, heart failure, and peripheral vascular disease.58,59
Evidence from epidemiological studies suggests that a higher range of 25D serum concentration is linked to lower risk for cardiovascular-related death (reviewed in Barnard, 201060). Giovannucci et al analyzed data on 18,225 men from the Health Professionals Follow-up Study and found a 2.4-fold increased risk of myocardial infarction for individuals with serum 25D below 15 ng/mL, compared to those above 30 ng/mL (95% CI 1.53-3.84).61 Pilz et al followed, for an average 7.7 years, a cohort of 3,299 patients who were routinely referred for coronary angiography at baseline.54 When patients with serum 25D <10 ng/mL were compared to patients with levels >30 ng/mL, their hazard ratio (which approximates relative risk) for death due to
heart failure was 2.84 (95% CI 1.20-6.74) and for sudden cardiac death was 5.05 (95% CI 2.13-11.97).
In contrast to the robust epidemiological evidence that vitamin D insufficiency increases cardiovascular risk, evidence that vitamin D supplementation can reduce cardiovascular risk is only tentative. Wang et al analyzed 17 prospective
studies and RCTs conducted from 1996 to 200962
and found that five prospective studies of patients receiving dialysis and one study involving a general population showed consistent reductions in cardiovascular disease mortality among adults who received vitamin D supplements. There was a slight reduction in cardiovascular disease risk (pooled relative risk 0.90) with vitamin D supplementation at doses averaging 1,000 IU/day that fell just short of statistical significance (95% CI 0.77-1.05). From their data, vitamin D plus calcium supplementation or calcium supplementation alone showed no evidence of benefit.
Vitamin D Status and Hypertension
Epidemiological studies suggest vitamin D insufficiency is associated with higher risk for hypertension,63 and that patients with hypertension and low 25D levels have higher risk for adverse cardiovascular events.7,8
In a four-year prospective study that involved subjects from both the Health Professionals Follow-up Study and the Nurses' Health Study, Forman et al64 reported a relative risk for incident hypertension of 3.18 for individuals with 25D levels <15 ng/mL, relative to those with levels >30 ng/mL. In the Framingham Offspring Study,57 with 5.4 years of follow-up, hypertensive subjects with serum 25D <15 ng/mL were 53-percent more likely to experience a cardiovascular event than those with serum 25D above that level. Subjects with values <10 ng/mL were 80-percent more likely to have a cardiovascular event.
The evidence for vitamin D supplementation against hypertension is less impressive. A 2009 systematic review and meta-analysis of eight randomized, controlled trials, which supplemented vitamin D to subjects with mean blood pressure (BP) >140/90 mmHg at baseline,63 found a small but statistically significant reduction in diastolic BP. A small reduction in systolic BP was also found, but failed to reach statistical significance. In the NHANES III (1988-1994),65 16,135 non-institutionalized men and women, mostly over age 50, were tested for systolic BP and serum 25D levels. In Caucasian men and women, levels of serum 25D <20 ng/mL were significantly associated with higher systolic BP. Approximately 61 percent of the whites and 92 percent of the blacks in this study had lower than the then-suggested optimum level of serum 25D (<32 ng/mL).
The NHANES III findings were supported by findings from two RCTs.66,67 One of these trials measured serum 25D and found that a 25D increase from 20 to 60 ng/mL was associated with a significant reduction in systolic BP (6 mmHg) after six weeks of treatment.67
Animal studies suggest 1,25D is a homeostatic endocrine regulator of BP, very likely via the renin-angiotensin system.68 Clinical evidence in support of this mechanism is currently limited to one Japanese case study.69
Protection against Mortality from Chronic Kidney Disease (CKD)
To date, the clearest indications that orally supplemented vitamin D can have cardiovascular benefit come from intervention trials involving patients with chronic kidney disease. Although serum 1,25D is normally tightly regulated,1 the ability of the proximal tubules to make 1,25D deteriorates as the kidneys fail, leading to eventual decline of circulating 1,25D.25
Patients with CKD on dialysis have increased risk for death if they are vitamin D deficient.70 Low serum 1,25D levels cause an increase in PTH secretion due to compensatory feedback, and secondary hyperparathyroidism can develop, which is a known mortality risk factor for patients on dialysis.19 In these patients low circulating 1,25D is also linked to ventricular hypertrophy, which at times can be ameliorated by treatment with vitamin D3.71
A 2010 meta-analysis of four prospective vitamin D trials with CKD patients concluded that mortality was significantly lower for patients who received oral vitamin D3 compared to those who did not.62 Although it has been customary to administer 1,25D to dialysis patients parenterally following dialysis, Verhave and Siegert asserted that oral treatment with 1,25D appeared to be equally as effective in reducing mortality risk and far less expensive.19
Mechanisms for Vitamin D Cardiovascular Benefits
The heart and circulation are likely paracrine components of the vitamin D endocrine system. Because cardiac muscle cells and vascular endothelial cells carry the 1alpha-hydroxylase enzyme that converts circulating 25D to 1,25D, these tissues have local capability to activate vitamin D.20,21 In addition, VDRs are widely distributed in muscle cells, vascular endothelial cells, and vascular smooth muscle.20,21,60 "VDR knockout mice" that lack the VDR show cardiovascular abnormalities, such as hypertension and left ventricular hypertrophy, and their cardiac muscle cells develop contractile abnormalities.13,72 Wu-Wong et al identified 176 genes in human coronary artery smooth muscle cells that are sensitive to 1,25D, including genes involved in regulating smooth muscle cell growth, endothelial degeneration, thrombus initiation, and fibrinolysis.73
Vitamin D could have clinical anti-inflammatory benefits. Schleithoff et al randomized 93 subjects with systolic dysfunction to receive either vitamin D2 (ergocalciferol, 2000 IU) plus calcium (500 mg) or placebo plus calcium (500 mg) daily.74 Baseline vitamin D concentrations were below the normal range in both groups (14.4 and 15.3 ng/mL in the treatment and placebo groups, respectively). After nine months, the vitamin D plus calcium group had significantly greater increases in 25D concentrations (from 14.4 to 41.2 ng/mL) than did the placebo group (from 15.3 to 18.9 ng/mL; p=0.001). Concentrations of tumor necrosis factor-alpha, a typically pro-inflammatory cytokine, decreased in the vitamin D-supplemented group and increased in the placebo group (p=0.006).
It has been suggested, mainly from in vitro evidence, that another plausible vitamin D/ cardiovascular mechanism is inhibition of pathologic blood vessel calcification.19 Arterial wall calcification leads to stiffening of the wall and loss of elasticity, with adverse functional effects74 that correlate with adverse clinical cardiac events.75 This correlation between arterial calcification and increased risk for cardiovascular mortality is especially documented for patients with stage 3 to 5 CKD.76 However, a recent study of 140 CKD patients found that vitamin D deficiency lowers survival independently of vascular calcification.77 One study that sheds light on this issue was conducted with CKD children on dialysis.78 Their carotid intima-media thickness and calcification scores showed a U-shaped distribution across 1,25D levels: patients with both low and high 1,25D had significantly greater intimal thickness (p<0.0001) and calcification (p<0.0002) than those with normal levels. It seems both abnormally low and abnormally high 1,25D levels can facilitate adverse calcium-phosphate homeostasis.
Vitamin D Deficiency, Insufficiency, Sufficiency, and Repletion
Most experts seem to accept that serum 25D is the best single indicator of systemic vitamin D status, and this position has been endorsed by the Institute of Medicine of the U.S. National Academy of Sciences, which is responsible for making intake recommendations.79 The vitamin D prohormones D3/cholecalciferol and D2/ergocalciferol are both difficult to measure because of their hydrophobic nature (very poor miscibility with water), and 1,25D serum levels have little discriminative value because they are so homeostatically regulated.1
The serum level of 25D is most often expressed as ng/mL, and less commonly as nM/L. This review will uniformly employ the ng/mL measure. To convert from nM/L values to ng/mL, divide by 2.496.1
Evidence-based Definition of Vitamin D Sufficiency
There is no consensus on what ranges of serum 25D levels constitute vitamin D deficiency, insufficiency, and sufficiency. Although as recently as 2007 leading researchers often defined serum 25D levels for deficiency at around 10-12 ng/mL, with up to 20-30 ng/mL considered insufficient and >30 ng/mL considered sufficient,1,80,81 some researchers are calling for higher levels. But even by these current standards vitamin D deficiency is widespread in pregnant women and newborn infants, as discussed by Cannell and Hollis in a 2008 review in this journal.28 They also noted that rickets, the archetype vitamin D deficiency, is again on the rise.
Assuming that serum 25D levels reflect functional vitamin D status, another approach to determining vitamin D deficiency, insufficiency, and sufficiency would be to tabulate the serum 25D levels at which particular positive and negative effects are documented to occur.
Below are reliable data culled from representative human studies:
Serum 25D <8 ng/mL: classic vitamin D deficiency - rickets or osteomalacia79
Serum 25D <17.8 ng/mL: increased risk for all-cause mortality7
Serum 25D <24 ng/mL: greater risk for death in patients receiving intensive care in Australia;
- patients had three times greater mortality rate than those with serum 25D >60 ng/mL82
Serum 25D 30 ng/mL: greater risk for depression among hospitalized subjects; control subjects averaged 43.6 ng/mL (p<0.02)83
Serum 25D 32 ng/mL: threshold for optimal calcium absorption from the intestine84
Serum 25D 38 ng/mL: threshold for optimal neuromuscular performance85
Serum 25D 38 ng/mL: 18-percent lower risk for all cancers in postmenopausal women supplemented with D386
Serum 25D >40 ng/mL: 40-percent lower risk for colorectal cancer diagnosis in Europe, compared with serum 25D <11 ng/mL87
Serum 25D 45 ng/mL: lowest risk for fracture prevention, from a linear relationship between increasing 25D levels and lowering levels of risk in a meta-analysis88
In 2005 the level of 25D required for sufficiency was suggested to be 33-80 ng/mL.4 Considerable new data accrued since then argues for a higher minimum - above 40 ng/mL. Perhaps the best perspective on this pivotal issue comes from the large 2009 meta-analysis of vitamin D for fracture prevention, conducted by Bischoff-Ferrari et al.88 Their meta-analysis, comprised of 20 double-blind RCTs on 83,165 subjects, found fracture risk increased linearly with serum 25D levels up to 45 ng/mL (112 nM/L). This sets the highest level of serum 25D documented for vitamin D efficacy. These researchers suggested the actual optimum level for fracture prevention could be even higher.45
Vitamin D Deficiency: Life-Threatening for the Sick and Vulnerable
Vitamin D deficiency can be life-threatening. Serum 25D lower than 17.8 ng/mL has been linked to increased all-cause mortality.7 Conversely, repletion via supplementation can lower mortality risk, as concluded from a 2007 meta-analysis.6
A meta-analysis of 18 U.S. or European RCTs evaluated vitamin D supplementation on health outcomes such as fractures, BMD, falls, and colorectal cancer incidence;6 all trials also reported mortality. The mean vitamin D supplementation (D3 or D2) was 528 IU daily and mean follow-up was 5.7 years. The relative risk for all-cause mortality was 0.93 (95% CI 0.87-0.99), indicating a seven-percent reduced mortality risk.
Vitamin D insufficiency is a major health problem among hospitalized patients and institutionalized elderly subjects. An evaluation of 290 consecutively admitted patients found that 57 percent were severely vitamin D deficient (25D <15 ng/mL).89 In parts of Europe, most community dwelling elderly also have inadequate 25D levels.90 For patients in intensive care in Sydney, Australia, Lee et al found 17 percent had undetectable serum 25D, and fully half were deficient or insufficient (serum 25D <24 ng/mL).82 They calculated that mortality rate was three times higher in those with <24 ng/mL compared to those who were considered 25D-sufficient (>60 ng/mL).
From their extensive experience with critically ill patients, Lee et al hypothesized that vitamin D deficiency or insufficiency may critically worsen organ dysfunctions that are less severe in the non-critically ill population.91,92 Hypocalcemia, which is rare in non-critically ill patients due to multiple homeostatic control mechanisms, is common among critically-ill patients and typically does not respond to parenteral calcium supplementation. They also linked vitamin D deficiency in the critically ill to immune impairments, the systemic inflammatory response syndrome, cardiogenic shock, impaired microcirculation, and other life-threatening complications.82
Cannell and Hollis discussed multiple factors that contribute to vitamin D deficiency.28 It is well established that incidence of vitamin D deficiency is greater in higher latitudes of both the northern and southern hemispheres. As examples, Boston, MA, has a four-month "vitamin D winter," while in northern Canada and Europe this can reach six months. Those who avoid sunlight are at risk any time of the year, at whatever latitude they live.28 Also at higher risk are darker-skinned individuals, as skin melanin is an effective sunblock against UVB; the elderly, who have less 7-dehydrocholes-terol in the skin and make much less vitamin D from any given amount of sunlight than do 20-year olds; and overweight and obese individuals, since body fat removes vitamin D from the circulation.
Safe and Effective Vitamin D Repletion
The wave of positive findings on new clinical applications for vitamin D has created a surge of support for increasing the recommended dietary intakes. Bischoff-Ferrari et al suggest, from their extensive meta-analyses, for effective fall and fracture prevention, cardiovascular health, and colorectal cancer prevention, mean serum 25D levels of 30-44 ng/mL may provide optimal benefits.45,88,93 This range of levels was achieved in RCTs with oral daily doses of 1,800-4,000 IU vitamin D.
The current U.S. intake guidelines for vitamin D were developed by the Food and Nutrition Board of the Institute of Medicine of the U.S. National Academy of Sciences in 1997 and have not been revised since then.79 A working group of U.S. and Canadian government experts has called for them to be revised.94 Developed as Adequate Intakes (AI), the 1997 guidelines recommend 5 mcg/day (200 IU) from birth to age 50 years, 10 mcg/day (400 IU) from age 51-70, and 15 mcg/day (600 IU) age 71+.79 The AI is "believed to cover the needs of all individuals in the group, but lack of data prevent being able to specify with confidence the percentage of individuals covered by this intake." This group also set Tolerable Upper Intake Levels (ULs) at 25 mcg/ day (1,000 IU) for the first year of life, then 50 mcg/day (2,000 IU) above age one year. The UL is the "maximum level of daily nutrient intake that is likely to pose no risk of adverse effects.”
Few foods contribute substantial vitamin D to the diet. Oily fish lead the list, including (roughly in the order of highest to lowest D3 content) catfish, salmon, mackerel, sardines, tuna, and eel, followed by eggs, beef liver (cooked), fish liver oils (e.g., cod liver oil), butter, and red meat.3 A 100-g snack of cooked salmon could provide 360 IU, but should preferably be from wild caught fish, since farmed salmon can contain as little as one-quarter the vitamin D of wild fish.95
Mushrooms are the only substantial vegan source of vitamin D2.96 Many countries allow or even encourage foods to be fortified with vitamin D (usually D3). In the United States, only milk is required to be fortified. The 2008 U.S. total daily intake of vitamin D (including reported supplement use) was estimated to be slightly over 320 IU, with the highest 20 percent averaging less
than 400 IU.3
The Safety of Supplemental Cholecalciferol
The versatility of action established for 1,25D hormone also means it has the potential to profoundly influence function in virtually all human tissues. At supra-physiological levels, 1,25D could possibly have unintended adverse effects. Fortunately, there is a large window of safety for vitamin D supplementation.
According to Heaney, controlled metabolic studies with D3 found that dosages up to 50,000 IU per day for up to five months produced neither hypercalcemia nor hypercalciuria.84 Hathcock et al could find no reported cases of vitamin D intoxication from daily intakes of 30,000 IU per day for extended periods, nor any intoxication from serum 25D levels up to 200 ng/mL.97 They concluded that a 10,000 IU daily intake should be the safe Tolerable Upper Intake Level (formally abbreviated UL) - five times the UL set by the U.S. government in 1997.79
In 2004, a human pharmacokinetic study found ergocalciferol or "vitamin D2" was less than one-third as effective as D3 for raising serum 25D levels.98 Also, human skin when exposed to sunlight does not make any detectable D2.1 In 2008, the veteran vitamin D researcher A.W. Norman suggested that oral and injectable vitamin D2 be phased out, especially since vitamin D3 is less costly and is widely available.1
The Vitamin K Metabolic System
As with vitamin D, basic and clinical research on vitamin K has markedly accelerated within the past decade. Originally discovered as an anti-hemor-rhagic factor (K for Koagulation),99 vitamin K's activity is now known to encompass a variety of physiological processes.99-101 Beyond its well recognized essentiality for activating the blood coagulation proteins, this vitamin helps regulate tissue calcium content99,100 and has growth-regula-tory,102,103 anticancer,104 and anti-inflammatory effects.105 Vitamin K also has potent antioxidative properties101 and can regulate gene activity by binding with a specific receptor.106
Vitamin K is actually an umbrella term for a number of nutrients, all of which are 3-substituted 2-methyl-1,4-naphthoquinones. Phylloquinone (vitamin K1) contains a saturated, phytyl side chain and is produced in algae and the higher plants.107
The menaquinones (MKs; collectively vitamin K2) are of microbial origin, whether produced in the gut or from other fermentation.107 They carry multiple, partially unsaturated isoprenyl groups that vary in number from 1 (MK-2) to 14 (MK-14) (Figure 3). Menadione (formerly called "vitamin K3") is a form that lacks isoprenyl groups, has minimal vitamin K activity, and has potential for toxicity.108
Dietary Sources of Vitamin K
The adequate U.S. intake for vitamin K is established at 90 mcg/day for women and 120 mcg/ day for men, based on old estimates (1994) of median intakes from foods;109 most of this comes from vitamin K1.107 Green leafy vegetables and crucifers are by far the best source of K1, followed by variable contributions from vegetable oils (soybean, canola, cottonseed, olive), then smaller amounts from peas, beans, tomatoes, and carrots. Certain population subgroups appear to be at risk for low K1 intakes, including children and the
elderly.100,107
Menaquinones (collectively vitamin K2) are produced by the human gut flora, but very little of this material is actually absorbed (via the lower bowel).100,107 Menaquinones come from animal products (meat, egg yolk, butter, cheeses) and from legumes such as soybeans.107 The traditional Japanese food natto, produced by Bacillus subtilis fermentation of soybeans, is rich in MK-7.100 Cheese supplies menaquinones, mainly MK-4 through MK-9, and is a substantial source of K2 for some populations.100
Vitamin K Oxidation-Reduction Cycling Activates Vitamin K-Dependent Proteins
Metabolically, vitamin K goes through a cycle of oxidation followed by reduction that drives protein carboxylation (Figure 4). The fully reduced vitamin K (the hydroquinone form) donates a pair of electrons to gamma-glutamyl carboxylase (GGCX) to enable this enzyme to carboxylate selected proteins at targeted glutamate groups along their peptide chains. The resultant oxidized vitamin K is subsequently recycled to the reduced hydroqui-none, primarily by the enzyme vitamin K oxidore-ductase (VKOR), using electrons mainly drawn from NADH (nicotinamide adenine dinucleotide, reduced).99 When this VKOR recycling enzyme is blocked by warfarin or other coumarins, coagulation activity and other vitamin K-dependent activity is also blocked.110 Vitamin K recycling is
Figure 3. Structures of Vitamin K (Phylloquinone) and Vitamin K2 (Menaquinones)
crucial to its biological action, because very little is stored in the body.100
The vitamin K cycle occurs in the rough endoplasmic reticulum membranes of cells.110 The major organ for vitamin K storage and metabolism is the liver, where the main GGCX activity is to carboxyl-ate coagulation-related proteins.99 Another significant organ with vitamin K activity is bone, wherein osteocalcin and other bone proteins are gamma-carboxylated. But the vitamin K cycle actually is functional in virtually every tissue and (as the inventory of vitamin K-dependent proteins expands) is known to be involved with physiological effects as diverse as bone mineralization, calcium homeostasis, cell growth control, apopto-sis, chemotaxis, and cell level signal transduction, in addition to its classic roles in hemostasis.110
Vitamin K-dependent Proteins Support Calcium Homeostasis
Proteins that become gamma-carboxylated with vitamin K as cofactor are aptly termed vitamin-K dependent (VKD) proteins.110 Specific glutamyl amino acid residues along their peptide chains become gamma-carboxylated in the cell's rough endoplasmic reticulum during or just subsequent to the protein's translational synthesis from its messenger RNA. Such "Glu" residues once gamma-carboxylated are designated "Gla" (Figure 4). The specific distribution of gamma-carboxyglutamyl (Gla) residues on a VKD protein modifies its three-dimensional shape and thereby induces a functional transformation. The molecule becomes activated, with its new Gla residues usually having strong calcium-binding activity.99,111
To date some 14 VKD proteins have been clearly identified. The most classic are those that influence blood coagulation (coagulation factors II, VII, IX, and X, prothrombin, protein C, and protein S).110,112 Osteocalcin (OC) and matrix Gla protein (MGP) are involved in the mineralization of bones and teeth, periostin is involved in extracellular matrix homeostasis (including in bone), and Gas6 is involved in endothelial homeostasis.110,113 In the case of several other VKD proteins, precise functions are still unknown.114
Osteocalcin is produced by osteoblasts during bone formation, is the most abundant protein in bone after collagen,110 and is indispensable for bone mineralization. Fully carboxylated OC is positioned within hydroxyapatite and binds calcium strongly to consolidate calcification of the hydroxyapatite crystal lattice. When undercarbox-ylated, the hydroxyapatite-binding capacity of osteocalcin plummets. Osteocalcin's production is regulated by retinoic acid, estrogens, glucocorticoids, and 1,25D.99,110
MGP is the VKD protein most closely linked to blood vessel wall health. It operates predominantly in the extracellular matrix of soft tissues (vascular, heart, lung, kidney, cartilage) to down-regulate calcium deposition.99 MGP most likely inhibits vascular calcification by directly binding with calcium ions to sequester them and thereby restrict their incorporation into the extracellular matrix.115 In humans, an MGP gene mutation causes abnormal cartilage calcification (Keutel syndrome) and often arterial calcification as well.116,117
Gas6 (named for its gene, growth arrest-specific gene 6) has homeostatic support functions, growth factor properties, modulates inflammation, and facilitates immune disposal of dead cells.118 Gas6 is also linked to down-regulation of atherosclerotic plaque formation.119
Periostin is a VKD protein that occurs in collagen-rich connective tissues, including bone.110 It carries a record 16 Glas per molecule and is produced in bone marrow mesenchymal stromal cells, which are stem cells capable of differentiating into osteoblasts, chondrocytes, and adipocytes.120 Periostin is associated with the extracellular matrix, where it plays a role in mineralization, but also contributes to the primary development and ongoing modeling of periodontal ligaments, trabecular bones, and heart valves.121 The VKD proteins have broad scopes of action that continue to expand as research progresses.
Assessing Vitamin K Deficiency and Sufficiency
Vitamins K1 and K2 can be directly measured in the blood or urine; however, their levels do not seem to correlate with vitamin K-dependent functions, rendering the clinical relevance of these measurements doubtful.109,122 The classic test for human vitamin K deficiency has been functional: abnormally long prothrombin time. This test is relatively insensitive, however, because prothrom-bin can be 50-percent less active before a value is considered out of the normal range.122 Also, prothrombin functionality may not be representative of the functionality of the non-hemostatic VKD proteins. Accurate assays for undercarboxyl-ation of VKD proteins, such as osteocalcin, have been developed and should help determine vitamin K intakes.
Figure 4. Oxidation/Reduction of Vitamin K Drives Protein Carboxylation
Fully reduced vitamin K (hydroquinone) donates a pair of electrons to facilitate the enzymatic carboxylation of specific proteins, then the oxidized form (quinone) is enzymatically re-reduced using an electron pair from NADH.
When vitamin K is deficient, biologically inactive, undercarboxylated forms of the vitamin K-dependent coagulation factors appear in the blood - protein induced by vitamin K absence or antagonism (PIVKA). Prothrombin (Factor II) corresponds to PIVKA-II. Sensitive immunoassays are available to measure PIVKA-II in plasma. Studies using these immunoassays tentatively suggest that phylloquinone intakes of less than 10 mcg/day are associated with abnormal PIVKA-II concentrations (greater than 2 ng/mL plasma); whereas, 100 mcg phylloquinone/day is associated with normal PIVKA-II.123
Serum undercarboxylated OC (ucOC) is a sensitive indicator of vitamin K status and correlates with plasma PIVKA-II concentrations (r=0.27, p>0.001).122 Circulating ucOC is significantly increased in elderly women and correlates with poor vitamin D status, which supports biochemical findings that vitamin D can up-regulate the biosynthesis of OC.110
Vitamin K, Bone Health, and Fracture Prevention
Vitamin K1 and Bone Health
The relationship between vitamin K1 and bone health has been well investigated, but with equivocal outcomes, as recently reviewed in Booth 2009.100 In eight observational studies, plasma levels of K1 or its dietary intake levels were consistently correlated with significantly lower fracture risk, although without showing positive effects on BMD. Of the five prospective RCTs conducted with K1, only two of them tracked fracture risk and one of these found benefit.124
This double-blind Canadian trial recruited 440 women with osteopenia and randomized them to 5 mg K1 or placebo daily for a minimum of two years.124 After two years, significantly fewer women in the vitamin-K group had experienced fractures, but BMD was not significantly improved over placebo.
Likewise, only one of the five prospective RCTs reviewed by Booth in 2009100 found that K1 improved BMD. This two-year trial of women older than 60 years tracked bone quality at several sites.125 BMD and bone mineral content significantly improved at the distal radius but not at other sites, and only in the intervention group that received vitamin D3 (400 IU/day) and calcium
(1,000 mg/day) in addition to K1 (200 mcg/day).
The groups that received the same levels of K1 alone, or D3 and calcium alone, showed no bone gain at any site.
Menaquinone-4 Effectively Improves Bone Quality
MK-4 has been studied extensively as a treatment for osteoporosis, usually at 45 mg/day (most often 15 mg three times daily), an amount that cannot be attained from the diet.100 A 2005 review by Plaza and Lamson in this journal covered 12 trials conducted with K2 against osteoporosis of various etiologies - postmenopausal, pharmaceutically induced, and associated with conditions including Parkinson's disease, biliary cirrhosis, stroke, and anorexia.126 It concluded that MK-4 slows bone loss, boosts bone formation, and has "a more powerful influence on bone than vitamin Kr" Six of these trials were included in a 2007 meta-analysis that produced impressive statistics for reduced bone loss by MK-4.127
This meta-analysis by Cockayne et al127 of RCTs, conducted with K1 or K2 (as MK-4) on bone density and fracture prevention, identified 13 RCTs with data on bone density, of which seven also reported fracture data. Pooling the seven trials with fracture data, they found odds ratios (OR) strongly favoring MK-4 for fractures:
Hip fractures: OR 0.23 (95% CI 0.12-0.47)
Vertebral fractures: OR 0.40 (95% CI 0.25-0.65)
Nonvertebral fractures: OR 0.19 (95% CI 0.11-0.35)
These data strongly support an interpretation that MK-4 conserves bone quality and thereby markedly lowers the risk of fracture. However, the meta-analysis127 was subsequently criticized for including one trial that allegedly biased its outcome in favor of MK-4,128 and for excluding another trial that included 4,000 subjects and could have swung the outcome against MK-4.129 In addition, all seven trials were conducted with Japanese subjects so may not necessarily extend to all population groups.
A 2007 three-year, randomized trial conducted in the Netherlands tested MK-4 at 45 mg/day versus placebo on 325 healthy, postmenopausal women.130 MK-4 did not improve bone quality at all the measured sites, but did significantly improve femoral neck width (by 1.5%; p<0.05 versus placebo). MK-4 also significantly lessened the three-year loss of bone mineral content in the femoral neck and significantly conserved the three bone strength indices - compression strength, bending strength, and impact strength - all measured at the femoral neck.
A 2009 randomized trial conducted in the United States also tested MK-4 (45 mg/day) on healthy postmenopausal women, this time versus placebo or K1 (1 mg/day).131 No significant benefit was observed on femur or other bone structure indices for either K1 or K2/MK-4. This trial had at least two notable differences from the 2007 Dutch trial: it lasted for just one year and subjects in all groups received vitamin D (400 IU/day) and calcium (630 mg/day as calcium citrate) throughout the study.
Natto, a traditional Japanese fermented soybean preparation, is highly enriched in vitamin K2 as MK-7. Japanese who consume high amounts of natto have higher circulating MK-7 and lower levels of undercarboxylated osteocalcin than citizens of other countries.132 Epidemiological and cohort studies reported correlations between higher natto intake in Japan and lowered incidence of hip fracture or increased hip BMD.133-135 However, because natto also provides a substantial amount of soy isoflavones, a direct vitamin K effect from this food cannot be assumed.136
A 2009 one-year, double-blind RCT conducted in Norway found natto provided no protective effect against bone loss in early menopausal women.137
But a 2010 Norwegian double-blind RCT, using 180 mcg/day MK-7, found significantly improved lumbar BMD in subjects who had just previously undergone lung transplantation.138
Taken together, the data on vitamin K for bone health suggests K1 is not consistently beneficial but that K2 as MK-4 is beneficial at relatively high intakes (45 mg/day). Concerning K2 as MK-7, there is not sufficient prospective data to draw firm conclusions.
Vitamin K and Cardiovascular Health
Vitamin K2 appears to be important for cardiovascular support, especially blood vessel wall integrity.139-145 In a recently published observational study,140 16,057 postmenopausal Dutch women reported their vitamin K intakes on food questionnaires then were followed for coronary heart disease (CHD) occurrence for over eight years. The mean K1 intake was 212 mcg/day, while the mean K2 intake was 29 mcg/day. Vitamin K2 intake, but not K1, was associated with decreased CHD risk.
Three earlier observational studies that examined vitamin K intake and risk of CHD found consistent lack of benefit from K1. The U.S. research team that conducted both the large Nurses' Health Study (72,874 female nurses) and the Health Professionals' Follow-Up Study (40,087 men) looked only at K1 intakes and concluded that high intake was a marker for dietary and lifestyle patterns associated with lower cardiovascular risk, rather than a viable measure of vitamin K specifically decreasing risk.141,142 The third study - the Dutch Rotterdam Study - also found significant associations between vitamin K2 intake (but not K1) and decreased CHD risk.143
In the Rotterdam Study, which followed 4,807 men and women over age 55 for 7-10 years, the highest tertile of K2 intake (MK-4 through MK-10, >32.7 mcg/day) showed significantly reduced risk for all-cause mortality, incident CHD, and CHD mortality.143 The same K2 intake level also afforded protection against aortic calcification (covered in more detail in the section that follows). Vitamin K1 intakes showed no statistically significant associations
Artery Elasticity
Vitamin K1 was used in a three-year RCT that examined carotid elasticity.144 Postmenopausal women (n=108), ages 50-60, were assigned to take a placebo, a supplement containing minerals and vitamin D (MD group), or the same supplement with K1 (MDK group). The MD supplement supplied daily 500 mg calcium, 150 mg magnesium, 10 mg zinc, and 8 mcg vitamin D3 (400 IU). The MDK supplement supplied an additional 1,000 mcg vitamin K1. At the trial's end, the elastic properties of the common carotid artery were not significantly worse in the MDK group, but had deteriorated in the MD and placebo groups; elasticity had deteriorated 13.2 percent in the placebo group (95% CI -35.8 to -5.3), compared to the MDK group. The researchers concluded that K1 in combination with vitamin D and the minerals had long-term beneficial effects on both the structure and function of the carotid arterial wall. Loss of vessel elasticity is often related to wall calcification.
Inhibition of Vascular Calcification
Vascular and heart valve calcification is commonly observed in aging individuals and patients with diabetes and end-stage renal disease, and is linked to thrombosis and other cardiovascular disease.139 A 2009 meta-analysis of prospective studies reporting calcification and cardiovascular disease analyzed 30 articles that covered 218,080 subjects with a mean follow-up of 10.1 years.145 Calcification (versus no calcification) had odds ratios with 95% CI as follows: » All-cause mortality: OR 4.62 (CI 2.24-9.53) » Cardiovascular mortality: OR 3.94 (CI 2.39-6.50) » Coronary events: OR 3.74 (CI 2.56-5.45) » Stroke: OR 2.21 (CI 1.81-2.69) » Any cardiovascular event: OR 3.41 (CI 2.71-4.30) » End-stage renal disease: OR 6.22 (CI 2.73-14.14)
These investigators concluded, "The presence of calcification in any arterial wall is associated with a 3- to 4-fold higher risk for mortality and cardiovascular events...subjects with vascular calcifications are high-risk patients."145
A 1995 observational study on vitamin K and vascular calcification involved a population-based sample of 113 postmenopausal women and assessed dietary intake of K1 but not of K2.146 Vitamin K1 intake was found significantly lower in a subgroup of women ages 60-69 with calcifications of the abdominal aorta, versus those without calcification. Also, in the women with calcification, circulating osteocalcin had lower calcium-binding affinity.
The Rotterdam observational study143 examined aortic calcification in 4,473 subjects. As with the other cardiovascular risk measures in this study, the highest tertile for K2 intake (>32.7 mcg/day) showed benefit, with a minimum 44-percent protection against calcification (OR 0.56; 95% CI 0.39-0.80; p=0.001). Vitamin K1 intake showed no benefit.
A 2005 study reported on a sample of 807 active duty U.S. Army personnel (ages 39-45, gender not specified) screened for coronary artery calcification using electron-beam computed tomography (EBCT).147 Vitamin K1 intakes, estimated using a dietary questionnaire, were not significantly correlated with decreased coronary calcification.
Another Dutch observational study also found no correlation between vitamin K1 intake and coronary calcification.148 It surveyed 564 postmenopausal women for coronary calcification and calculated their K1 and K2 (MK-4 to MK-10) intakes via questionnaire. Menaquinone intake was associated with reduced calcification (RR 0.80; 95% CI 0.65-0.98; p=0.03).
A double-blind, three-year RCT tested vitamin K1 for coronary calcification inhibition.149 Healthy men and women (n=388; average age 68) were randomized to receive either K1 (500 mcg/day) plus a daily effervescent multivitamin formula or the multivitamin alone. Both groups also received a second daily effervescent tablet that contained calcium (600 mg) and D3 (400 IU). As expected,
plasma K1 concentrations increased in the group that received K1, but not in the control group. K1 significantly slowed progression of preexisting calcification (6% less progression compared to the control group; p<0.04), but only in those subjects who were >85-percent compliant with the program.
Vascular calcium deposition occurs in vessel wall smooth muscle via mechanisms similar to those underlying bone formation.150 The most likely mechanism is depletion or malfunction of MGP, a VKD protein. Reminiscent of the human MGP mutation that results in Keutel syndrome,116,117 targeted deletion of the MGP gene ("knockout") in mice causes extensive calcification of the abdominal aorta.151,152
MGP has been found in human atherosclerotic plaques,153 with the undercarboxylated form more concentrated in the calcified regions of the vasculature.154,155 Vitamin D status may also influence MGP function: the promoter region for the MGP gene contains a 1,25D responsive element, and MGP transcription can be up-regulated by vitamin D3.156
Vitamin K clearly has pleiotropic functions in the cardiovascular milieu that surpass its classic coagulation functions. Vitamin K sufficiency activates a variety of carboxylated proteins that manage calcium homeostasis in the circulating blood, the walls of the blood vessels, and undoubtedly also the heart.157 These normally prevent inappropriate mineralization of the vessel walls, and their absence or malfunction can lead to calcification. MK-4, but not phylloquinone, protects against arterial calcification in warfarin-treated rats.158
Vitamin K Supplementation to Stabilize Warfarin Anticoagulation
Warfarin and related coumarins (phenprocou-mon, fluindione, acenocoumarol) have been the preferred oral anticoagulants for more than 50 years. They are used on an estimated minimum 1-1.7 percent of individuals.159 Although all of them present severe difficulties in clinical practice, warfarin is by far the most commonly prescribed, so will be used herein to denote the entire drug class.
These vitamin K antagonistic anticoagulants are most commonly used to prevent venous thrombo-embolisms and systemic embolism, for primary prevention of acute myocardial infarction in high-risk men, and for the prevention of stroke, recurrent infarction, or death in patients with acute myocardial infarction. All work via potent vitamin K antagonism.160
Warfarin and the other vitamin K antagonists are effective anticoagulants, indirectly blocking the classic coagulation cascades by directly binding to the VKOR enzyme that ensures the reductive recycling of vitamin K.160 Since the body's vitamin K stores are typically very limited, the anticoagulants' effects can be virtually immediate. Their clinical difficulties come mainly from: (1) a narrow therapeutic window, (2) considerable variability in dose response among subjects, (3) interactions with other drugs and diet, and (4) problems with dosing from miscommunication between physician and patient.
The risk of major hemorrhage from warfarin is as high as 7.4 percent in population cohort studies; with intracranial bleeding, the risk of death approaches 60 percent.159 Because warfarin-induced bleeding is difficult to control, there is a need to better manage anticoagulant therapy. Vitamin K repletion is already an established option for managing warfarin patients. In the case of hemorrhage or the threat thereof, the aim of treatment is to elevate the reduced levels of VKD clotting factors, the degree of urgency depending on the international normalized ratio (INR) and the severity of bleeding.159
The INR is a value that reflects the degree to which warfarin has reduced coagulation factor levels and the associated coagulation potential of the blood.161 Usually an INR of 2.0-3.0 is the desirable therapeutic range; values less than 2.0 are associated with increased risk for embolism, while values greater than 4.0 are associated with increased bleeding complications. The bleeding risk, particularly for intracranial hemorrhage, increases markedly as the INR exceeds 4.5.161 Even in clinics that specialize in warfarin management, INRs are outside the therapeutic range one-third to one-half the time.162
Clinical Experience with Vitamin K to Balance Warfarin
Case series studies and other non-randomized trials previously indicated that relatively small increases of oral vitamin K intakes might improve anticoagulation control for patients on warfa-rin.161,163,164 Noting that patients with unstable control of anticoagulation have a consistently and significantly lower intake of vitamin K than their matched stable counterparts, a UK anticoagulation group165 recruited atrial fibrillation patients with ongoing unstable response to warfarin into a double-blind, placebo-controlled study.
These patients' target INR was 2.0-3.0 and they were classified as unstable if their standard deviation was greater than 0.5 and/or they had a history of at least three warfarin dose changes in the previous six months.165 Sixty-eight patients were randomized to 150 mcg/day vitamin K1 or a placebo for six months. Their anticoagulation status was monitored initially once weekly, then
once monthly after they entered the target INR range.
Although both the placebo group and the vitamin-K group demonstrated some improvement in INR (predictable from patients enrolled into a clinical trial), the vitamin K group showed significantly more marked improvement - more than a two-fold decrease in the standard deviation of the INR and a nearly two-fold increase in percentage time within target INR range. Of the vitamin K patients, 33/35 showed improved anticoagulation control and 19/35 became stable. Of those on placebo, 24/33 showed some degree of improvement and 7/33 became stable.165
A recent U.S. RCT recruited 676 patients with very high baseline INR values (4.5-10.0). Patients received either 1.25 mg/day of vitamin K (type unspecified) or a placebo, for three months.161 Although one day after the trial began INR was significantly more improved in the vitamin K group, after 90 days no significant improvements in INR, bleeding events, thromboembolism, or death were detected in the vitamin K group, compared to placebo. Retrospective analysis also failed to find differences after seven and 30 days.
This trial has been extensively criticized for using a noncommercial source of vitamin K, not standardizing the warfarin regimen during the course of the trial, using too low a dose of vitamin K considering the very high INR patient values, and for omitting details of other potentially important clinical variables, such as concomitant antiplatelet agents or recent surgery.166-169 Two groups critical of the trial167,168 vowed to continue the 2008 evidence-based practice guidelines from the American College of Chest Physicians, which include the option of using oral low-dose vitamin K.170
Countering the Long-Term Calcification Threat
A long-term adverse effect of warfarin therapy is vascular calcification.152,171 The proven mechanism is warfarin's near-shutdown of the body's vitamin K recycling capacity.160
As the availability of functional (that is, electronically reduced) vitamin K via the K cycle becomes limited, whether from warfarin therapy, from dietary inadequacies, or from other factors, the body progressively is deprived of vitamin K's carboxylation capacity. The VKD proteins OC and MGP are abundant in bone110,111 and vessel wall connective tissues, respectively,110,115-117 and are central to calcium homeostasis in these tissues. Vitamin K depletion impairs their physiological carboxylation, which translates into derangement of calcium homeostasis (among other adverse effects);110,117 hence, the pathological calcification of the blood vessels, a severe complication of warfarin therapy.161
The importance of VKD carboxylation for calcium homeostasis is also established through animal experiments. Thus in rats, the use of warfarin to experimentally block vitamin K-dependent carboxylation (the basis for its anticoagulant action in humans) leads to arterial calcification, which is reversed by diets high in vitamin K.152 Gene expression experiments with mice suggest that vitamin K as MK-4 acts as an anti-calcification component in the vessel wall.139 To best ensure against pathologic calcium distribution patterns throughout the body, it would seem prudent to maintain vitamin K status sufficient to fully (or near-fully) carboxylate OC, MGP, and other VKD proteins.
On balance, the evidence for vitamin K as a complement to warfarin anticoagulation favors relatively modest vitamin K doses, ranging from 100 mcg/day to as high as 2 mg/day. For most patients, using a reputable dietary K supplement is better advised than attempting to standardize vitamin K intake using foods, which vary greatly in their vitamin K content. When combined with competent medical management of the INR, prudent personal management of vitamin K status should ensure the greatest benefits from vitamin K's diverse and potent pleiotropic actions.
Evidence for Synergy Between Vitamins D and K
The potential of vitamin K to lower the risk of fracture and otherwise improve bone quality has been most systematically pursued in Japan. At Osaka Medical College, Ushiroyama et al found that vitamin K plus vitamin D increased bone density in human subjects markedly better than vitamin K alone.172 Postmenopausal women (n=126) with osteopenia and osteoporosis were randomized to four groups for two years: (1) diet alone, (2) 45 mg/ day MK-4, (3) a D3 analog (1alpha-hydroxycholecal-ciferol, Onealfa® at 1 mcg/day), or (4) the combination K2 plus D3. Calcium was not supplemented or otherwise controlled. BMD was measured in the lumbar spine.
After two years, BMD decreased four percent in the control group, while it increased in the combination K2+D3 group (4.92% ±7.89%; p<0.01 versus control), just 0.135 percent in the K2 group (0.135% ±5.44%; p<0.05 versus control), and BMD in the D3 group was significantly different from control but not from K2.172 This study suggests that combining K2 and D3 might have a synergistic effect superior to using either alone. A caveat is that the D3 molecule employed was not cholecalcif-erol but an analog.
To explain this apparent synergy of vitamins K and D, one likely nexus is the VKD protein osteo-calcin. Vitamin K is necessary to gamma-carboxyl-ate OC and thereby activate the molecule, which is essential for bone hydroxyapatite crystal forma-tion.173,174 When circulating concentrations of vitamin K are insufficient, a greater proportion of OC remains undercarboxylated. Elevation of total undercarboxylated OC has been linked to lower bone density in elderly men and women.174 Preceding the carboxylation step, the transcription of the OC gene to messenger RNA and its subsequent translation into OC polypeptide are regulated by 1,25D and therefore vulnerable to vitamin D deficiency.175
Another area of vitamin D and vitamin K overlap is inflammation, which is causally implicated both in cardiovascular disease and osteoporosis.176,177 More specifically, proinflammatory imbalances of cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-a) are implicated in both osteoporotic bone deterioration and calcification of blood vessel walls, which can coexist in the same patient."178,179
Both vitamins D and K have been found to down-regulate pro-inflammatory cytokines and biomarkers in clinical settings. Vitamin D supplementation lowered circulating TNF-a levels in patients with osteoporosis180,181 and heart failure.74 In the Framingham Offspring Study cohort, a community-based sample of healthy men and women, vitamin K status was inversely associated with circulating markers of inflammation (p<0.001).105 Higher vitamin K intake was significantly correlated with lower blood levels of C-reactive protein (CRP; p<0.03), IL-6 (p<0.009), and urinary isoprostanes (p<0.02). This study suggested that vitamin K's inverse association with inflammatory markers was separate from its gamma-carboxylation function, since ucOC showed no association with these markers.
Vitamins K and D also overlap metabolically at the cellular level. The cyclic oxidation and reduction of vitamin K is a source of electron transfer for antioxidant power to protect living cells against oxidative attack.182 Likewise, D3/cholecalciferol has potent antioxidant capacity, as evidenced in rats.183 Using cultured human osteoblasts, Japanese researchers discovered that vitamin K2 promotes normal vitamin D-stimulated osteocalcin accumulation and mineralization processes in these cells.184 Human osteoblasts also carry the vitamin K cycle enzymes, and 1,25D enhances the reductive recycling of MK-4.185 Hence vitamins K and D can mutually enhance each other's metabolism, a biochemical reciprocity consistent with clinical synergy.
Conclusions
Experts seem to agree that, regardless of the exact blood ranges used to define deficiency and insufficiency, functional vitamin D deficiency is widespread.9,17,186 From 42 epidemiological and prospective studies recently analyzed by Barnard and Colon-Emeric,60 the prevalence of vitamin D insufficiency (which they defined as 25D concentration <30 ng/mL) in community-dwelling older adults (>65 years of age) ranged from 40-100 percent in the United States and Europe. In two U.S. states (Colorado and Georgia), despite reported consumption of more than the required daily intake of vitamin D (400-600 IU/day), vitamin D insufficiency (defined as 25D <32 ng/ mL) among community-dwelling older adults ranged from 37-74 percent. High rates of vitamin D deficiency have also been reported in children and adults living in the Middle East, India, Australia, New Zealand, and Asia.186
Using strict criteria to rank the strength of the clinical evidence, Peterlik et al assessed the links between vitamin D status and disease risks9,20 and found convincing evidence that vitamin D insufficiency contributes to osteoporosis and related bone diseases, and to colorectal and breast cancer. They rated the evidence good for other cancers (prostate, endometrial, ovarian, esophageal, gastric, pancreatic, bladder, renal), cardiovascular disease, neuromuscular dysfunctions, type 1 diabetes, tuberculosis, gingivitis, and periodontal disease. Depression and cognitive difficulties are not yet firmly linked to vitamin D insufficiency, but could emerge in the near future.60 Cannell and Hollis discuss vitamin D links with multiple sclerosis and many other diseases and suggest that such routine complaints as fatigue, muscular weakness, and musculoskeletal pain also could be linked to vitamin D deficiency.28
In the case of vitamin K, the currently recommended U.S. adult AI is 90-120 mcg/day.109 The recommended intakes are based solely on the amounts required to maintain coagulation function, and some experts believe these may not be high enough to ensure optimal gamma-carboxyl-ation of VKD proteins. As one measure, when prothrombin is fully carboxylated in the blood, about 10-40 percent of serum OC remains undercarboxylated.187
Vitamin K is just now getting the scientific respect it deserves. In a sweeping 2009 review, McCann and Ames reported on "gene knockout" experiments with vitamin K-dependent proteins in animals.113 These experiments establish that fully half of the 14 VKD proteins identified to date are absolutely essential to life. McCann and Ames also documented a variety of pathologies linked to vitamin K deficiency - from bone and cardiovascular conditions to insulin resistance, osteoarthritis, chronic kidney disease, and cancer. Also, vitamin K can operate other than via VKD protein carboxyl-ation, for example to directly influence gene expression by binding with the steroid and xenobiotic receptor.29
The wide-ranging, pleiotropic involvements of vitamins D and K in calcium homeostasis and in bone and cardiovascular health, with their attendant contributions to lowering morbidity and premature mortality, have significant public health implications. Both these nutrients are safe to use, readily available, and relatively inexpensive. Their considerable metabolic overlap and likely synergy of benefits renders these two nutrients powerful tools to upgrade the public health.
References
See pdf