Child bone conference: many vitamin D and ricket abstracts
6th International Conference on Children's bone Health
June 22-25, 2013, Rotterdam Netherlands
See also VitaminDWiki
The following are a few of the many presentations and posters on vitamin D and/or rickets
Several are incomplete due to problems of the text being in footnotes. See PDF for actual details
PDF is attached at the bottom of this page
IS11 Other Therapeutic Options: Nutrition, Vitamin D, and Physical Activity
Catherine Gordon
Hasbro Children's Hospital and Brown University, Providence, RI, USA
The childhood and adolescent years represent a critical period for bone acquisition. Extrinsic factors such as diet and physical activity represent modifiable variables that may have a significant impact on a young adult's peak bone mass. This lecture will consider dietary supplementation with specific nutrients as a strategy to augment bone density during the childhood and teenage years. An overview will be provided, as well as data reviewed from supplementation trials in the pediatric age group. Calcium and vitamin D will be discussed as traditional approaches to increase bone mass, as well as data from trials of vitamin K and magnesium, with discussion on these and other less common nutrients. Lastly, physical activity will be discussed as part of the skeletal therapeutic armamentarium for children and adolescents. Different types of activities will be reviewed (weight bearing vs. not). as well as the use of vibrating plates for pediatric chronic disease groups. These platforms represent a unique means by which high frequency, low magnitude mechanical stimulation can be provided to change bone turnover to increase bone mass in children.
OC4 Maternal antenatal 25(OH)-vitamin D status is associated with offspring muscle strength at 4 years of age
Rebecca Moon1-2, Avan A Sayer1, Georgia Ntani1, Justin Davies2, Sian Robinson1,3, Keith Godfrey1,3, Hazel Inskip1, Cyrus Cooper1, Nicholas Harvey1
1MRC Lifecourse Epidemiology Unit, University of Southampton, UK, 2Paediatric Endocrinology, University Hospital Southampton NHS Foundation Trust, UK, 33NIHR Southampton Biomedical Research Centre, University of Southampton and University Hospital Southampton NHS Foundation Trust, UK
Objectives: Serum 25(OH)-vitamin D [25(OH)D] concentration is known to influence muscle function in postnatal life. Maternal 25(OH)D status during pregnancy has been implicated in the fetal programming of bone and fat mass, but little is known about its role in determining offspring muscle development. We investigated the associations between maternal serum 25(OH)D concentration in pregnancy and offspring muscle mass and strength at 4 years.
Materials and Methods: A prospective mother-offspring birth cohort, the Southampton Women's Survey (Southampton, UK), was studied. Maternal serum 25(OH)D status was measured at 34 weeks gestation. At 4 years, offspring hand-grip strength (Jamar Dynamometer) and body composition by dual energy Xray Absorptiometry (Hologic Discovery) were assessed. Offspring physical activity (PA) was assessed over seven days using accelerometry (Cambridge Neurotechnology Actiheart).
Results: 326 mother-offspring pairs were included. Maternal serum 25(OH)D concentration in late pregnancy was positively associated with offspring height-adjusted hand grip strength (P=0.12 SD/SD, p=0.02), which persisted after adjustment for a number of maternal confounding factors (including maternal height, pre-pregnancy body mass index, gestational weight gain, walking speed in late pregnancy and smoking status), duration of breastfeeding and child's physical activity at 4 years 0=0.12 SD/SD, p=0.03). Maternal 25(OH)D was also positively associated with offspring percent lean mass (P=0.11 SD/SD, p=0.05), but not total lean mass (P=0.02 SD/SD, p=0.67). This however did not persist after adjustment for confounding factors (P=0.07 SD/SD, p=0.24).
Conclusions: Maternal 25(OH)D status during pregnancy is positively associated with offspring grip strength at four years. These results are consistent with a role for antenatal 25(OH)-vitamin D exposure in offspring muscle development.
P111 Vitamin D status and association to bone health in 781 healthy 8-11 year old Danish school children -preliminary results from the OPUS School Meal Study
RA Petersen1, CT Damsgaard1, S Dalskov1, LB Sorensen1, RP Laursen1, MF Hjorth1, R Andersen2, I Tetens2, H Krarup3, A Astrup1, KF Michaelsen1, C Molgaard1
Department of Nutrition, Exercise and Sports, Faculty of Science, University of Copenhagen, Frederiksberg C, Denmark, 2Division of Nutrition, The National Food Institute, Technical University of Denmark, S0borg, Denmark, 3Department of Clinical Biochemistry, Section of Molecular Diagnostics, Aalborg University Hospital, Denmark
Background: Low vitamin D concentrations among children and adolescents at northern latitudes are frequently observed. Also, inverse associations between 25-hydroxyvitamin D (25(OH)D) and PTH concentrations have been found in children of different ages. More studies on the link between vitamin D status and childhood bone health are needed.
Objective: To evaluate the status of serum 25(OH)D in autumn and the association between 25(OH)D concentrations and bone health in 781 healthy 8-11 year old Danish children (55°N).
Method: A Cross-sectional analysis was performed using baseline data from the OPUS (Optimal well-being, development and health for Danish children through a healthy New Nordic Diet) School Meal Study, including 3rd and 4th graders from nine public schools. In autumn 2011, fasting blood samples were drawn and serum 25(OH)D and intact PTH analysed. Background interviews were conducted and anthropometry, puberty stage, intake of dietary supplements and physical activity was measured. Whole body DXA scans were performed and Total body less head (TBLH) DXA values were used in data analyses.
Results: Serum 25(OH)D ranged from 15.2 to 132 nmol/l, with mean of 60.7 nmol/l±18.7. Twenty-six per cent of the children had concentrations between 25-50 nmol/l, while 2.4% had concentrations <25 nmol/l. Intake of dietary supplements >4 days/week (n=305) was associated with higher serum 25(OH)D (p<0.001). Girls had significantly lower 25(OH)D (p<0.001), and significantly higher iPTH (p=0.012) concentrations than boys. Serum 25(OH)D was inversely associated with iPTH without, and with, adjustment for age, gender, pubertal stage, month and ethnicity (p<0.001). No significant associations were found between serum 25(OH)D and Bone Mineral Content (BMC) without, nor with, adjustment for Bone Area (BA), age, height, weight, gender, pubertal stage, ethnicity and physical activity. Likewise, no associations were found between serum 25(OH)D and BA or BMD.
Conclusion: A substantial number of Danish children did not reach the recommended level of 25(OH)D (>50 nmol/l) during autumn. Despite a significant association with iPTH, no overt association between serum 25(OH)D and bone health was established.
The OPUS project (Optimal well-being, development and health for Danish children through a healthy New Nordic Diet) is supported by a grant from the Nordea Foundation.
P116 Vitamin D dependent rickets type 1 (VDDR-1): two years after discontinuation of treatment
Victoria Kougia1, Stella Seitanidou1, Asterios Kampouras1, Filotas Talidis1, Konstantinos Kollios1, Emmanuel Roilides1
Third Department of Pediatrics, Hippokration Hospital, Thessaloniki, Greece
Backround: Vitamin D dependent rickets type 1 (VDDR-1) is an autosomal recessive disorder caused by 1a hydroxylase enzyme deficiency, that leads to low or undetectable levels of 1,25 dihydroxyvitamin D despite normal levels of 25-hydroxyvitamin D levels. Additional laboratory findings include hypocalcemia and increased levels of parathyroid hormone. Clinically it presents as early onset rickets and severe hypotonia.
Presenting Problem: A 6 year old Caucasian girl was referred to our Clinic after a 6 month history of hypotonia. Rickets was diagnosed at the age of 9 months, based on typical laboratory and radiological findings. Severe hypophosphatemia and generalized aminoaciduria were identified then. The levels of 25-hydroxyvitamin D were normal. She was started on 1-a hydroxyvitamin D with prompt clinical and laboratory improvement. Under medication, the biochemical findings normalized and the child remained asymptomatic. That misled the parents into discontinuing treatment 3,5 years after diagnosis and for the next two years.
Clinical Management: Physical examination on admission revealed genu valgum, short stature and generalized hypotonia. Laboratory workup revealed hypocalcemia, hypophosphatemia, marked elevation of alkaline phosphatase and parathormone, with normal levels of 25-hydroxyvitamin D and low levels of 1,25 dihydroxyvitamin D. Based on these findings and the fact that she had previously responded well to 1-a hydroxyvitamin D, VDDR-1 was diagnosed. Awaiting genetic confirmation she was restarted on 1-a hydroxyvitamin D. Biochemical and radiographic improvement was achieved within 3 and 6 months respectively.
Discussion: Clinical and radiological findings of VDDR-1 are indistinguishable from those of other forms of rickets. Distinction between the two can be based on characteristic biochemical findings. Normal levels of 25-hydroxyvitamin D exclude nutritional rickets, while normal serum calcium combined with elevated PTH excludes hypophosphatemic rickets.
Patients with DDR-1 should receive life long replacement treatment with 1-a hydroxyvitamin D or calcitriol.
P118 Variation in response to vitamin D therapy in a series of consecutive children referred to a paediatric bone disease service
Fawaz Arshad12-, Sally Hinton2, Nick Bishop1,2, Paul Arundel2
Department of Human Metabolism, University of Sheffield, UK, 2Sheffield Children's Hospital, UK
Objectives: Guidelines for treatment of vitamin D deficiency (VDD) vary. We aimed to review the range of treatment regimens for VDD used locally and variation in responses.
Methods: We conducted a retrospective review of the records of consecutive patients referred to a children's bone disease service with a putative diagnosis of VDD over a 14 month period. Data collected includes vitamin D type used, dose and duration of treatment, and pre ? ? ?
Abstracts
AM
and post serum 25-hydroxy vitamin D (25OHD). Cases were excluded if these data were missing. Weight was used to calculate total dose of vitamin D per kg administered. In the absence of a contemporary weight, subjects were assumed to have mean weight for age. Presence of rickets, radiographic reports, history of fracture and adverse events were collected.
Results: From 66 consecutive subjects, 29 had pre- and post-treatment 25OHD concentrations and a confirmed serum 25OHD <25nmol/l. Demographics - 18/29 male; 12/29 South Asian, 7/29 Black African, 4/29 White British. 13/29 had radiographs looking for signs of rickets. In 2/13 rachitic features were identified. In both cases repeat radiographs confirmed resolution with treatment. 4/29 had ever suffered fractures. Cholecalciferol treatment was variably instituted by primary or secondary care physicians. Daily doses ranged 3000-10000 U (median 6000); duration 4-12 weeks (median 6). 2/29 subjects received two doses
of 100000 U each. Estimated total dose/kg ranged 3400-35000 U/kg
(mean 13500, SD 7400). The increase in serum 25OHD correlated with estimated total dose/kg (R2=29%, p=0.003). 2/29 remained vitamin D insufficient (34 and 45nmol/l). 4/29 subjects had an increase in 25OHD >200nmol/l. These were all under 18 months of age and received estimated total doses 11000-35000 U/kg over 4-12 weeks. There were no recorded adverse effects.
Conclusion: We found that commonly used regimens for treatment of VDD were effective in raising 25OHD to >50nmol/l with no evidence of harm. This study is limited by its retrospective character, small size, incomplete data and potential bias regarding subject selection. However, there is variability in response to vitamin D treatment and we believe that clinicians should consider the weight-related total dose, particularly in younger children.
P164 Vitamin D deficiency in Moscow children and adolescents
Dmitry Shilin1, Tatyana Osipova2, Lidia Kostina2
Moscow State University of Medicine and Dentistry, Russia, 2Scientific Center EFIS, Moscow, Russia
Objectives: to determine the prevalence and intensity of D-deficiency in children and adolescents in the metropolitan area with subtotal deficiency of ultraviolet B (55° N).
Methods: from May 2008 to May 2010 in a random sample of 163 Muscovites 0-18 years of old (9.9±0.4; girls/boys = 81/82) serum 25-hydroxyvitamin D content was determined by chemiluminescent analysis [DiaSorin Inc., USA; n=56 and Roche Diagnostics, Switzerland; n=107). The results were evaluated according to the criteria McKenna M.J. and Freaney R. (1998).
Results: the 2-year overall frequency of subnormal vitamin values (<40 ng/ml) was 77%. Mild decrease (20-<40) is set at 32% of young Muscovites, moderate (10-<20) - 30%, severe (<10) - 15%. A mild deficiency prevailed from May to August (43±7% of n=54 vs. 27±4% of n=109 in the remaining months, RR=1.6 with 95% CI [1.03-2.5]; p<0.04), and more severe (<20 ng/ml) - from September to April (53±5%, n=109 vs. 28±6%, n=54 for others, RR=1.9 [1.2-3.1]; p=0.002). Gender differences were not found. Between chronological age and separate degrees of D-deficiency was found the weak correlation (r=+0.23-0.32; p=0.0008-0.004). The sole category of children with the best vitamin status were at the age of 0-3 years: they had normal levels three times more common (">40 ng/ml": 57±11%, n=23 vs. 18±3%, n=140 in patients 4-18 years, RR=3.2 [1.9-5.2], p=0.0001) and three times more rare were cases with moderate to severe D-deficiency ("<20" 17±8% vs. 49±4%, RR=0.35 [0.14-0.87], p<0.009).
Conclusion: in Russian largest metropolis with geographical and social disadvantage (due to low insolation and absence of mass prophylaxis) most children older than 3 years and adolescents have vitamin D insufficiency; this unfavorable feature revealed regardless of sex, often manifests with moderate to severe degree, for the most part of calendar year.
[Summary vy VitaminDWiki: Moscow children at 56 degrees latitude away from equator: 77% < 40 ng; and age 0-3 57% > 40ng]
P184 High FGF23 measurements in a child with Vitamin D dependent rickets type I. Cause or consequence?
Ciara McDonnell1, Bryony Treston1, Nuala Murphy1, Mark Kilbane2, Malachi McKenna2
'Children's University Hospital, Dublin, Ireland, 2St Vincent's Hospital, Dublin, Ireland
Background: Defects in 1-a-hydroxylase enzyme activity result in reduced activity of 1, 25(OH)2D causing Vitamin D dependent rickets. Physiologically FGF23 levels are stimulated by a rise in 1, 25(OH)2D which in turn suppresses 1-a-hydroxylase expression to complete the feedback loop.
Presenting Problem: A 15 month old Irish Caucasian girl was referred by her GP for failure to weight bear. She was born at term via elective section, and was bottle fed with no dietary or absorption issues. She had prominent swelling of her wrists, femora and tibiae but no genu valgum or varum, talipes or spinal anomalies. X-rays demonstrated metaphyseal flaring of all long bones suggestive of rickets. Skeletal biochemistry confirmed this with raised alkaline phosphatase, low-normal calcium and low phosphorus. Serum 25OHD was raised while 1, 25(OH)2D was inappropriately low. Subsequent genetic testing identified a heterozygous mutation in the 1-a-hydroxylase gene considered to be pathogenic because it creates a frameshift mutation changing the amino acid sequence from position 387 with a premature truncation. The mutation is paternally inherited.
Clinical Management: The girl was commenced on calcium supplementation with One Alpha replacement resulting in improvements in serum PTH, alkaline phosphatase, calcium and phosphorus over subsequent months. FGF23 levels were measured at initial assessment and during recovery and are persistently raised [Range 127-190 RU/ml, reference range <100] despite persistent low phosphorus levels thought to be secondary to the raised PTH level. Clinically, her demeanour has improved from initial treatment and after six months she began weight bearing without difficulty and showing interest in walking.
Discussion: The phenotype of this girl reflects the diagnosis of a 1-a-hydroxylase mutation albeit with the identification of only one affected allele. Blunted activity of 1,25[OH]2D and hypophosphataemia should both result in the lowering of FGF23 levels yet counter intuitively the levels remain high. Is this a cause or consequence of therapy?
P192 The assessement of the vitamin D supply in the population of Polish children at the age of 9-12 years -multicentre research- preliminary report
Danuta Chlebna-Sokol, Joanna Golec, Jolanta Karalus, Zenon Halaba, Elzbieta Karczmarewicz, Jerzy Konstantynowicz, Beata Kulik-Rechberger, Marek Niedziela, Anna Dobrzanska 'Medical University of Lodz Department of Propedeutics of Paediatrics and Bone Metabolic Diseases, Lodz, Poland, Medical University of Wroclaw Department of Ginecology and Neonatology, Wroclaw, Poland, The Children's Memorial Hospital Department of Biochemistry and Experimental Medicine, Warsow, Poland, Medical University of Bialystok Department of Paediatrics and Developmental Disturbances in Children, Bialystok, Poland, Medical University of Lublin Department of Propedeutics of Paediatrics, Lublin, Poland, Medical University of Poznan Department of Endocrinology and Reumatology of Children, Poznan, Poland, Medical University of Warsow Department of Neonatology Pathology and Intensive Care for Newborns, Warsow, Poland
Introduction: The importance of vitamin D in metabolism, bone growth and functioning of many organs and systems (the plejotropic effect) has been broadly discussed in the literature recently. The systemic deficiency of vitamin D connected with the lower sunlight exposure and the decreased diet supply favours to bone mineral density lowering and the bone structure disorganization. More and more often the common vitamin deficiency in children and adolescents has been observed. It is universally known that even temporary shortage of vitamin D during the rapid growth may hamper the correct peak bone mass acquistion.
Aim: The aim of the study was to determine the vitamin D supply in schoolchildren from the different regions of Poland.
Patients and methods: The study comprised research centers from the cities in Poland: Lodz (coordinator), Bialystok, Katowice, Szczecin, Lublin, Poznan. The healthy schoolchildren at the age of 9-11,99 were
and functioning of many organs and systems (the plejotropic effect) has been broadly discussed in the literature recently. The systemic deficiency of vitamin D connected with the lower sunlight exposure and the decreased diet supply favours to bone mineral density lowering and the bone structure disorganization. More and more often the common vitamin deficiency in children and adolescents has been observed. It is universally known that even temporary shortage of vitamin D during the rapid growth may hamper the correct peak bone mass acquistion.
Lublin, Poznan. The healthy schoolchildren at the age of 9-11,99 were examined. In every child the liver metabolite of vitamin D was detected twice (first after the winter season, secondly after the summer). The serum was analysed in the laboratory with the international certificate in the Department of Biochemistry and Experimental Medicine in The Children's Memorial Health Institute in Warsow. The serum concentration of vitamin D (25OHD) was detected with the immunochemiluminescence method with the DEQAS international control system. The sufficient 25 OHD serum concentration was recognized at range of 20-100 ng/ml. The concentration at the range of 10-20 ng/ml was recognized as vitamin D insufficiency and below 10 ng/ml as vitamin D deficiency.
Results: The 715 of children were examined. The greatest vitamin D shortages were observed in Szczecin and Bialystok - in 95% and in 90% of children ( insufficiency in 64% and 67% and deficiency in 31% and 23%). In Katowice and Lublin the lower vitamin D concentration was detected in 89% and 88% of children (insufficiency in 73% and 68% and deficiency in 16% and 20%). The lower shortages were revealed in children from Lodz and Poznan- in 77% and 74% (insufficiency in 57% and 59% and deficiency in 20% and 15%). The results of the vitamin D in the same children proved considerable improvement after the summer. The greatest shortages were obtained in Poznan and Szczecin - in 52,9% and 42,1% (insufficiency in 52,2% and 42,1% and deficiency in 0,7% and 0%). On the other hand in Lodz the decreased 25OHD concentration was observed in 41,5% of children and it was the insufficiency only. The lowest shortages were revealed in Lublin, Bialystok and Katowice- in 28%, 26,3% and 26,3% of children and again it was the insufficiency only.
Conclusions: The lower concentration of liver metabolite of vitamin D in as many of examined children indicates on adverse diet and climatic conditions which may influence on bone mineralization in children.
P199 Levels of 25(OH)vitamin D in Children and Adolescents with Type 1 Diabetes Mellitus and in Healthy Controls in Bulgarian Population
Olga Slavcheva1, Maia Konstantinova1, Adelina Tsekova2, Radka Savova1, Margarita Arshinkova1
'University Pediatric Hospital, Sofia, Bulgaria, 2Alexandrovska University Hospital, Sofia, Bulgaria
Objectives: The aim is to examine the serum levels of 25(OH)vitamin D in children and adolescents with type 1 diabetes mellitus and in healthy controls and to determine whether patients with diabetes have higher prevalence of vitamin D deficiency/insufficiency and whether it is correlated to its metabolic control.
Methods: A cross-sectional study of 73 patients (35 males) aged 11,84±4,44 years and 27 healthy controls (15 males), aged 7,36 ± 4,71 years. The participants are divided in 2 subgroups according to the month the sample was taken- May-September and October-April. Patients are divided in 2 subgroups according to their metabolic control: good (HbA1c < 7,5%) and poor (HbA1c > 7,5%). Levels of 25(OH)vitamin D were determined by electrochemiluminescence detection technology. The statistical methods used are Mann-Whitney and Kruskal-Wallis tests.
Results: There is no statistically significant difference between 25(OH)vitamin D levels in diabetic patients and in controls (p=0,783). The mean level of 25(OH)vitamin D in patients is slightly higher- 25,39 ±8,14 ng/ml than in controls- 24,44±11,88 ng/ml. The mean levels of 25(OH)vitamin D are higher in the period with more outdoor sunlight. In May-September period - 29,01± 9,2 ng/ml in patients (n=28) and 29,85± 8,42 ng/ml (n=9) in controls, for October-April period 25(OH)vitaminD levels are 23,14±6,55 ng/ml vs 21,74±12,63 ng/ml for patients (n=45) and controls (n=18) respectively. We use US Endocrine Society guideline to define vitamin D deficiency and insufficiency as 25(OH)vitamin D level < 20ng/ml and 21 - 29 ng/ml respectively. 36% of all patients (n=26) and 33% of controls (n=9) have vitamin D deficiency. Vitamin D insufficiency is observed in 37% of patients (n=27) and 37% of controls (n=10).
Mean level of HbA1c in good control group (n=16) is 7,05±0,33%, in poor control group(n=39)- 9,18±1,36%. No correlation between metabolic control and vitamin D levels is found. Level of 25(OH)vitamin D are 25,86±7,29ng/ml and 25,56±8,23ng/ml respectively (p=0,476).
Conclusions: Presence of diabetes mellitus type 1 does not influence vitamin D metabolism. Our results show no significant differences between 25(OH)vitamin D levels in diabetic patients and in healthy controls. Vitamin D deficiency is slightly but not significantly prevalent in diabetic patients and is almost equal to that observed in healthy Bulgarian adults.
Supported by Grant from Medical University Sofia, Bulgaria.
P200 Low 25-hydroxyvitamin D levels in Scheuermann's disease: a preliminary study of nineteen patients
Edward Southern1-2, Max Gosey3,2
'LSU Health Sciences Center, New Orleans, LA, USA, 2Children's Hospital, New Orleans, LA, USA, 3Ochsner Clinic, New Orleans, LA, USA
Objectives: Scheuermann's disease is a common cause of pediatric kyphotic deformity, and its etiology remains poorly understood. A hypothetical relationship has been described between osteoporosis and the development of the disorder. Also, a recent study revealed that young pigs developed kyphosis when fed low-vitamin D diets. Due to these factors, we designed the present investigation to measure the prevalence of vitamin D insufficiency and deficiency in a group of patients with Scheuermann's disease.
Methods: This is a case series of nineteen patients. In this study, ICD-9 codes for kyphosis, juvenile osteochondrosis of the spine, and low back pain were used to identify patients with the diagnosis of Scheuermann's kyphosis and disc disease from the clinics of the senior author at a tertiary-care children's hospital over a six-month period. Patients with radiographic evidence of Scheuermann's disease (N=20) were evaluated by the authoring surgeon personally, and the diagnosis was confirmed. The study population included eleven males and nine females. High-performance liquid chromatography/mass spectrometry assay was used to measure serum 25-hydroxyvitamin D in all these patients (age ranges 10.6 to 18.3 at testing) during the course of their regular clinic follow-up, and one value is still pending. Vitamin D adequacy was defined by a value within our laboratory's normal range (32-100 ng/mL). Inadequacy was subdivided into insufficiency (20-32 ng/mL) and deficiency (<20 ng/mL).
Results: Of the nineteen currently returned vitamin D levels (for eleven males and eight females), fifteen patients (79%) had inadequate vitamin D levels (range 14-31 ng/mL), including eleven (58%) who were insufficient and four (21%) who were deficient. Only four values (21%) were within normal limits (range 32-43 ng/mL). Mean and median values were 25.7 +/- 7.4 and 24 ng/mL, respectively.
Conclusions: A majority of these Scheuermann's disease patients assayed for vitamin D were found to be insufficient, with a substantial number qualifying as deficient. These observations, coupled with the newly discovered link in vitamin-deficient piglets, demonstrate a need for a more detailed, prospective evaluation of our Scheuermann's disease patients, with an appropriate control group, and this will be the subject of a future longitudinal study, preferably at multiple centers.
P189 Clinical features of temporary brittle bone disease
Colin R Paterson
University of Dundee (formerly), Dundee, Tayside, UK
Temporary brittle bone disease has been a controversial explanation of multiple unexplained fractures in early childhood. Evidence for its existence is growing. We report the clinical and laboratory features of 104 patients investigated personally. These patients had in aggregate 984 fractures or fracture-like lesions.
Our patients included disproportionate numbers of infants born preterm or as a result of multiple pregnancy. The fractures were mainly identified in the first six months of life and entirely within the first year of life. Most fractures were asymptomatic, particularly the many rib fractures and metaphyseal lesions. 140 fractures were diaphyseal including 81 transverse fractures. Few patients had evidence of bruising at presentation; none had clinical evidence of inflicted injury commensurate with the fractures found.
In several cases fractures took place while the children were in hospital. Unexplained bruising and sub-conjunctival haemorrhages also occurred in hospital, suggesting a collagen defect. Hernias were recorded; in most these resolved spontaneously, again suggesting a transient collagen defect. Among the unexplained symptoms of the patients was a history of vomiting, often projectile vomiting. Some patients had unusually blue or grey sclerae for the child's age. Many patients had abnormally large anterior fontanelles. Laboratory findings included anaemia, neutropenia and an exceptionally high serum alkaline phosphatase.
Our findings reinforce the view that children with temporary brittle bone disease have a distinctive and identifiable disorder and that they are not the victims of non-accidental injury. The potential causes of this disorder including rickets, scurvy and copper deficiency will be discussed. While the causes remain unclear, its characteristic features should be recognised.
P17 The optimal dose of vitamin D in growing girls during academic years: a randomized trial
Samane Tefagh, Mehrdad shakiba, Zahra Nafei 1Shahid Sadoughi University of Medical Sciences, Yazd, Iran
Objectives: Vitamin D is an essential hormone for growth and development of bones in children. Prevalence of vitamin D deficiency is remarkable during childhood and adolescence throughout the world. The aim of this study was to specify the optimal dose of vitamin D in growing girls during an academic year in a sunny city.
Materials and methods: This randomized clinical trial study was carried out in Yazd in the center of Iran in 2007;120 junior high school girls (aged 12-15 years) were randomly divided into 4 groups. Sixty students in groups I and II were initially treated for vitamin D deficiency with 300,000 IU vitamin D3 and then randomly received 50,000 U/monthly or 100,000IU/3 months vitamin D3; 60 other students in groups III and IV received 50,000 IU/3 months and 100,000/3 months from the beginning of the academic year. Medication continued for the entire academic year; 1 month after the last dose, serum 25(OH)D levels were measured.
Results: The mean level of 25 (OH) D was 29.7 ± 4.60 ng/mL in group of 1000 or 2000IU/day would maintain serum 25(OH)D and 30 ± 5.61 ng/mL in group II. Mean serum levels of 25 (OH) D were 15.2 ± 6 ng/mL and 23 ± 6.8 ng/mL for groups III and IV, respectively. (table)
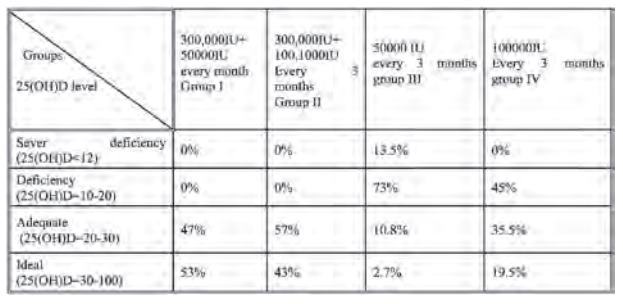
Conclusion: This study shows that in the area with high prevalence of vitamin D deficiency (more than 50%), recommended doses of neither 400IU/day nor 800IU/day are sufficient to maintain optimal level in all. But after treatment of deficiency with 300000IU of vitamin D.both doses
P20 Assessment of vitamin D nutrition status and dietary calcium intake in children 2-5 years of age
Priyanka Kureel, Anju Seth, Ritu Singh, R.K Marwah0, Satvinder Aneja
1Lady Hardinge Medical College, New Delhi, India
Objectives: To assess the vitamin D nutrition status of healthy children in the age group 2-5 years and to assess the daily dietary calcium intake of these children.
Methods: A total of 100 healthy children (age group 2-5 years) were studied in this cross sectional study. Dietary calcium and energy intake was estimated using 24 hour dietary recall method. Average sun exposure over last 3 days was assessed by calculating UV score.
Biochemical parameters assessed included serum calcium (total and ionic), inorganic phosphorous, alkaline phosphatase (ALP), parathormone (PTH) and 25 hydroxy vitamin D (25OHD).
Results: Diet of 32% children provided met the ICMR recommendation of daily dietary calcium intake > 600 mg. 23% children had an adequate vitamin D nutrition status (serum 25OHD >20 ng/ml). Average sun exposure was 21.4 + 19.8 min/day (range 5-120 min). Only 9% children had adequate calcium intake (>600 mg/day) as well as optimal vitamin D status. 54% children did not have either adequate calcium intake or optimal vitamin D status. Serum PTH was elevated in 5% and ALP in 10% cases. Serum ALP was significantly higher in subjects with 25OHD<10 ng/ml. No correlation was observed between serum 25OHD and PTH levels.
Conclusion: Bone health status of children 2-5 years of age is sub-optimal, with prevalence of vitamin D deficiency in 77% & low dietary calcium intake in 68% subjects.
P25 Maternal bone density and rickets in Nigerian children
Jennifer Hsu1, Philip Fischer1, John Pettifor2, Thomas Thacher1
Mayo Clinic, Rochester, MN, USA,23Department of Paediatrics, University of the Witwatersrand and Chris Hani Baragwanath Hospital, Johannesburg, South Africa
Objectives: While nutritional rickets is traditionally associated with vitamin D deficiency, a number of other etiological factors have been proposed, including low calcium intake. Maternal nutrition can affect fetal and infant skeletal growth and development. Our aim was to determine the relationship between maternal bone density and rickets in Nigerian children.
Methods: We measured areal forearm bone mineral density (BMD) in 56 and 131 mothers of children with and without nutritional rickets, respectively. Active rickets was confirmed with radiographs of the wrists and knees. Pregnancy and lactation status were recorded, but bone density measurements were not performed in the first trimester of pregnancy. Using logistic regression, we assessed the association of maternal forearm bone density, controlling for parity, pregnancy and lactation status, duration of most recent breastfeeding, age of menarche, and maternal age with nutritional rickets.
Results: The median (range) age of mothers was 30 y (17-47 y), and parity was 4 (1-12). A total of 36 (19%) were pregnant and 55 (29%) were currently breast feeding. Mean (±SD) distal forearm BMDs were 0.321±0.057 and 0.314±0.052 g/cm2 in mothers of children with and without rickets, respectively (P=0.43). Proximal 1/3 forearm BMDs were 0.719±0.071 and 0.713±0.070 g/cm2, respectively (P=0.58). Bone mineral content and bone area were not significantly different between the two groups. Neither the distal nor proximal 1/3 forearm maternal BMD was associated with nutritional rickets in multivariate logistic regression (P=0.42 and 0.84, respectively). In the adjusted analysis, rickets was associated with shorter duration of breast feeding (OR 0.90 for each additional month; P=0.01) and use of lead-containing eye cosmetics by mothers (OR 4.78; P=0.01). Maternal age, parity, age of menarche, and body mass index were not associated with having had a child with rickets in multivariate analysis.
Conclusion: There was no relationship between maternal BMD and nutritional rickets in children. However, early discontinuation of breast feeding and use of lead-containing eye cosmetics may increase the risk of nutritional rickets in Nigerian children.
P39 Prevalence of Vitamin D deficiency in adolescent Muslim girls attending a school in the UK which adheres to a conservative dress code
S. Lukman1, R. Syahanee2, J. L. Berry3, M. Z. Mughal1
'Royal Manchester Children's Hospital, Central Manchester University Hospitals Foundation NHS Trust, UK, 2Alder Hey Children's NHS Foundation Trust, Liverpool, UK,3 Vitamin D Research Group, Endocrine Sciences, University of Manchester, UK
Aim: To determine the prevalence of vitamin D deficiency among adolescent Muslim girls attending a school in the UK which adheres to a conservative dress code.
Methods: Fifty six (31%) out of 180 girls attending a Muslim High School for Girls [median age 13.2years, (IQR 12.5-13.8 years)] took part in this cross-sectional study. Seventy nine percent (n=45) were of South Asian origin, 3.5% were Black African origin (n=2), 1.8% was Middle Eastern origin (n=1) and 15.8% were other ethnic origin (n=9). The participant's serum concentration of calcium (Ca), phosphate (P), alkaline phosphatase (ALP), parathyroid hormone (PTH) and serum 25-hydroxyvitamin D (25OHD) were measured. Dietary intake of calcium and vitamin D were also estimated.
Results: Fifty-one out of 56(91%) (95% CI 86 to 95) girls were found to be vitamin D deficient (25OHD < 25nmol/L) and 4 out of 56 (7%) (95% CI 5 to 17) were vitamin D insufficient (25nmol/L < 25OHD < 50nmol/L). The median serum concentration of 25OHD was 12.8nmol/L, (IQR 10 to 17 nmol/L). Serum concentration of Ca, P, ALP and PTH were all within the normal limits. The median vitamin D intake was 69 i.u./day, (IQR 29 to 122 i.u./day), which is 17% of the recommended daily intake (400 i.u.). The median dietary calcium intake was 662mg (IQR 456 -860mg), which is four-fifth of the recommended daily intake (800 mg). The median serum 25OHD of subjects taken multivitamin (MV) supplements [median= 17.3nmol/L (IQR 13-26.3)] was (p<0.01) higher than that of subjects not taking MV supplements [11.3nmol/L (IQR 8.8-14)].
Conclusions: All subjects (98%) bar one had vitamin D deficiency (91%) and vitamin D insufficiency (7%). Those taking MV supplements had higher serum 25OHD concentrations, although optimum serum concentrations of >50 nmol/l were not achieved. Further studies are needed to determine the dose of vitamin D supplementation needed to optimise the vitamin D status of these groups of adolescent girls.
P44 A homozygous mutation in the DNA binding domain of human vitamin D receptor causes vitamin D resistant rickets
Bram van der Eerden1, Josine van der Heyden2, Jan Piet Hamburger3, Marijke Schreuders-Koedam1, Patrick Asmawidjaja3, Sabine de Muinck Keizer-Schrama2, Erik Lubberts3, Johannes van Leeuwen1, Stenvert Drop2
'Internal Medicine, 2Pediatric Endocrinology, 3 Rheumatology, Erasmus MC, Rotterdam, The Netherlands
In this case report, we present a brother and sister with hereditary vitamin D resistant rickets (HVDRR). Both children presented at the age of 18 months with severe rickets and elevated serum levels of 1,25-(OH)2D3. They differ from each other in that the girl presented with hypophosphatemia instead of hypocalcemia. Besides, she developed alopecia earlier than the boy and needed more 1,25-(OH)2D3 supplementation. Interestingly, the boy does not require supplementation anymore since the age of 19.
We performed DNA sequencing of both patients along with their 3 siblings and their parents, who are first cousins. Both patients carry a homozygous point mutation (A133G) in the vitamin D receptor (VDR) gene, leading to an amino acid change in the DNA binding domain (K45E). Both parents were heterozygous for the same mutation. We collected skin fibroblasts from the boy. 1,25-(OH)2D3 was unable to inhibit their proliferation (in contrast to a healthy subject). Moreover, 1,25-(OH)2D3 failed to enhance 24-hydroxylase activity and VDR expression. Binding of 1,25-(OH)2D3 to the VDR, however, was not affected in the patient.
Since 1,25-(OH)2D3 plays a role in the innate and adaptive immune system, we screened the 1,25-(OH)2D3 response of peripheral blood mononuclear cells (PBMCs) from the boy, his parents and healthy controls. Both the T helper cell (Th) population-specific transcription of Tbet (Th1), Gata3 (Th2) and Roryt (Th17) as well as production of cytokines, such as interferon (Th1) and interleukins IL-4 (Th2), IL-10 (Th17) and IL-22 (memory T cells) was altered in control PBMCs. No transcriptional or translational changes were observed in the PBMCs from the boy further supporting the inability to respond to 1,25-(OH)2D3.
Collectively, these data show that the A133G mutation in the VDR prevents nuclear binding, which leads to unresponsive 1,25-(OH)2D3 downstream signalling. Although 1,25(OH)2D3 acts on the immune system and has been associated with autoimmune diseases such as diabetes and multiple sclerosis, the patient, who is 1,25-(OH)2D3 insensitive, has no immunopathies but long-term follow-up necessary to monitor this. The treatment independence of the boy may be related to enhanced calcium uptake capacity in the intestine between 15 and 25 years of age, an age range he currently is in. The intriguing differences in onset of alopecia between the boy and the girl as well as their respective reduced serum calcium and phosphate at 18 months of age remain to be scrutinized.
P47 Vitamin D deficiency and structural and functional state of bone tissue in schoolchildren of Ukraine
Vladyslav Povoroznyuk1, O Tyazhka2, Nataliya Balatska1, T Budnik3, I Kubey4, N Haliyash4
'D.F. Chebotarev Institute of Gerontology NAMS Ukraine, Kyiv, Ukraine, 2Bogomolets National Medical University, Kyiv, Ukraine, 3Lugansk State Medical University, Lugansk, Ukraine, 4I Y. Horbachevsky Ternopil State Medical University, Ternopil, Ukraine
Introduction: Vitamin D is an essential material in bone metabolism, and regulation of body minerals. Vitamin D deficiency has various causes, including limitations in sunlight exposure (type of clothing, sunscreen usage, indoor activity), seasonal geographic latitude and altitude, atmospheric pollution, diet, and ageing.
The aim of the work was to determine the frequency of vitamin D deficiency among Ukrainian schoolchildren and its influence on bone mineral density.
Methods: There were examined 304 children aged 10-18 years. The boys consisted 55.0 %. The average age of boys was 12.9±0.2 and girls - 12.4±0.2 yr. old. The study was performed within two months -
October and November 2011, to exclude the influence of seasonal factors on the level of 25(OH)D. Researches included ultrasound densitometry of calcaneus by SAHARA (Hologic), blood chemistry, 25(OH)D and intact parathyroid hormone (iPTH) in plasma were determined by Elecsys 2010. Also, it was evaluated the average content of calcium and vitamin D in the diet form the products consumption frequency questionnaire.
Results: Vitamin D deficiency was founded in 92.2 % of schoolchildren, and vitamin D insufficiency was diagnosed in 6.1 % of cases. Secondary hyperparathyroidism was verified in 0.9 % of children. The average level of consumption of calcium and vitamin D in children was below recommended data, and consisted (Me 649 [488.7; 691.86]) mg/day for calcium and (Me 68.69 [58.45; 117.3]) IU/day for vitamin D.
Children with vitamin D insufficiency had significantly higher data of structural and functional state of bone tissue in comparison with the data of pupils with severe deficiency of vitamin D: stiffness index
105.03±6.12 vs 93.7±2.51 % (p<0.02); BMD 0.574±0.024 vs 0.528±0.019 (p<0.02) and speed of sound 1573.61±6.70 vs 1557.2±5.41 (p<0.01).
Conclusion: High level of vitamin D deficiency (92.2 %), secondary hyperparathyroidism (0.9 %), low data of ultrasound densitometry in severe vitamin D deficient children make doctors to research the effective methods of treatment and prophylactics of revealed disorders.
P60 Failure of free, public vitamin D supplementation program for Quebec infants - temporal trends and significant predictors
Maude Millette1, Atul Sharma1, Hope Weiler1, Odile Sheehy2, Anick Berard2, Celia Rodd1
1McGill University, Montreal, Canada, 2Centre Hospitalier Universitaire Ste-Justine, Montreal, Canada
Over 80% of Quebec woman initiate breastfeeding, and rates of exclusive breastfeeding at 6mo doubled from 2003 (9.7%) to 2009 (19.0%). To prevent deficiency, current recommendations for these infants include 400IU/day of vitamin D. For 20y, Quebec has offered a program of free vitamin D supplements through its public medication insurance plan (RAMQ).
Objective: Program evaluation over the last decade.
Methods: This is a retrospective descriptive analysis of infants born between Jan. 1998 and Dec. 2008. All healthy term infants covered by RAMQ drug plan were eligible; ~30% of pregnant women and infants are covered. Data were extracted from the Quebec Pregnancy Registry linking three databases: RAMQ (diagnoses, medications, SES), MedEcho (hospitalizations), and ISQ (birthweight, SES). Multivariable logistic regression (GEE) examined predictors of participation.
Results: A total of 123,018 infants were eligible. Mean annual prevalence of vitamin D exposure was 17.9%±5.6. Median age at which the first bottle of supplements was obtained was 36 days (range=0-370). The majority (51.0%) obtained only one bottle of fifty doses (median=1, range=1-20). Significant predictors (p<0.05) were prescription by pediatrician (0dds Ratio OR=1.23, with 95% confidence interval CI= 1.19-1.27); increasing maternal age (OR=1.018 per year, CI=1.015-1.021); non-synthesizing season for vitamin D (OR=1.04, CI=1.01-1.07); women living alone (OR=0.87, CI=0.83-0.91), less education (OR 0.88, CI=0.84-0.92) and rural residence (OR 0.94, CI=0.91-0.98). There was also a decline in program participation over time (OR 0.89 per year, CI=0.88-0.90).
Conclusions: Program participation was low and decreased with time. Additional risks for rickets included long delay prior to filling the first prescription, failure to renew, younger mothers, mothers with less education, and care by a non-pediatrician. Overall, poor uptake suggests difficulty in administration of supplements, poor understanding of their potential benefits, or low acceptance of health professionals' advice. New preventive strategies need to be developed to increase long-term vitamin D compliance.
Funded by Montreal Children's Hospital-Research Institute and Gray Family Fund.
P64 The level of vitamin D and calcium in urban pregnant women in Russian Federation
Olga Ershova12. Valentina Dzhalatova2,1, Ksenia Belova1,2, Ekaterina Svetalkina2,1
1Yaroslavl State Medical Academy., Yaroslavl, Russia, 'State Clinical Hospital for Emergency Medical Care n.a. N.V. Solovyev of Yaroslavl Region., Yaroslavl, Russia
Background: Optimal intake of calcium and vitamin D of pregnant women is an important component for the normal course of pregnancy, but here are the contradictory opinions about the case of shortage of the consumption, there is no uniform approach to the appointment of them.
Aim: To assess the level of consumption of alimentary calcium, and characteristic of the status of vitamin D and calcium in blood serum of pregnant women.
Materials and Methods: We examined 80 women at the age of 20-35 years (mean age of 27,12±4,36 year) in the third trimester of pregnancy (gestation 31,71±3,37 weeks) residents of Yaroslavl city, Russian Federation. The average consumption of calcium in foodstuff was estimated according to the tables with norms from Russian guidelines for osteoporosis, 2012. The analysis of calcium and vitamin D (25(OH) vitamin D) in blood samples was carried out during the whole year. The concentration of vitamin D in blood serum was determined by the electrochemiluminescence immunoassay («ECLIA»), the concentration of calcium - by the method of optical density on the unit COBAS 400 PLUS.
Results: The average consumption of calcium in foodstuff was 1148,25 ±368,91 mg per day (from 350 to 2064 mg). 29 (36,25 %) of women consumed less than 1000 mg, less than 1200 mg - 46 (57,50%), more than 1500 mg - only 16 (20,00%) women. The total blood calcium was 2,14 ±0,28 mmol/l (from 1,43 to 2,48 mmol/l). Hypocalcaemia was in 40 (50,00%) of the pregnant women.
The average level of 25(OH) -vitamin D was 26,61±13,69 ng/ml (from 4,10 to 58,16). The normal content ration (more than 30 ng/ml) was detected in 29 (36,25%) of people, insufficiency (from 21 to 29,9 ng/ml) - at 18 (22,50%), deficit (less than 20 ng/ml) - at 33 (41,25%) women. There was no difference in mean concentration of vitamin D in blood samples from different seasons (from OCT to APR - 26,51±11,69 ng/ml, from MAY to SEP -26,79±17,32 ng/ml, p>0,05). The clinical manifestations of the vitamin D deficiency and/or hypocalcaemia were noted in 17 (21,25%) women.
Conclusions: Our data demonstrate the wide prevalence of the deficiency of dietary calcium and low level of vitamin D of the urban pregnant women in the third trimester of pregnancy.
[Summary by VitaminDWiki :Pregnant Russian women (3rd trimester) at 57 degrees lat away from equator 36% >30 ng, 22% 21-30 ng, 41% < 20 ng; not change with season]
P91 Hypovitaminosis D in chronically ill children in Greece and its Management
Damiani Tsiamasfirou1, Charalambos Tsakiropoulos2, Alexandros Vassilakis2, Ioanna Paspati2 Department of PM&R;, KATHospital, Athens, Greece, 'Department of Orthopaedics, Pendeli Children's Hospital, Athens, Greece
Objectives: Study the prevalence of hypovitaminosis D in chronically ill children in Greece, as well the efficacy of a proposed replacement therapy.
Methods: A total number of 213 children(121 males, 92 females), with mean age 10.1 years (1-18), suffering various pathological conditions (cerebral palsy, Duchenne myopathy, epilepsy), were sampled to measure serum 25(OH)D and parameters of bone turnover. 101 children were given replacement therapy according to levels of hypovitaminosis [15-20ng/ml pos ergocalciferol and calcium (4000IU+500mg/day), <15ng/ml intramuscular ergocalciferol (400.000IU) once per month for 2 months combined with pos ergocalciferol and calcium (4000IU+500mg/day)] while 60 children were re-evaluated during the four months follow-up.
Results: The mean serum 25(OH)D was 14.20ng/ml on total (15.5ng/ml for patients<12years old and 12.6ng/ml for patients>12years old), while the highest rate was measured at 44.53ng/ml. Respectively median value for PTH was 48.87pg/ml on total. 34.74% of patients had vitamin D deficiency (10-20ng/ml) while overt vitamin D deficiency (<10ng/ml) was measured in 21.59% of patients of whom 21.73% had less than 4ng/ml. Of the 22 children receiving antiepileptics, 86.34% had vitamin D deficiency. 9% presented secondary hyperparathyroidism. Higher serum PTH levels were observed in the group of 25(OH)D<10ng/ml for both age groups, however the inverse relationship between serum 25(OH)D and PTH was statistically nonsignificant at 25(OH)D levels>10ng/ml. A positive correlation between 25(OH)D and serum phosphorus was also observed (p = 0.003) After replacement therapy, children displayed higher levels of 25(OH)D on total (median 25(OH)D=25.8ng/ml, p<0,0005) and for both age groups(fig1).
P99 Potential association between vitamin D deficiency and hypertension in adolescents: A pilot study
Edyta Babinska-Malec1, Jerzy Konstantynowicz1, Pawel Abramowicz1, Irena Werpachowska1, Malgorzata Bazyluk-Muszynska1, Janina Piotrowska-Jastrzebska1
Medical University of Bialystok, Poland
Objective: Insuficient vitamin D supply defined as serum hydroxyvitamin D (25OHD) less than 20 ng/ml is considered as one of possibile cardiovascular risk factors among adults with hypertension. Furthermore, some data also suggest an independent association between vit. D deficits and hypertension and obesity during growth. The aim of the study was to assess vit. D status in children and adolescents with hypertension.
Methods: The cross sectional study was performed on a group of 99 subjects (43 girls, 56 boys) aged 8.4 - 17.6 years (mean: 12.1), stratified according to their values of blood pressure (BP). Blood samples were taken to determine 25OHD; anthropometric traits and BP measurements were carried out using standard methods and equipment. The study was performed after winter time i.e. in March 2012.
Results: Only 8% of all studied children and adolescents demonstrated vitamin D level above 20 ng/ml, whereas predominantly severe deficits were found (92%). Significant correlations were observed between
25OHD and systolic BP (r= -0.37, p=0.0003) and mean BP (r= -0.3, p=0.002). Children and adolescents with normal systolic BP had better supply with vit. D compared with age- and sex-matched hypertensive pairs i.e. subjects with critically increased systolic BP (> 90 percentile). The association (p=0.03) was independent of age, BMI and anthropometric parameters.
Conclusions: Our findings show associations between decreased levels of serum 25OHD and hypertension in adolescents suggesting potential role of vitamin D deficits in the development of this condition. However, these relationships and possible causal links need to be investigated in further prospective studies including larger groups of pediatric patients.
Fig. Correlation between mean blood pressure (Mean BP) concentration of '5(OH)D in subjects aged 8 - 17 years
P129 Radiographic Evidence of Rapid Healing of Vitamin D Deficient Rickets after 2 weeks of Therapy
Kathryn Stephens1, Sasigarn Bowden1
1Nationwide Children's Hospital/The Ohio State University, Columbus, Ohio, USA
Clinical Management: This patient was started on calcium and ergocalciferol 2000 IU daily for treatment of nutritional vitamin D deficient rickets. Due to his femur fracture, a repeat radiographic film was obtained approximately 2 weeks following his initial injury. Repeat radiographic film demonstrated remarkable resolution in cupping and fraying of the metaphysis. Repeat vitamin D studies 4 months after starting treatment with ergocalciferol demonstrated adequate vitamin D stores with 25-OH vitamin D level of 59 ng/mL and normalization of serum calcium, phosphorous and PTH.
Discussion: This case demonstrates radiographic evidence of rapid healing of vitamin D deficient rickets following initiation of treatment with calcium and ergocalciferol after only 2 weeks of therapy. This is much more rapid than previously demonstrated. Furthermore, this case also demonstrates that vitamin D deficiency can predispose infants to fractures mimicking those caused by non-accidental trauma.
P173 Vitamin D Prescription: A review of British National Formulary for Children recommendations, and a proposal
Andreas Kouklinos1, Julian Lim1, Benjamin Jacobs1
Royal National Orthopaedic Hospital, Stanmore, UK
Aims: To review changes in the advice regarding Vitamin D deficiency in the United Kingdom and compare these with other national guidance.
Methods: All Vitamin D guidance in the Royal College of Paediatrics and Child Health 2003 guide (Medicines for Children) and in the 8 editions since the British National Formulary for Children (BNFc) was first published in 2005 was reviewed.
Results: Dosage and Indications of Prevalence are shown in the Table.
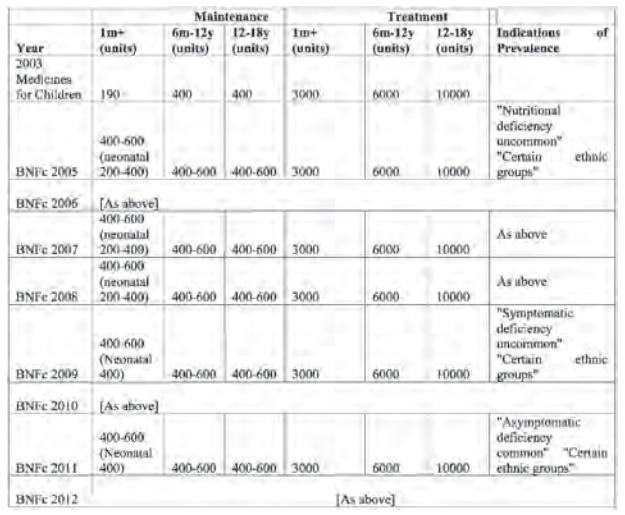
Doses are higher than recommended by the UK Chief Medical Officers in 2005 and 2012. Emphasis in the remarks about prevalence has shifted from "deficiency is uncommon " to "symptoms are uncommon ". Each of the 8 editions has stated that children on treatment doses should have a blood test weekly (or twice weekly) to check calcium levels.
Conclusions: The BNFc portrayal of D Deficiency as an uncommon problem has gradually changed thorough the editions so that since 2011 the high prevalence of asymptomatic deficiency has been acknowledged. However the recommendation that children should have regular blood tests, which is not based on evidence, and is against the consensus of national experts, has remained through the editions. We propose a new clearer national dosage guide in line with the recommendations of the Chief Medical Officer and withdrawal of the recommendation to monitor serum calcium in well children with asymptomatic D Deficiency.
P190 Vitamin D deficiency rickets in neonates
Colin R Paterson, David Ayoub
'University of Dundee (formerly), Dundee, Tayside, UK, Clinical Radiologists
SC, Springfield, Illinois, USA
This paper reviews clinical reports of vitamin D deficiency rickets in neonates from 1930 onwards. In 24 reports there was good evidence of maternal deficiency. In some the diagnosis of the rickets led to the identification of symptomatic osteomalacia in the mothers; several had been severe and longstanding. Of the 15 mothers who had assays for serum 25-hydroxyvitamin D (25OHD) 13 had values < 25 nmol/L (10 ng/mL) and 10 had values < 12.5 nmol/L (5 ng/mL).
Presentations in the infants included craniotabes, wide skull sutures, rachitic rosaries, enlargement of the wrists and ankles, tetany and hypocalcemic convulsions. In three cases rickets had been suspected from antenatal X-rays. In four cases fractures were found at the time of initial presentation. Of the 19 infants with serum calcium assays 12 had values lower than 2.0 mmol/L (8.0 mg/dL). A variety of methods had been used for serum alkaline phosphatase assays but of 18 infants at least 15 had abnormally high levels for a child. Of the 11 infants in whom serum 25OHD was measured before treatment, all had values < 25 nmol/L (10 ng/mL). Eight had values < 12.5 nmol/L (5 ng/mL). Seven infants had assays for serum parathyroid hormone; all had substantially raised values.
These reports provide strong support for the view that maternal deficiency leads to overt bone disease from before birth. Larger surveys have shown that maternal deficiency leads to long-term impairment of bone quality in postnatal life. The importance of ensuring adequate vitamin D nutrition in pregnancy is emphasised.