Benefits of vitamin D experienced then described by retired Biologist
Retired German Biologist had typical problems of elderly

He got lots of vitamin D in 2013 and his health problems went way
He currently takes 50,000 IU vitamin D3 weekly
He researched vitamin D (while retired)
He published the following excellent Vitamin D overview in 2014
Appears that the overview was also published in Russian
Many excellent ideas and observations (VitaminDWiki has bolded some of them)
This version uses an incorrect English word < 1% of the time.
My Vitamin D Story. by Horst Goering
– from http://www.grassrootshealth.net/
Horst Goering, 80+ years
Retired Professor at the Humboldt-University Berlin, Germany
Married 58 years to Svetlana Koshuchowa
2 children, and 3 grandchildren - living in the US and Germany
The beginning, by Horst Goering
During all the years at the university my health was not very good. For this and other reasons I left the university life and applied myself in different fields, years after retirement. My health was sometimes better, sometimes worse. A few years ago (2013), my situation could be described as following:
- Chronic pain in the neck, shoulders, back and right leg.
- Diagnosis: a slipped disk. Surgery was recommended. I declined.
Two or three times a year I had a very heavy flu or cold (4-6 weeks recovery with antibiotics)
Tiredness and intensive nightly sweating
Neurodermitis
Gum inflammation and chronic periodontitis
Shingles (Herpes Zoster) two or three times a year
General weakness and powerlessness
Lack of motivation and signs of depression
Irritable bowel syndrome for more than 50 years
Vitamin D therapy - did it work?
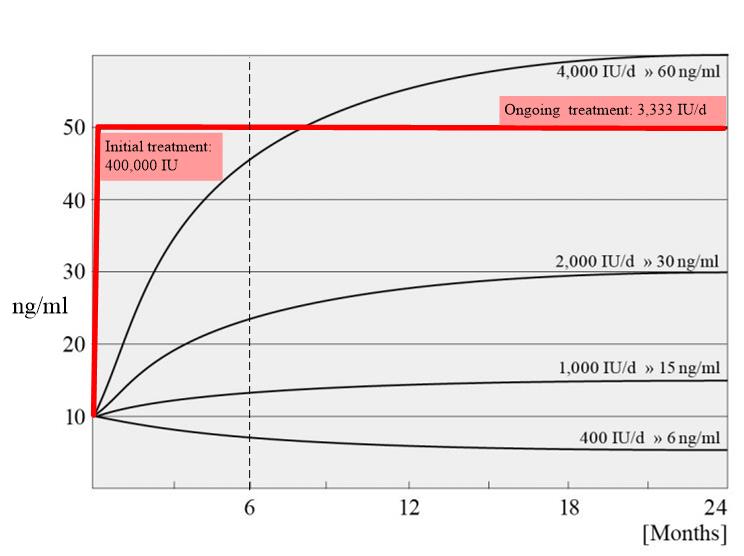
Was it time to go? I was already more than eighty years old and, maybe, that was it? My wife's situation was not much better. In the summer of 2013, both my wife and I had no strength, no drive, just weakness ...! I asked my doctor to check my vitamin D level again. The result: 19.6 ng/ml. At this time my doctor, without hesitation, prescribed Dekristol (20,000 IU vitamin D). I started a vitamin D-therapy according to von Helden. This means, first day - 200,000 IU, then 5 days each time 20,000, later 20,000 IU every third day. After 2-3 weeks I felt already better. (7 weeks later his vitamin D level was 42 ng/ml).
At present, 2 years after the beginning of vitamin D-therapy, we are back to life. I test my vitamin D levels twice a year and they are usually about 70 ng/ml. I take 50,000 IU/week . What happened during that time?
After only 4 days, the pain in the neck and shoulders disappeared
After about 3 weeks, nightly sweating disappeared
After 4 - 6 weeks, gum inflammation and chronic periodontitis was gone
After 6 - 8 weeks, all symptoms of neurodermitis vanished
I no longer suffer from flu or cold
The same is true for shingles (Herpes Zoster)
Even my colon is working quite normal now
Life again!
Vitamin D? I think you can say that I am the living example that it is possible to turn just before the cemetery gate back into the stream of communal living thanks to vitamin D. The same is true for my wife, for our immediate neighbors, for some friends, for a lot of other people who came to my lectures or were reading my flyers and pamphlets, in Germany and in Moscow and even some in the US. Each of us is an individual case - a "meaningless nothing" to the statistic-driven modern medicine. But for me it means everything! It makes the difference between death and life. My life!
Vitamin D proponent and researcher
Since 2013 I have spent all my time studying the hormone cholecalciferol, so-called "vitamin D". I started sharing my knowledge with friends and other people, about what I had read and what my own experiences of its effects on me were. Some hundreds of them improved their quality of life to different degrees after vitamin D-therapy. One of my flyers came to an editor of the journal Biochemistry. At the end of October 2014, I was asked to write a review on vitamin D ; I did not know what to do. At our age? After all we suffered?! Neither my wife nor I have medical training, we are "just" biologists and long retired. Nevertheless, we agreed and you can read this paper.
What would Horst tell a neighbor about vitamin D?
What about vitamin D? It means cholecalciferol, a hormone, the so-called vitamin D. This is a unique compound in nature. We cannot synthesize it by ourselves. There is some amount in our food, at best, about 10% of what we need. But it is synthesized by UV-B-irradiation in our skin if there is enough sunshine. We need it urgently and permanently from our childhood up until old age. An optimal level of vitamin D protects us against 60 to 80% of all age-related diseases, against pain in neck, shoulder, back etc., against cold and flu. Vitamin D regulates our power of resistance.
Publication: Vitamin D - the Sun Hormone. Life in Environmental Mismatch - 2015
Biochemistry (Moscow), 2015, Vol. 80, No. 1, pp. 8-20. © Pleiades Publishing, Ltd., 2015. Received March 23, 2014, Revision received May 15, 2014
Original Russian Text © H. Goring, S. Koshuchowa, 2015, published in Biokhimiya, 2015, Vol. 80, No. 1, pp. 14-28. DOI: 10.1134/S0006297915010022
H. Goring and S. Koshuchowa
Goring Consulting, Mahlsdorfer Strasse 91, De12555 Berlin, Germany; E-mail: horst-goering@online.de
📄 Download the PDF from VitaminDWiki
Abstract—While some representatives of the animal kingdom were improving their biological mechanisms and properties for adapting to ever-changing life conditions, the genus Homo was developing backward: human individuals were losing their adaptation to life areas conquered earlier. Losing step-by-step their useful traits including the body hair cover, the primitive genus Homo retained his viability only under very favorable conditions of the equatorial Africa. Protection from UV radiation danger was provided only by pigmentation of skin, hair, and eyes. However, “impoverished” individuals of this genus gained the ability to walk upright. Their hands became free from participation in movement and became fine tools for producing useful instruments, from the stone knife to the computer. The major consequence of upright movement and hand development became the powerful development of the brain. A modern human, Homo sapiens, appeared capable of conquering very diverse new habitats. The human’s expansion on the Earth occurred somewhat limited by his dependence on vitamin D. His expansion into new areas with lower Sun activity was partially associated with the loss of skin pigmentation. But there is an open question, whether under these new conditions he is satisfactorily provided with vitamin D. This paper discusses the following problems: how can we ensure a sufficient intake of vitamin D, how much does an individual require for his existence and optimal life, what will be consequences of vitamin D deficiency, and what are the prospects for better provision with vitamin D?
VITAMIN D - EVOLUTIONARY BACKGROUND
No life can exist on the Earth without the Sun. Everything on the Earth, from favorable temperature conditions to creation of bioorganic mass and free oxygen in the atmosphere is created only due to the rays of the Sun. In the living world, a number of systems have been created that are capable of using solar radiation, such as photosynthesis in cyanobacteria and plants, regulation of diurnal rhythms by melatonin, etc.
The photoisomerization of some biologically important compounds such as sterols, cholesterol and ergo- sterol, plays a special role. These molecules can be synthesized only in living cells. However, their photoisomerization can occur not only in living cells, but also in organic remains and even simply in a test tube (in vitro) at temperatures above 25°C [1, 2].
The ability to synthesize sterols is thought to be a very ancient property of living organisms because these substances are indispensable components of biological membranes. Sterols and products of their photoisomerization are widely distributed in algae. Microalgae are an important part of the phytoplankton that is the first link in the food chain for the majority of aquatic animals [3]. Therefore, sterols are likely to be found everywhere. There is an impression that vitamin D precursors, cholesterol and ergosterol, also existed in Nature from very ancient times. For formation of vitamin D, only two additional factors are needed: UV radiation for photoisomerization of 7-dehydroxycholesterol to previtamin D, and temperature above 25 °C for thermoisomerization of previtamin D to vitamin D.
In 1989, M. Holick wrote [4] that vitamin D seemed to be one of the first hormones, or even the very first hormone existing on Earth. The phytoplankton species Emiliania huxleyi, which has existed without change in the Sargasso Sea for more than 750 million years, produces ergosterol (provitamin D2) to ~0.1% of its dry matter. On irradiation of this organism with artificial solar light, ergosterol converts to previtamin D2, which rapidly turns to vitamin D2 [4]. Although it was unknown why these early life forms accumulated such a huge amount of provitamin D2, it was supposed that ergosterol could protect the organisms against UVB- and UVC-radiation. Holick also referred to this idea in his later works published in 2003 and 2007 [5, 6].
Certainly, vitamin D2 did not play this role. Most likely, it was its precursor ergosterol, which could not be dissolved in cells in such amount, because it is a fat-soluble substance. In the cells, it can be present mainly as a component of cell membranes. In the membranes, molecules of this sterol are strictly oriented and subjected to photoisomerization under the influence of UV radiation. However, the further thermoisomerization to vitamin D does not occur because the ocean water has a low temperature. The photoisomerization of both ergosterol and cholesterol is reversible, and therefore these sterols are powerful absorbers of UV radiation at temperatures below 25°C.
Thus, in phytoplankton organisms, as in many similar organisms, ergosterol and cholesterol do not function as a prohormone or even a hormone. Photosensitive molecules of ergosterol or cholesterol, together with their s-cis, s-cis-iso- mers, at temperatures below 25°C can serve as powerful systems protecting bioorganic molecules against the damaging effect of UV radiation.
Perhaps both cholecalciferol and ergocalciferol could occur in very early stages of evolution. What functions could they execute in aquatic organisms before their coming onto land? It was unlikely that it was associated with providing their cells with calcium ions because the average Ca2+ concentration in seawater varies near 1.2%. This means that sea organisms live in a medium enriched with calcium ions. Moreover, calcium became the most important element of their outer and inner skeletons. The development and solidity of the skeleton became decisive evolutionary traits and simply the most important prerequisite for coming on land of aquatic organisms. Moreover, fresh water and food found by the neophytes on dry land were essentially poorer in calcium. Therefore, new regulatory mechanisms had to appear to provide a sufficient amount of this cation in blood vessels of these organisms. It is vitamin D that fulfilled this function.
There is clear evidence that for the majority of animals living under conditions of the atmosphere, from amphibians to primates, a vitally indispensable photodependent mechanism of vitamin D synthesis has been elaborated [4].
HUMAN EVOLUTION AND VITAMIN D
During evolution, all organisms acquired some features that promoted their survival in one or another environment, i.e. they adapted to conditions of their existence. However, every new adaptive trait to certain specific conditions automatically limited adaptations to other conditions. That is why every species occupies a strictly determined limited areal on Earth. Consideration of human evolution shows that at a certain stage they began to lose step-by-step various specific adaptations of their ancestors, and, finally, they converted to a “naked ape”! They occurred biologically adapted only to the most favorable life conditions in equatorial regions of Africa and became really “Homo imperfectum”. Let us see if for humans anything occurred from the standpoint of evolution.
The loss by humans of specificity was associated, first, with gaining upright posture for walking that made hands free from participation in movement and provided a unique possibility for development of the brain. This finally created the conditions for converting the hands to a universal organ for making various tools. In turn, this promoted further development of the brain. Humans became “Homo sapiens”.
Using brain and hands, humans gradually conquered all regions of the Earth, lifted into the air, and realized the first steps in mastering space. All they needed humans created themselves! However, for Homo sapiens one limitation remained that made essentially more difficult progress into new regions of the Earth. This limitation was dependence on provision with UV radiation-dependent vitamin D, although they could more or less get this substance with food products. May be just because of this, humans spent nearly one million years to overcome the distance from the Equator to the Mediterranean Sea shore [7].
In the regions of the human origin, solar radiation seemed to be too aggressive for their naked body. But the human ancestors had strongly pigmented skin, hair, and eyes. It is not surprising that our ancestors were black! With expansion into new habitats where the Sun even in summer never rises to the zenith, a significantly less UV radiation reaches the Earth’s surface, especially in winter, and the capability of our ancestors of synthesizing vitamin D decreased significantly. Humans more or less succeeded in adaptation to these new conditions by a decrease in the pigmentation of their skin.
Loomis [8] supposed that the melanin pigmentation was developing under the influence of the solar radiation as a protection against “intoxication” with too high concentration of vitamin D. Later it has been shown that the Sun itself regulates the level of vitamin D that is produced under the influence of solar radiation (see below). Pigmentation prevents the production of vitamin D. The level of vitamin D in blood of white-skinned humans becomes balanced already in 20 min of exposure to UV radiation, whereas in dark-skinned humans the same state is reached after three-six times longer [9, 10].
This is the evidence that human pigmentation is protection against the deleterious effect of UV radiation. When humans had advanced into regions where the Sun did not provide the needed amount of vitamin D, they began also to lose step-by-step this protective function. As a result, they became more sensitive to the damaging effect of UV radiation. In the new habitats, the UV radiation intensity was much lower than in regions near the Equator. This resulted in a kind of compromise: the provision with vitamin D was improved at the cost of worsening skin protection against UV radiation. (This situation has had far-reaching consequences for human life under new conditions, see below).
BRIEFLY ABOUT THE HISTORY OF VITAMIN D
Substances that are now called vitamins usually became known from the consequences of their insufficient supply. The same was in the case of vitamin D. In 1822 , Sniadecki [11] noted that children living in Warsaw became ill with rickets more frequently than children living in the countryside did. He concluded logically that they simply had a shortage of Sun. In 1824, Schuette [12] treated children suffering with rickets with cod-liver oil. Both these publications as well as some later ones were not noticed.
The situation changed sharply when in 1918 Mellanby published results of his experiments on dog puppies [13]. He kept them in the dark and gave them different food. It appeared that the addition to the food of cod-liver oil protected the puppies against the development of rickets. Initially, the curative effect was ascribed to vitamin A. However, in contrast to vitamin A, the curative component of cod-liver oil was thermoresistant. This new substance was termed vitamin D [14]. In experiments of Huldschinsky, children with rickets were irradiated by mercury lamps [15], and after four months, these children became healthy. Moreover, the functions of both hands improved even if only one hand was irradiated.
Results of these studies, as well as using rats as new model experimental animals for treatment of rickets, induced a new wave of investigations in this field. Rats were easily treated for rickets using UV radiation. It was surprising that they became healthy even when they were taken from their cages and the cages were irradiated. Rats with rickets (non-irradiated!) were placed into the irradiated cages and they recovered [16]. Initially the authors thought that a component of the air in the cages was an acting factor. However, later it was found that the recovery of the rats was due to their eating their own excrements and the bedding that were not removed from the cages before the irradiation . Cholesterol and ergosterol of the excrements and bedding under the influence of UV radiation were converted to cholecalciferol and ergocal- ciferol, i.e. vitamins D3 and D2. This is how the rats overcame the vitamin D shortage and recovered [17].
Further studies on vitamin D were characterized by both increase and decrease in interest from time to time. Thus, interest in studies on the role of vitamin D in human life sharply increased after a patent was obtained on its enrichment in irradiated food products [18]. Upon the development of a method for production of a large amount of inexpensive vitamin D2 from yeast cultures, this vitamin began to be added directly into milk (423 IU/ liter) [6]. For a long time, food products, especially milk, were widely enriched with vitamin D2.
Unexpectedly in the 1950s in Great Britain , cases of neonatal hypercalcemia were recorded (British Pediatric Association, 1956 [19]). The situation suddenly changed sharply. Some rather authoritative specialists decided that this was due to overdosing vitamin D in milk . Governments of European countries urgently decided to forbid the enrichment of food products with vitamin D. Since this time, physicians are strongly prejudiced against using vitamin D. However, note that there was no direct proof that these clinical cases were caused only by intoxication with high doses of vitamin D. Symptoms of the illness determined as vitamin D3 hypervitaminosis more likely indicated development of Williams syndrome . This syndrome is characterized by increased sensitivity to vitamin D and is observed very rarely in humans [6].
VITAMINS D ARE UNIQUE COMPOUNDS
Living beings can synthesize all needed organic compounds, but this concerns only the living world as a whole. Humans and other animals cannot produce some compounds and get them only with food, i.e. they utilize products of other organisms. Undoubtedly, such compounds for humans are vitamins. The exception is group D vitamins. Without the UV part of the solar radiation spectrum, no vitamin D would be present on the Earth at all!
If vitamin D precursors, cholesterol (7-dehydrocholesterol) and ergosterol, appear somewhere on Earth, the B ring of these molecules is broken under the influence of solar UV radiation (290-310 nm), previtamin D is produced, and then through thermoisomerization it is converted to cholecalciferol and ergocalciferol, i.e. vitamins D3 and D2, respectively.
Photo isomerization of the 7-dehydrocholesterol molecule dissolved in hexane or other solvents occurs relatively slowly because its intermediate product s-cis,s-cis- previtamin D3 changes to s-trans,s-cis-previtamin D3, and the equilibrium of this reaction is shifted to the latter isomer. In living cells, provitamin D3 is strictly oriented in the membrane, which results in instant conversion of s- cis,s-cis-previtamin D3 to vitamin D3 at sufficiently high temperature [9]. The formation of vitamin D3 is associated with breaking of hydrophilic and hydrophobic interactions with phospholipid compounds of the membranes, and it is released into the intercellular space. Then it is transferred into blood vessels where it is bound to a specific D3-binding protein. Thus, vitamin D3 is constantly removed from the intercellular space, and this maintains a gradient of its concentration [20, 21].
Already at the erythematous dose of solar radiation (slight reddening of the skin 24 h after irradiation), vitamin D3 is synthesized in the skin in the amount equivalent to its taking per os in dose 10,000-25,000 IU [22]. Such powerful production of vitamin D3 would seem to result in its accumulation in the organism in toxic concentrations, but this does not occur. In a human with white skin, level of vitamin D3 reaches a balance already upon 20-30 min of exposure to UV radiation. Vitamin D3 synthesized above this level is not accumulated, but destroyed [23].
These data show that there is a system responsible for regulation of vitamin D3 level in blood directly by UV radiation. Under the influence of UV radiation, previtamin D3 can reconvert to provitamin D3 or other isomers — lumi- sterol3 and tachisterol3. During the next stage, already vitamin D3 is converted to other photoisomers — supersterol I, supersterol II, and 5,6-transvitamin D3. Thus, intoxication of humans with increased dose of vitamin D3 resulting from UV irradiation is completely excluded [24].
The unique properties of vitamins D3 and D2 depend on those of their precursors. For a long time, it was believed that cholesterol was synthesized in animals, and ergosterol in fungi and plants. It seems that ergosterol can be found in plants because of their contamination with fungi or fungal remains . Until now, there is no reliable proof that ergosterol can be synthesized by plants [25]. Sterols play a significant role in both the structure of cell membranes and regulation of their permeability and some other features. Sterols are also precursors of many steroid hormones [26]. Thus, their large amount in Nature is not surprising. Jaepelt and Jacobsen [3] supposed that plant sterols could be synthesized through cycloartenol and cholesterol (in animals) and ergosterol (in fungi) through lanosterol. It is reasonable to think that lanosterol might be a precursor of cholesterol also in plants.
If we admit that cholesterol in plants is not a unique compound but is rather widely distributed, we can expect also the presence of cholecalciferol, i.e. vitamin D3. In fact, the existence of vitamin D3 and its metabolites was discovered because of a disease of herbivorous animals, enzootic calcinosis. This disease is observed in cows, sheep, horses, goats, pigs, and other animals. Animals became ill in both Alpine meadows and South America pastures. This disease was shown to be hypercalcemia because the animals eat plants rich in vitamin D3 and its activated form — calcitriol. In Europe, this disease is caused by the cereal Trisetum flavescens , which is a typical species for the European Alps and Caucasus [27-30]. The toxic effect of this plant is maintained and seems even to increase after drying by sunlight [31].
In South America, toxic effect to some animals is caused by Solanum glaucophyllum . Experiments were performed with rats [32] and rabbits [33, 34]. In the USA another plant from the Solanaceae family, Cestrum diurnum, is dangerous for animals [35]. A hydroxylated form of vitamin D3, 1,25(OH)2D3, is found in both T. flavescens and S. glaucophyllum. The active form of vitamin D3 is often found in these plants at a relatively high concentration. High concentrations of 25(OH)D3 and 1,25(OH)2D3 were found in vitro in S. glaucophyllum cell culture [36].
A question arises whether these three plant species (perhaps their number will be higher if searches are extended or the sensitivity of D3 determination methods is increased) have any evolutionary advantage compared to other species. The situation became still more puzzling after a pathway of vitamin D synthesis was found in an in vitro culture without the influence of UV radiation. In other words, S. glaucophyllum cells in tissue culture and in cell suspension could open ring “B” of 7-dehydroxycho- lesterol in the dark without UV radiation [37]. If this is true, it is sensational! However, no new data have been published from this laboratory and from others for more than 10 years.
Thus, vitamin D precursors are widely distributed throughout the world. Only sunlight is required to break ring “B” in them. The photoisomer previtamin D is produced not only in living cells, but also in their dead remains, anywhere, even in a drop from a pool, especially because living matter dying off is accompanied by releasing cholesterol molecules from membranes. The data indicated that animals including humans usually have two or more chances for obtaining vitamin D. This gives great advantages for conquering new territories.
HOW DO ANIMALS PROVIDE THEMSELVES WITH VITAMIN D?
In the first part of this paper, we mentioned that when animals came onto the land vitamin D began to play an important role in the regulation of blood level of calcium ions. Sources of vitamin D seemed to be UV radiation and food. Five pathways can principally exist for gaining this.
Application of biological products treated by UV radiation. Under the influence of UV radiation, cholesterol and ergosterol are converted into the corresponding previtamins D3 and D2. Photoisomerization beyond the organism was used in many model experiments conducted in vitro [10, 23]. This reaction can be widely distributed in Nature that shown by experiments on rats when UV irradiation even of their excrements and beddings in cages was sufficient to cure the animals from rickets [38, 39].
It was thought for a long time that only products of animal origin and fungi could be sources of vitamin D, but later it was found that plants also contain vitamin D (see [3] for a review). Some plants (Trisetum flavescens, Solanum glaucophyllum, Cestrum diurnum) contain vitamin D3. By the way, nearly 100 years ago rats were treated against rickets by feeding them with UV irradiated grass and hay [40]. Very interesting experiments were performed on the medic Medicago sativa. Long-term treatment of this plant with UV radiation significantly increased level of vitamin D2 in it [2, 40]. Old leaves of adult plants were especially rich in vitamin D2, and with plant aging, the amount of vitamin D2 increased by an order of magnitude [41]. This was due to infection of the plants with fungi.
Thus, wide distribution of various fungi in the plant world is obviously useful for herbivorous animals. It is especially clear after the death of fungi that is associated with releasing a large amount of ergosterol from the cellular membranes. Under the influence of UV radiation, ergosterol is easily converted to vitamin D2.
Coprophagous animals. We already mentioned that rats were easily cured from rickets due to eating their own excrements that had been treated with UV radiation. In Nature, rats mainly eat small animals, and this can fully satisfy their need in vitamin D. Coprophagy is widely distributed among animals. This type of nutrition has been observed in rats, mice, guinea pigs, rabbits, hares, wolves, dogs, horses, elephants, gorillas, etc. It is thought that this provides more complete use of partially digested food (caecotrophy in rabbits) along with assimilation of necessary intestinal bacteria, mineral substances, vitamins, etc. (e.g. a foal eats excrements of its mother). This perhaps provides the organisms with previtamin D and vitamin D3. Whether coprophagy in Nature is significant for providing animals with vitamin D is still unclear.
Carnivorous animals. It is well known that carnivorous animals satisfy their need in vitamin D with meat of their prey because it contains vitamin D3. Though data on vitamin D3 content in different publications vary greatly, they allow us to see that meat is a reliable source of vitamin D3. Especially rich are pluck. The liver and kidneys are places of synthesis of important metabolites of vitamin D3 [42, 43]. Therefore, nutrition with meat products supplies carnivorous animals with a sufficient amount of vitamin D3.
Excretion of cholesterol with fat onto hair coat surface. It is well known that cholesterol is excreted through adipose glands on the hair surface in animals possessing a fell with thick wool. When the animals are warming themselves in the Sun, cholesterol on their wool is converted through photo- and thermoisomerization to vitamin D3, which is licked from the wool and thus enters the gastrointestinal tract and then into blood vessels [44]. In this respect, observations on primates are especially interesting [45]. It is known that they lick not only their own wool, but also the wool of their relatives. This is associated with absorption of vitamin D3 produced from cholesterol and accumulated on the hair coats under the influence of UV radiation [46]. However, perhaps some vitamin D3 can be absorbed directly by the skin [47]. Nevertheless, a significant fraction of vitamin D enters the organism of primates per os. It is interesting that vitamin D3 has been detected also in the sweat of modern humans [46]. Based on these data, Vieth [45] concluded that in the early stages of development humans could also gain vitamin D3 through licking it from their skin. Some animals lick their wool very intensively, which leads to its full disappearance in some places on the body and even to skin inflammation, which is a pathological consequence. However, this can be associated only with insufficient provision of the organism with vitamin D3 (hypovita- minosis, disorders in formation of vitamin D3 receptors), and attempts of the animals to compensates for the shortage of vitamin D [48].
Skin upper layer cells as producers of vitamin D3. We are speaking about the epidermal layers of skin cells. These covering layers do not have blood vessels, but they consist of living cells from which their dying remains are constantly desquamating outwards. Cholesterol is released just into this layer, stratum spinosum, in the neighborhood of melanocytes accumulating a protective pigment. Here, on the outer edge of a living organism, at the very skin surface in its external cells, photo- and thermoisomerization of cholesterol occur. Note that here cholesterol is not dissolved but is in cellular membranes [24].
The calculation per surface unit shows that ~65% of the total cholesterol is located just in the skin epidermis and only 35% in the dermis. More than 95% of previtamin D3 is synthesized just in the skin epidermis [20, 49]. In a white human being (European skin type II), the skin epidermis passes about 20-30% of radiation with wavelength of 295 nm [50, 51]. A significantly lesser amount, 2-5% of this radiation, penetrates through the epidermis of a black human’s skin (skin type V).
PROVISION OF HUMANS WITH VITAMIN D
It was already shown that in the region of their origin humans were fully provided with vitamin D, but on their movement northward they occurred in new regions where the UV radiation level was much lower than in their historical motherland. When humans remained as hunters, they gained some amount of vitamin D as a carnivorous being. However, in regions with another climate they were forced to cover their bodies to protect against cold. Their life mode changed sharply. They began to spend more time in closed places and under shelters built by themselves. Moreover, cultural, social, and religious traditions required them to use clothes. Under new environmental conditions, the humans began to suffer from vitamin D shortage. This was manifested, first, by rickets in children that, by Professor Holick expressed, is only “the top of the iceberg”.
The following questions arise.
1) What is the degree of human provision with vitamin D under current conditions?
2) What amount of vitamin D do humans need for existence at the minimal level and for full-valued life?
3) Under what conditions is vitamin D toxic for humans?
4) What are the consequences of vitamin D shortage?
5) What must be done to provide humans with vitamin D at the optimal level?
Are humans sufficiently provided with vitamin D? Let us proceed from the environmental conditions during the emergence of humans. If we consider now living primates to be somehow related to our ancient ancestors, it is interesting to know their blood level of vitamin D3, especially taking into account that nearly all of them remained in warm Equatorial regions. Unfortunately, these data include those obtained on primates living in zoos: 134 and 33 ng/ml [52], 200 ng/ml [53], 129 ng/ml [54] vitamin D3. For people living under approximately similar geographical conditions and working mainly outdoors, the following data are obtained:
42 ng/ml in medical persons and
54 ng/ml in farmers in Puerto-Rico [55],
65 ng/ml in lifeguards in St.-Louis [56],
59 ng/ml in lifeguards in Israel [57].
Most likely, 55-100 ng/ml is the etalon level for many inhabitants of sunny countries and the aboriginal population of tropical countries [58]. On the other hand, there are many literature data on very low blood level of vitamin D in populations of England, Canada, and other countries. Even in regions with low latitudes, i.e. not far from the Equator, many people suffer from insufficiency of vitamin D and have children with rickets. Materials concerning this problem are discussed in detail in a two-volume edition about vitamin D [59].
Consider data on this problem for Germany as a country with relatively high levels of life and medical care. The provision of the German population with vitamin D is officially represented by data obtained by the Robert Koch Institute in Berlin (the central institution of the federal government for disease prevention). The data were published by the German Society on Nutrition (DGE) based on the decision of the German Bundestag [60]. Altogether, 11,721 persons were examined. The blood level of vitamin D was >30 ng/ml in only 20% of men and women of ages from 18 to 79 years old. In half of this age group, the blood level of vitamin D was lower than 20 ng/ml.
In children and young people, the situation was still worse — a level lower than 20 ng/ml was found in 86%. These data reveal a very strong insufficiency of vitamin D in the young people of Germany. It is especially dangerous that in 4% of German children and young people the blood level of vitamin D is lower than 5 ng/ml. These data characterize changes in the human life nowadays that have been spoken about above. Before considering health problems related with these data, it is necessary to elucidate what blood level of vitamin D3 is needed for humans.
What amount of vitamin D is necessary for humans?
There is no generally adapted opinion about this question among physicians and scientists. The official opinion is that humans gain vitamin D mainly when under the Sun as well as from food products. The lacking part of vitamin D has to be compensated by food supplementation. For a long time it was thought in Germany that it was sufficiently to take 200 IU vitamin D daily, then this dose was increased to 400 IU. In 2013, an official institution increased the recommendation up to 800 IU [61]. This official institution soothes the people by the statement that frequently being under the Sun can provide an acceptable blood level of vitamin D without additional supplements. It is important to note that according to this document, the “desired” blood level of vitamin D is only 20 ng/ml. Obviously, the authors think that the normal level of vitamin D in the organism is such that is not associated with a development of rickets and osteomalacia. There are similar statements about the provision of people with vitamin D in the USA and many other countries.
Certainly, to proceed from the desired blood level of vitamin D3 would be the best, but what is this level? Remember that in people working every day outdoors under the Sun the blood level of vitamin D3 is 54-65 ng/ml, and in populations of sunny countries its level is 55-100 ng/ml (see above). The physician von Helden presented a scale of vitamin D3 blood level [62]:
<12 ng/ml — extreme shortage (risk of rickets and osteomalacia),
<20 ng/ml —significant shortage (risk of osteoporosis, disorders in the vegetative nervous system),
<30 ng/ml — shortage (risk of osteoporosis in old age),
30 ng/ml — satisfactory provision (good absorption of Ca2+),
40 ng/ml — good provision (decreased risk of many diseases),
50-90 ng/ml — the level for regular insolation, the minimal risk of many diseases,
100 ng/ml — recommended upper limit of vitamin D3 blood level,
150 ng/ml — risk of an increased blood level of Ca2+,
300 ng/ml — toxic effect.
Based on his own observations, von Helden concluded that therapy with increased doses of vitamin D3 could cure or at least improve conditions by about 80% in the following states: weakness, chronic somnolence, disorders in blood circulation, insomnia, muscular convulsions, headache, aches in feet and back. Von Helden successfully used his “vitamin D therapy” also in the treatment of other diseases. However, these results cannot be considered reliable because of the limited number of observations.
Other specialists think that vitamin D blood level of 32-50 ng/ml is only satisfactory, of 20-31 ng/ml — insufficient, and <20 ng/ml — deficient [58].
Vitamin D toxicity.
The question of the toxicity of vitamin D is under consideration in discussions about its application. There is no publication concerning the application of vitamin D without a notice about its toxicity even in relatively moderate doses. This situation is mainly a consequence of the enrichment with vitamin D of milk and other food products in European countries.
Cases of vitamin D toxicity were observed on its application in pharmacological doses from 50,000 to 1,000,000 IU per day. This increased blood level of vitamin D above 200 ng/ml [6]. The critical limit of high doses of vitamin D is usually determined by the stability of calcium ion content in blood. Taking vitamin D in the dose of 12,500 IU per day for eight weeks did not influence the blood level of Ca2+ [63]. Later it was shown that on taking vitamin D at the dose of 40,000 IU per day for one month, [Ca2+] in both blood and urine was unchanged [64]. This is in a good agreement with the above-presented classification of von Helden [62].
It is not quite clear why up to now many medical reports stubbornly warn about the threat of taking increased doses of vitamin D. There are warnings even against taking >4000 IU per day as if it is already a significant overdose accompanied by very dangerous consequences. However, there are many data indicating that these statements do not correspond to reality. From the abundance of literature data, we shall present only a few works that show the wrongness of these warnings and allow the reader to have a correct understanding.
VITAMIN D AND ENVIRONMENTAL MISMATCH
Are humans living in an adequate environment? From the evolutionary standpoint, we can boldly say NO! An adequate environment for Homo sapiens is Equatorial Africa. Here they find favorable life conditions if they retain their skin and hair pigmentation. All deviations are already an “environmental mismatch”. Even the loss of the skin pigmentation could only partially improve human adaptation to new life conditions. Moreover, covering the body with clothes, preferential residence in closed rooms, changed food products, etc. — all this is an environmental mismatch from the standpoint of human evolution.
At present, it is aggravated by the development of transport that significantly simplifies human migration. On one hand, many people from Southern regions migrate or were forced earlier to resettle in northern regions: black Africans into America, Mexicans into USA, black Africans and residents of Mediterranean countries into Northern Europe, residents of Asia, Central Asia, and near East into countries of middle and Northern Europe. On the other hand, residents of European and North America countries migrate for a short time (leave, holidays, and temporal work) or even immigrate into countries with excess solar radiation. All this sharply enlarges the circle of people living in environmental mismatch. In the USA, medicine is dealing for long with this problem [65], but in Europe it is not studied enough in spite of its significance. Some results obtained in the USA are presented below. The blood level of vitamin D was determined in men and women of age >70 years for three ethnic groups: white Americans, Mexicans, and Blacks. The blood level of vitamin D <15 ng/ml was found in 5, 13, and 33%, and >30 ng/ml in 27, and 11% of subjects of these ethnic groups, respectively. These data convincingly indicate that the shortage of vitamin D in blood is especially pronounced in the black population and the least expressed in white people [65]. Certainly, such data raise the question about the real consequences of insufficient provision of humans with vitamin D.
VITAMIN D SHORTAGE AND ITS CONSEQUENCES
Symptoms of rickets have been known for a rather long time. The situation is more difficult with many other diseases that can also be caused by insufficient supply of the organism with vitamin D.
It is reasonable to find out some general criteria that would allow systematizing different responses of the organism to shortage of vitamin D. The first group will include all diseases associated with disorders in homeostasis of Ca2+ in blood, i.e. diseases associated with disorders in the normal development of bones. Another group of diseases depending on vitamin D is associated with the immune response of the organism. Many problems in the human health that are also caused by insufficiency of vitamin D are associated with chronic inflammation of different organs. There are also diseases that some authors think to be associated with vitamin D insufficiency, but other authors think they are not.
Significance of vitamin D for development of bones.
Rickets. The appearance of this disease in children has been discussed above. Remember only that the blood level of vitamin D3 above 20 ng/ml reliably protects children against this disease. Moreover, note that vitamin D acts on bone tissues not directly, but through homeostasis of Ca2+ in blood. This also refers to all other bone diseases.
Osteomalacia. There are data indicating that osteomalacia also develops because of vitamin D insufficiency [66-68].
Osteoporosis. About 95% of all cases are classified as primary osteoporosis. The optimal blood level of vitamin D is needed for generation of maximal bone mass beyond youth, and this, in turn, is a prerequisite for preventing primary osteoporosis [69-71].
Growing pains. Children, more frequently at the age of 4-6 and 8-12 years, complain (particularly at night) of bone aches, especially in the legs and sometimes in the arms [72]. In this case, pediatricians usually recommend that parents pay more attention to their children because these are only growth-associated pains, which will disappear soon, but these problems should not be ignored. It is proved that bone density in children suffering with night bone aches in legs is significantly lower than in other children [73]. However, referring to work [74], Evans [72] states that treatment of such children with vitamins C and D or calcium and magnesium ions is inefficient. In fact, in the work of Uziel and Hashkes [74] only one sentence concerns vitamin D: they wrote that nutrition enriched with Ca ions and vitamin D was likely to influence bone conditions and pains, but this theory was not studied. In their recent work, which also considered the growing pain problem, vitamin D was not mentioned. Positive results were obtained from the treatment of two girls (3 and 5 years old) with 5000 IU of vitamin D3 per day [62].
Crooked teeth . It is believed that 70% of all children in Germany have crooked teeth. Crooked teeth in children are corrected with braces that are associated with discomfort, difficulties, and sometimes pain for children. This is a rather expensive treatment, and parents in many countries cannot treat their children because of financial problems. Crooked teeth are mainly a result of insufficient development of jawbones. Jawbones do not reach the necessary thickness, and therefore permanent teeth on their appearance do not find the due place for their orientation. Vitamin D was shown to be very important also for the development of alveolar bones [75, 76]. To realize that vitamin D (or UV radiation) plays a role in the correct development of teeth, one has only to look at smiling faces of African children.
Influence of vitamin D on development of immune reactions.
The innate immune system reacts rapidly but not very specifically, whereas the acquired immune system reacts very specifically but is less active. Some studies have revealed the influence of vitamin D (1,25(OH)2D) on the innate and acquired immune systems [19, 77, 78]. In work [79], vitamin D was shown to be a decisive factor for activation of immune protection. Below we present some examples to illustrate this statement.
Tuberculosis. The influence of vitamin D on the treatment of tuberculosis has been studied in many works [80]. A favorable role of Sun for recovery from tuberculosis has been known for a long time. This disease was widely distributed among poor urban populations. Prosperous people with tuberculosis went to Southern sunny regions, e.g. to Italy. One can see a kind of parallelism with rickets.
Influenza infections. An inverse correlation is shown between the distribution of influenza infections and the Sun’s radiation intensity [81, 82]. In 2008-2009, schoolchildren in Japan were given daily 1200 IU of vitamin D or a placebo during December-March; the morbidity from influenza in the experimental classes was 58% lower [83].
This list can be continued: pneumonia, sepsis, etc. Certainly, these diseases cannot be cured with vitamin D — it only improves the immune response against these infections.
Vitamin D and chronic inflammation.
The organism reacts to infection (with bacteria, viruses, fungi, parasites) or to irritation of tissues (with UV radiation, chemical substances, wounds, etc.) by generating tissue hormones (histamine, serotonin, cytokines, prostaglandins, etc.).
The immune system is activated, and then the organism recovers, or an acute inflammation can become a secondary chronic one. As differentiated from secondary chronic inflammation, primary chronic inflammation develops as an autoimmune inflammation when the immune system attacks cells of its own organism, as is exemplified in cases of arthritis, ulcerative colitis, Crohn’s disease, multiple sclerosis, rheumatoid arthritis, psoriasis, etc. Although patients with these diseases were shown to have a shortage of vitamin D, up to now there are no reliable data on the dependence of these diseases on the organism’s supply with vitamin D [84].
Secondary chronic inflammations are very numerous:
gum diseases (gingivitis, periodontitis, etc.),
asthma, s
ome forms of arthritis,
Alzheimer’s disease,
cardiac diseases,
atherosclerosis,
type 2 diabetes,
Parkinson’s disease,
some intestinal diseases,
neurodermitis, etc.
Sometimes secondary chronic inflammation occurs unrecorded (silent inflammation). Such chronic inflammation can develop for decades and lead to a latent damage to the brain, heart, and nervous system. Chronic inflammation can cause development of serious diseases [85].
During recent years, the number of works increased indicating that the development of these diseases can depend on vitamin D insufficiency or demonstrating the possibility to prevent these diseases with vitamin D. Examples of such diseases are gingivitis [86-88], periodontitis [89, 90], type 2 diabetes [91, 92], cardiovascular diseases [93], and arthritis [94].
A positive effect of vitamin D on the development of these diseases was shown in many works, but in other publications, no positive effect was demonstrated. For other diseases, e.g. for tumors, the results are even more contradictory. A recent review [95] presented results of 46 studies performed during the period from 1985 to 2012. Even first acquaintance with this review reveals that only in 11 of these works was vitamin D used at a dose >1000 IU . The observations in the majority of these works were for no longer than two years; therefore, one could not expect convincing results. Moreover, when cancer diseases were under consideration.
VITAMIN D IS NOT A DRUG, NOT A VITAMIN, IT IS A HORMON
It is unlikely that vitamin D can be considered a drug, a therapeutic agent. More likely, vitamin D as a hormone is a necessary compound for development of the immune system of the organism [96-98].
If so, it would be reasonable to take care of providing the normal status of vitamin D in all people. Physicians of the whole world try to maintain blood pressure and composition in certain limits, but why so little attention is paid to the status of the hormone “vitamin D”?
Even in such a developed country as Germany, nearly 80% of the population is not sufficiently provided with vitamin D. This means that all studies on various medical problems are performed on “sick people”, in any case on people “insufficiently provided with vitamin D”. Vitamin D insufficiency can cause fatigue, morning indisposition, and exhaustion [62]. These manifestations can be pronounced stronger or weaker depending on the vitamin D deficiency degree, individual features of the organism, etc. If so, what is the true value of chronobiological studies performed with such people?
Thus, many diseases are shown to depend on vitamin D level in the organism. Considering that in developed countries nearly 80% of the population is not sufficiently provided with vitamin D, it is surprising that the number of patients with one or another disease is even not higher than it is recorded presently. First, under relatively favorable conditions, humans are not inevitably ill with shortage of this hormone. The organism can adapt to an insufficient provision with various factors. Second, we do not know the number of people with so-called chronic inflammation. In humans of these two groups, any additional load (influenza, stress, etc.) can worsen their health suddenly and sharply. Moreover, many people are suffering from fatigue, nervousness, night sweating, dryness of skin and mucous membranes, neuropathic pains, joint pains, muscular-skeletal pains, paresthesia, absent-mindedness, insomnia, morning constraint, absence of motivation and enthusiasm, indifference, passivity, dissatisfaction, fear, depression, and food cravings. Very often, no organic causes of these states can be found.
Von Helden [62] treated 228 patients suffering from one of the above-listed symptoms. Every patient was given initially 100,000 IU vitamin D3 per day for some days and then 20,000 IU per week.
Even in 17 days,
positive results were observed in 78% of the patients, and
20% the results were estimated as very good and in
26% as good.
The author thinks the states with such symptoms to be associated with a disease of the vegetative nervous system, i.e. to vegetative dystonia. In many cases, these symptoms coincided with symptoms of fibromyalgia. Studies on vitamin D status or its taking revealed the dependence on vitamin D in patients with fibromyalgia [99-101]. But in works [102, 103] the correlation between vitamin D and fibromyalgia was not confirmed. However, in these works the level of vitamin D was far from sufficient in both control and experimental groups.
Other aspects that are consequences of the wide distribution of the above-mentioned symptoms among the population are also interesting. On one hand, many of these symptoms frequently occur in very old people who also have extremely low level of vitamin D. When very old people visit a physician and complain of such symptoms, the physician often speaks that it is common for the patient’s age, and even “if you are older than 65 years and you do not have an ache you are already dead”, but it is possible to improve the state of many such people and sometimes even significantly. The level of vitamin D in these people is very likely to be in the limits of 5-10 ng/ ml, and why not save them from this extremely strong deficiency. It is quite reasonable to expect an improvement of the symptoms in about 80% of the patients!
What is the situation with children and teenagers ? They also have a very low level of vitamin D (5-20 ng/ml, see above), and it is striking that many of the above-mentioned symptoms are widely distributed among these age groups. It is very likely that their
chronic fatigue,
absence of motivation and purposefulness,
tendency for food cravings and obesity,
depressive mood,
flight to the world of narcotics,
uninhibited aggression, and
inclination to violence
cannot be explained only by social reasons. Maybe a biological component also plays a role, e.g. the shortage of vitamin D.
The discussion of different consequences of an increase in the blood level of vitamin D3 leads to the question how the same chemical compound can be involved in such different processes in our organism. First, we are to understand that vitamin D is not a pharmaceutical preparation! Second, vitamin D is not a vitamin! This substance was termed vitamin only because it was found to be an active component of cod-liver oil, which was used for treatment of puppies against rickets [13]. In fact, the so-called vitamin D can be synthesized in our organism, but only under the influence of UV radiation. Chemically, vitamin D is a secosteroid and can be ascribed to steroid hormones based on its biological action. Its major action is mediated through activation of certain genes [96, 104-106, 135], but non-genomic reactions are also described [98, 107].
WHAT MUST BE DONE FOR OPTIMAL PROVISION OF HUMANS WITH VITAMIN D?
It has been said already that vitamin D is present in many food products. However, its concentration in them is rather low. Fatty fish, eggs, and meat are especially rich with vitamin D. Carnivorous animals eat meat in great amount (see above), but people usually can insufficiently satisfy their need for vitamin D with meat. The content of vitamin D in fish and eggs is higher, but it is still too low [59] that to satisfy the need for vitamin D; a human would have to eat daily dozens of eggs or up to 2.5 kg fish. It is necessary to take into consideration how the hens were maintained and fed and whether the fish was caught in the sea or grown in special farms. The level of vitamin D in fishes can vary 4-6-fold [108]. In the best case, on using for nutrition the best opportunities, e.g. buying fish just caught in the open sea, a person can obtain with food only to 20% of their need for vitamin D, but in fact, humans satisfy with food only about 10% of their need in vitamin D. Only people inhabiting the far North or South are exceptions [59]. They do not obtain UV radiation at all.
They really eat only fatty fish and other animals of the Arctic and Atlantic Oceans. The liver of the polar bear is especially rich in vitamin D.
Humans can also obtain vitamin D due to its synthesis in the skin under the influence of UV radiation. We have already considered in detail problems associated with this pathway for present day humans. The question is whether we really want to subject our skin to the influence of UV radiation in the due dose. Our skin is already not pigmented sufficiently to protect us against oncologic diseases. Regular visiting solariums is also not recommended because their sources of UV radiation are often even more oncologically dangerous for white peoples’ skin than solar radiation [109]. However, not all specialists believe that UV radiation has such a great threat of melanoma for humans with white skin [110]. Daily irradiation for no more than 15 min is recommended.
Taking into considering specific conditions of our existence, we cannot satisfy the need in vitamin D with nutrients . Moreover, because for different reasons (religion, traditions, special way of life, cancerophobia, etc.), many people are also unable to synthesize it in the skin under the influence of UV radiation!
The only thing to be done is addition of vitamin D to
food products, e.g. enrichment of milk and milk products with vitamin D3 or D2 as it is done already in many countries (USA, Iceland, Sweden, Finland, France) [111],
using vitamin D capsules (each capsule contains from 3000 to 5000 IU) (USA, France, Netherlands, etc.),
using pharmaceutical preparations such as Dekristol 20000, Drisdol 50000, Pro D3 30000, Vitamin D3 20000, Sterogyl 20000, Zymad 10000, etc.
It would be reasonable to create in the future new agricultural products with increased concentration of vitamin D [25]. New cultivars of rice, wheat, soya, and other plants, which are major agricultural food products, would be capable of satisfying the basic need of humans for vitamin D that would be especially important for inhabitants of the developing countries.
REFERENCES
Goldblatt, H. (1924) Experimental rickets in rats on a purified synthetic diet deficient in phosphorus and fat-soluble organic factor, Biochem. J., 18, 414-488.
Hess, A. F., and Weinstock, M. (1924) Antirachitic properties imparted to inert fluids and to green vegetables by ultraviolet irradiation, J. Biol. Chem., 62, 301-313.
Jaepelt, R. B., and Jacobsen, J. (2013) Vitamin D in plants. A review of occurrence, analysis, and biosynthesis, Front. Plant Sci., 4, 136.
Holick, M. F. (1989) Phylogenetic and evolutionary aspects of vitamin D from phytoplankton to humans, in Vertebrate Endocrinology: Fundamentals and Biomedical Implications (Pank, P. K. T, and Schreibman, M. P., eds.) Academic Press, Orlando, FL, pp. 7-43.
Holick, M. F. (2003) Vitamin D: a millenium perspective, #J. Cell Biochem., 88, 296-307.
Holick, M. F. (2007) Vitamin D deficiency, N. Engl. J. Med, 357, 266-281.
Ingman, M., Kaessman, H., Paabo, S., and Gyllensten, U. (2000) Mitochondrial genome variation and the origin of modern humans, Nature, 408, 708-713.
Loomis, F. (1967) Skin-pigment regulation of vitamin D biosynthesis in man, Science, 157, 501-506.
Holick, M. F., Tian, X. Q., and Allen, M. (1995) Evolutionary importance for the membrane enhancement of the production of vitamin D3 in the skin of poikilother- mic animals, Proc. Natl. Acad. Sci. USA, 92, 3124-3126.
Chen, T C., Chimeh, F., Lu, Z., Mathieu, J., Person, K. S., Zhang, A., Kohn, M., Martinello, S., Berkowitz, R., and Holick, M. F. (2007) Factors that influence the cutaneous synthesis and dietary sources of vitamin D, Arch. Biochem. Biophys., 460, 213-217.
Mozolowski, W. (1939) Jedrzei Sniadecki (1768-1883) on the cure of rickets, Nature, 143, 121.
Schuette, D. (1824) Beobachtungen uber den Nutzen des Berger Lebertrans, Arch. Med. Erfahr., 2, 79-92.
Mellanby, T. (1918) The part played by an “accessory factor” in the production of experimental rickets, J. Physiol., 52, 11-14.
McCollum, E. F., Simonds, M., Becker, J. E., and Shipley, P. G. (1922) Studies on experimental rickets and experimental demonstration of the existence of a vitamin which promotes calcium deposition, J. Biol. Chem., 53, 293-312.
Huldschinsky, K. (1919) Heilung von Rachitis durch kuen- stliche Hoehensonne, DTWDtsch. Tieraerztl. Wochenschr., 45, 712-713.
Humme, E. M., and Smith, H. H. (1923) The effect of air, which has been exposed to the radiations of the mercury-vapor quartz lamp, in promoting the growth of rats, fed on a diet deficient in fat-soluble vitamins, Biochem. J., 17, 364-372.
Jones, J. H., Steenbock, H., and Nelson, M. T (1924) The comparative amounts of vitamin A and antirachitic factor in butter fat and cod liver oil, J. Metab. Res., 6, 169-187.
Schneider, H. A. (1973) Harry Steenbock (1886-1967) — a biographical sketch, J. Nutr., 103, 1233-1247.
Holick, M. F. (2006) Resurrection of vitamin D deficiency and rickets, J. Clin. Invest., 116, 2062-2072.
Holick, M. F., MacLaughlin, J. A., Clark, M. B., Holick, S. A., Potts, J. T, Jr., Anderson, R. R., Blank, I. H., Parrish, J. A., and Elias, P. (1980) Photosynthesis of previtamin D3 in human skin and the physiologic consequences, Science, 210, 203-205.
Tian, X. Q., Chen, T. C., Matsuoka, L. Y., Wortsman, J., and Holick, M. F. (1993) Kinetic and thermodynamic studies of the conversion of previtamin D3 to vitamin D3 in human skin, J. Biol. Chem., 268, 14888-14892.
Holick, M. F. (2004) Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease, Am. J. Clin. Nutr., 79, 362-371.
Holick, M. F. (1995) Environmental factors that influence the cutaneous production of vitamin D, Am. J. Clin. Nutr., 61, 638-645.
Chen, T. C., Lu, Z., and Holick, M. F. (2013) Photobiology of vitamin D, in Vitamin D. Physiology, Molecular Biology, and Clinical Applications (Holick, M. F., ed.) Human Press Inc., N. Y, pp. 35-60.
Fitzpatrick, T. B., Basset, G. J. C., Borel, P, Carrari, F, DellaPenna, D., Fraser, D. P, Hellmann, H., Osorio, S., Rothan, C., Valpuesta, V., Caris-Vyrat, C., and Ferni, A. R. (2012) Vitamin D deficiencies in humans: can plant science help for certain vitamins, namely A, B and E, viable strategies to enhance the overall levels of these metabolites in plants have been presented, Plant Cell, 24, 395-414.
Piironen, V., Lingsay, D. G., Miettinen, T. A., Toivo, J., and Lampi, A. M. (2000) Plant sterols: biosynthesis, biological function and their importance to human nutrition, J. Sci. FoodAgric., 80, 939-966.
Dirksen, G., Plank, P, Spiess, A., Hanichen, T, and Daemmrich, K. (1970) Ueber eine enzootische Kalzinose beim Rind. 1. Klinische Beobachtungen und Untersuchungen, DTW Dtsch. Tieraerztl. Wochenschr., 77, 321-338.
Bensch, C., and Steng, G. (1999) Kalzinose beim Schaf — ein Fallbericht, Tieraerztl. Praxis, 27, 83-86.
Dirksen, G., Steer, K., and Herrmanns, W. (2003) Enzootische Kalzinose beim Schaf nach Verzehr von Goldhafer (Trisetum flavescens), DTW Dtsch. Tieraerztl. Wochenschr., 110, 475-483.
Mello, J. R. (2003) Calcinosis — calcinogenetic plants, Toxicon, 41, 1-12.
Lichtenegger, E., Kutschera, L., Koehler, H., and Libiseller, R. (1979) Zur Kalzinose der Rinder in Oesterreich. VIII. Untersuchungen ueber die Zusammenhaenge zwischen Kalzinose, Klima, Boden und Duengung in Kals in Osttirol, Zentralbl. Veterinaermed. A, 26, 290-308.
Uribe, A., Holick, M. F., Jorgensen, N. A., and DeLuca, H. F. (1974) Action of Solanum malacoxylon on calcium metabolism in the rat, Biochem. Biophys. Res. Commun., 58, 257-262.
Mautalen, C. A. (1972) Mechanism of action of Solanum malacoxylon upon calcium and phosphate metabolism in the rabbit, Endocrinology, 90, 563-568.
Dallorso, M. E., Gil, S., Pawlak, E., Lema, F, and Marquez, A. (2008) 1,25(OH)2 vitamin D concentration in the plasma of Solanum glaucophyllum intoxicated rabbits, Aust. Vet. J, 79, 419-423.
Wasserman, R. H., Corradino, R. A., and Krook, L. P (1975) Cestrum diurnum: a domestic plant with 1,25-dihy- droxycholecalciferol-like activity, Biochem. Biophys. Res. Commun., 62, 85-91.
Curino, A., Milanesi, L., Benasatti, S., Skliar, M., and Boland, R. (2001) Effect of culture conditions on the synthesis of vitamin D3 metabolites in Solanum glaucophyllum grown in vitro, Phytochemistry, 58, 81-89.
Curino, A., Skliar, M., and Boland, R. (1998) Identification of 7-dehydrocholesterol, vitamin D3, 25(OH)-vitamin D3 and 1,25(OH)2-vitamin D3 in Solanum glaucophyllum cultures grown in absence of light, Biochim. Biophys. Acta, 1425, 485-492.
Steenbock, H., and Black, A. (1924) The induction of growth-promoting and calcifying properties in a ration by exposure to ultraviolet light, J. Biol. Chem., 61, 408-422.
Nelson, M. T, and Steenbock, H. (1925) Observations bearing on the alleged induction of growth-promoting properties in air by irradiation with ultraviolet light, J. Biol. Chem., 62, 575-593.
Steenbock, H., Hart, E. B., Elvehjem, C. A., and Kletzin, S. W. F (1925) Dietary factors influencing calcium assimilation, J. Biol. Chem., 61, 425-441.
Jaepelt, R. B., Didion, T, Smedsgaard, J., and Jacobsen, J. (2011) Seasonal variation of provitamin D2 and vitamin D2 in perennial reygrass (Lolium perenne L.), J. Agricult. Food Chem, 59, 10907-109012.
Schmid, A., and Walther, B. (2013) Natural vitamin D content in animal products, Adv. Nutr., 4, 453-462.
Calvo, M. S., Whiting, S. J., and Barton, C. N. (2004) Vitamin D fortification in the United States and Canada: current status and data needs, Am. J. Clin. Nutr., 80, 1710-1716.
Carpenter, K. J., and Zhao, L. (1999) Forgotten mysteries in the early history of vitamin D, J. Nutr., 129, 923-927.
Vieth, R. (2003) Effect of vitamin D on bone and natural selection of skin color: how much vitamin D nutrition are we talking about, in Bone Loss and Osteoporosis: An Anthropological Perspective (Agarwal, S. C., and Stout, S. D., eds.) Kluwer Academic/Plenum Publishers, N. Y., pp. 135-150.
Bicknell, F, and Prescott, F. (1946) Vitamin D. The antirachitic or calcifying vitamin, in Vitamins in Medicine (Bicknell, F, and Prescott, F, eds.) Whitefriars Press, London, pp. 630-707.
Fraser, D. R. (1983) The physiological economy of vitamin D, Lancet, 1, 969-972.
Kalueff, A. V., Minasyan, A., Keisala, T, Kunslathi, M., and Tuohimaa, T. (2014) Vitamin D as a neurosteroid hormone: from neurobiological effects to behavior, in Vitamin D: New Research (Stoltz, V. D., ed.) Nova Science Publisher, N. Y, pp. 29-65.
Havinga, E. (1973) Vitamin D, example and challenge, Experientia, 29, 1181-1193.
Anderson, R. R., and Parrish, J. A. (1982) Optical properties of human skin, in The Science of Photomedicine (Regan, J. D., and Parrish, J. A., eds.) Plenum Press, N. Y, pp. 147-194.
MacLaughlin, J. A., and Holick, M. F. (1983) Photobiology of vitamin D in the skin, in Biochemistry and Physiology of the Skin (Goldsmith, L. A., ed.) Oxford, N. Y., pp. 734-754.
Adams, J. E., Gacad, M. A., Baker, A. J., and Rude, R. K. (1985) Serum concentrations of 1,25-dihydroxyvitamin D3 in Platyrrhini and Catharrhini: a phylogenetic appraisal, Am. J. Primatol., 9, 219-224.
Vieth, R., Kessler, M. J., and Pritzker, K. P (1987) Serum concentrations of vitamin D metabolites in Cayo Santiago rhesus macaques, J. Med. Primatol., 16, 349-357.
Ott, S. M., Lipkin, E. W, and Newell-Morris, L. (1999) Bone physiology during pregnancy and lactation in young macaques, J. Bone Miner. Res., 14, 1779-1788.
Haddock, L., Corcino, J., and Vazquez, M. D. (1982) 25(OH)D serum levels in the normal Puerto Rican population and in subjects with tropical sprue and parathyroid disease, PR Health Sci. J., 1, 85-91.
Haddock, L., and Kyung, J. C. (1971) Competitive proteinbinding radioassay for 25-hydroxycholecalciferol, J. Clin. Endocrinol., 33, 992-995.
Better, O. S., Shabtai, M., Kedar, M., Melamud, A., Berenheim, J., and Chaimovitz, C. (1980) Increased incidence of nephrolithiasis in lifegards in Israel, in Phosphate and Minerals in Health and Disease, Plenum Press, N. Y., pp. 467-472.
Grant, W. B., and Holick, M. F. (2005) Benefits and requirements of vitamin D for optimal health: a review, Altern. Med. Rev., 10, 94-111.
Holick, M. F. (2013) Vitamin D and health: evolution, biologic functions, and recommended dietary intakes for vitamin D, in Vitamin D. Physiology, Molecular Biology, and Clinical Applications (Holick, M. F., ed.) Humana Press Inc., N. Y, pp. 3-33.
Hintzpeter, B., and Volkert, D. (2011) Vitamin D — Versorgung in Deutschland, in Vitamin D und praevention ausgewaehlter chronischer Krankheiten (Ernaehrung, D. G. E., ed.) Umschau Verlag, Bonn, pp. 7-10.
Ernaehrung, D. G. E. (2013) Vitamin D, in Referenzwerte fuer die Naehrstoffzufuhr (Ernaehrung, D. G. E., ed.) Umschau-Verlag, Bonn, pp. 78-96.
Von Helden, R. (2014) Healthy in Seven Days. Success through Vitamin D Treatment, Hygeia Publisher, Dresden.
- See reference at the bottom of this page
Heaney, R. P. (2003) Quantifying human calcium absorption using pharmacokinetic methods, J. Nutr., 133, 1224-1226.
Kimpball, S. M., and Vieth, R. (2007) A comparison of automated methods for the quantitation of serum 25- hydro xyvitamin D and 1,25-dihydroxyvitamin D, Clin. Biochem., 40, 1305-1310.
Weisberg, P, Scanlon, K. S., Ruowei, L., and Cogswell, M. E. (2004) Nutritional rickets among children in the United States: review of cases reported between 1986 and 2003, Am. J. Clin. Nutr, 80, 1697-1705.
Hill, T. R., Aspray, T. J., and Francis, R. M. (2013) Vitamin D and bone health outcomes in older age, Proc. Nutr. Soc., 72, 372-380.
Mac-Way, F., Azzouz, L., Noel, C., and Lafarge-Proust, M. H. (2014) Osteomalacia induced by vitamin D deficiency in hemodialysis patients: the crucial role of vitamin D correction, J. Bone Miner. Metab., 32, 215-219.
Bhan, I., Tamez, H., and Thadhani, R. (2013) Role of vitamin D and vitamin D analogs for bone health and survival in chronic kidney disease, in Vitamin D. Physiology, Molecular Biology, and Clinical Application (Holick, M. F., ed.) Humana Press, N. Y., pp. 955-965.
Koo, W., and Walyat, N. (2013) Vitamin D and skeletal growth and development, Curr. Osteopor. Rep., 11, 188-193.
Holick, M. F., Binkley, N. C., Bischoff-Ferrari, H. A., Gordon, M. C., Hanley, D. A., Heaney, R. P, Murad, M. H., and Weaver, C. M. (2012) Guidelines for preventing and treating vitamin D deficiency and insufficiency revisited, J. Clin. Endocrinol. Metab., 97, 2062-2072.
Sohl, E., van Schoor, N. M., de Jongh, R. T, Visser, M., Deeg, D. J., and Lips, P (2013) Vitamin D status is associated with functional limitations and functional decline in older individuals, J. Clin. Endocrinol. Metab., 98, 1483-1490.
Evans, A. M. (2008) Growing pains: contemporary knowledge and recommended practice, J. Foot Ankle Res., 1, 4.
Hashkes, P J., Gorenberg, M., Oren, V., Friedland, O., and Uziel, Y. (2005) “Growing pains” in children are not associated with changes in vascular perfusion patterns in painful regions, Clin. Rheumatol., 24, 342-345.
Uziel, Y., and Hashkes, P J. (2007) Growing pains in children, Pediatr. Rheumatol. Online J., 5, 5.
Davideau, J. L., Lezot, F., Kato, S., Bailleul-Forestier, I., and Berdal, A. (2004) Dental alveolar bone defects related to vitamin D and calcium status, J. Steroid Biochem. Mol. Biol., 89-90, 615-618.
Hujoel, P P (2013) Vitamin D and dental caries in controlled clinical trials: systematic review and meta-analysis, Nutr. Rev., 71, 88-97.
. Cantorna, M. T. (2006) Vitamin D and its role in immunology: multiple sclerosis, and inflammatory bowel disease, Progr. Biophys. Mol. Biol., 92, 60.
. DeLuca, H. F., and Cantorna, M. T (2001) Vitamin D: its role and uses in immunology, FASEB J., 15, 2579-2585.
. Von Essen, M. R., Kongsbak, M., Schjerling, P, Olgaard, K. , Odum, N., and Geisler, C. (2010) Vitamin D controls T cell antigen receptor signaling and activation of human T cells, Nature Immunol., 11, 344-349.
. Liu, P. T, Hewison, M., and Adams, J. S. (2013) Vitamin D and the innate immunity, in Vitamin D. Physiology, Molecular Biology, and Clinical Application (Holick, M. F., ed.) Humana Press, N. Y., pp. 297-310.
. Cannel, J. J., Vieth, R., Umhau, J. C., Holick, M. F., Grant, W. B., Madronnich, S., Garland, C. F., and Giovannucci, E. (2006) Epidemic influenza and vitamin D, Epidemiol. Infect., 134, 1129-1140.
. Aloia, J. F., and Li-Ng, M. (2007) Re: epidemic influenza and vitamin D, Epidemiol. Infect., 135, 1095-1096, author reply 1097-1098.
. Urashima, M., Segawa, T., Okazaki, M., Kurihara, M., Wada, J., and Ida, H. (2010) Randomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildren, Am. J. Clin. Nutr., 91, 1255-1260.
. Papa, H. M., Gordon, C. M., Saslowsky, T. M., Zholudev, A., Horr, B., Shih, M. C., and Grand, R. J. (2006) Vitamin D status in children and young adults with inflammatory bowel disease, Pediatrics, 118, 1950-1961.
. Broedlein, I. (2006) Onkologie: Wie chronische Entzuendungen zu Krebserkrankungen fuehren, Dtsch. Aerztebl., 103, A592/B512/C492.
. Dietrich, T, Nunn, M., Dawson-Hughes, B., and Bischoff-Ferrari, H. A. (2005) Association between serum concentrations of 25-hydroxyvitamin D and gingival inflammation, Am. J. Clin. Nutr., 82, 575-580.
. Hiremath, V. P, Rao, C. B., Najak, V., and Prasad, K. V. (2013) Anti-inflammatory effect of vitamin D on gingivitis: a dose response-randomized controlled trial, Indian J. Public Health, 57, 29-32.
. McMahon, L., Schwartz, K., Yilmaz, O., Brown, E., Ryan, K., and Diamond, G. (2011) Vitamin D-mediated induction of innate immunity in gingival epithelial cells, Infect. Immun., 79, 2250-2256.
. Stein, S. H., and Tipton, D. A. (2011) Vitamin D and its impact on oral health — an update, J. Tenn. Dent. Assoc., 91, 30-33.
. Joensson, D., Aggarwal, P, Nilsson, B. O., and Demmer, R. T. (2013) Beneficial effects of hormone replacement therapy on periondontitis are vitamin D associated, J. Periodontal., 84, 1048-1057.
. Riek, A. E., Oh, J., Darwech, I., Moynihan, C. E., Bruchas, R. R., and Bernal-Mizrachi, C. (2013) 25(OH)vitamin D suppresses macrophage adhesion and migration by downregulation of ER stress and scavenger receptor A1 in type 2 diabetes, J. Steroid Biochem. Mol. Biol., doi: 10.1016.
. Jehle, S., Lardi, A., Felix, B., Hulter, H. N., Stettler, C., and Krapf, R. (2014) Effect of large doses of parenteral vitamin D on glycemic control and calcium/phosphate metabolism in patients with stable type 2 diabetes mellitus: a randomized, placebo-controlled, prospective pilot study, Swiss Med. Wkly., 144, w13942.
Carbone, L. D., Rosenberg, E. W., Tolley, E. A., Holick, M. F., Hughes, T A., Watsky, M. A., Barrow, K. D., Chen, T. C., Wilkin, N. K., Bhattacharya, S. K., Dowdy, J. C., Sayre, R. M., and Weber, K. T. (2008) 25-Hydroxyvitamin D, cholesterol, and ultraviolet irradiation, Metabolism, 57, 741-748.
Kostik, M. M., Smirnov, A. M., Demin, G. S., Scheplyagina, L. A., and Larionova, V. I. (2014) Juvenile idiopathic arthritis patients and their skeletal status: possible role of vitamin D receptor gene polymorphism, Mol. Biol. Rep, 41, 1937-1943.
Boland, R., Grey, A., Gamble, C. D., and Reid, I. R. (2014) The effect of vitamin D supplementation on skeletal, vascular, or cancer outcomes: a trial sequential metaanalysis, Lancet Diabetes Endocrinol., 2, 307-320.
Mocanu, V., Oboroceanu, T, and Zugun-Eloae, F. (2013) Current status in vitamin D and regulatory T cells- immunological implications, Rev. Med. Chir. Soc. Med. Nat. Iasi, 117, 965-973.
Wang, Q., He, Y., Shen, Y., Zhang, Q., Chen, D., Zuo, C., Qin, J., Wang, H., Wang, J., and Yu, Y. (2014) Vitamin D inhibits COX-2 expression and inflammatory response by targeting thioesterase superfamily member 4, J. Biol. Chem, 289, 11681-11694.
Moukayed, M., and Grant, W B. (2013) Molecular link between vitamin D and cancer prevention, Nutrients, 5, 3993-4021.
Matthana, M. H. (2011) The relation between vitamin D deficiency and fibromyalgia syndrome in women, Saudi Med. J, 32, 925-929.
Olama, S. M., Senna, M. K., Elarman, M. M., and Elhawary, G. (2013) Serum vitamin D level and bone mineral density in premenopausal Egyptian women with fibromyalgia, Rheumatol. Int., 33, 185-192.
Mody, G. M., and Brooks, P. M. (2012) Improving musculoskeletal health: global issues, Best Pract. Res. Clin. Rheumatol., 26, 327-349.
Tandeter, H., Grynbaum, M., Zuili, I., Shany, S., and Shvartzman, P. (2009) Serum 25-OH vitamin D levels in patients with fibromyalgia, Isr. Med. Assoc. J., 11, 339342.
McBeth, J., and Mulvey, M. R. (2012) Fibromyalgia: mechanisms and potential impact of the ACR 2010 classification criteria, Nat. Rev. Rheumatol., 8, 108-116.
Eyles, D. W., Liu, P. Y., Josh, P, and Cui, X. (2014) Intracellular distribution of the vitamin D receptor in the brain: comparison with classic target tissues and redistribution with development, Neuroscience, 268C, 1-9.
Dowd, D. R., and McDonald, P. N. (2013) The molecular biology of the vitamin D receptor, in Vitamin D. Physiology, Molecular Biology, and Clinical Applications (Holick, M. F., ed.) Humana Press, N. Y., pp. 135152.
Carlberg, C. (2013) Diversity of vitamin D target genes, in Vitamin D. Physiology, Molecular Biology, and Clinical Applications (Holick, M. F., ed.) Humana Press, N. Y., pp. 255-274.
Blomberg, J. M., Jensen, M., and Dissing, S. (2012) Non- genomic effects of vitamin D in human spermatozoa, Steroids, 77, 903-909.
Calvo, M. S., and Whiting, S. J. (2013) Determinants of vitamin D intake, in Vitamin D. Physiology, Molecular Biology, and Clinical Applications (Holick, M. F., ed.) Humana Press, N. Y, pp. 361-382.
Ting, W, Schultz, K., Cac, N. N., Peterson, M., and Walling, H. W. (2007) Tanning bed exposure increases the risk of malignant melanoma, Int. J. Dermatol., 46, 12531257.
Holick, M. F., and Jenkins, M. (2009) The UV Advantage, J. Boylston and Company, N. Y.
Mosekilde, M. (2013) Vitamin D deficiency and its health consequences in Northern Europe, in Vitamin D. Physiology, Molecular Biology, and Clinical Applications (Holick, M. F., ed.) Humana Press, N. Y., pp. 435-451.
See also VitaminDWiki
Free Vitamin D evaluation service Von Helden
Increasing German levels of vitamin D to 30 ng could save 18,300 lives annually - Dec 2009 Von Helden
Healthy in Seven Days - Loading dose of Vitamin D – book 2014 Von Helden