Chronic Kidney Disease and Vitamin D Analogs – commentary
Shining light on vitamin D trials in chronic kidney disease
Kidney International (2013) 83, 198–200; doi:10.1038/ki.2012.415
Sagar U Nigwekar1,2 and Ravi I Thadhani1
1 Division of Nephrology, Massachusetts General Hospital, Boston, Massachusetts, USA
2 Scholars in Clinical Science Program, Harvard Medical School, Boston, Massachusetts, USA
Correspondence: Ravi I. Thadhani, Bulfinch 127, Massachusetts General Hospital, 55 Fruit Street, Boston, Massachusetts 02114, USA. E-mail: rthadhani@partners.org
Vitamin D compounds may have extraskeletal functions. Chronic kidney disease (CKD) offers an opportunity to investigate these actions, as vitamin D deficiency is prevalent in this population and actions of vitamin D such as those on the heart and glucose metabolism are highly relevant. However, recent randomized controlled trials have tempered enthusiasm. We appraise a trial by de Boer et al. that addresses effects of paricalcitol on glucose metabolism in CKD, and offer perspectives on future trials.
Chronic kidney disease (CKD) continues to be a modern-day epidemic, and it is associated with significant morbidity and mortality.1 Although there is an abundance of experimental animal studies as well as clinical cross-sectional and longitudinal studies in this field, well-designed and adequately powered randomized controlled trials (RCTs) evaluating specific interventions remain relatively scarce.2 In this regard, the RCT reported by de Boer et al.3 (this issue) is certainly a step in the right direction.
CKD and metabolic syndrome
Metabolic syndrome and its individual components, including insulin resistance, are now recognized as independent risk factors for CKD development in diabetic as well as in nondiabetic patients.4 CKD independently increases insulin resistance, creating a vicious cycle that increases cardiovascular risk.5 Altered glucose metabolism and reduced tissue sensitivity to insulin have been reported for more than two decades in both early-stage and advanced CKD.5 Although the exact mechanism for insulin resistance in CKD remains unclear, a postreceptor defect in the insulin-receptor signaling pathway in skeletal muscle is the likely primary abnormality.5 A variety of factors, including but not limited to inflammation, oxidative stress, anemia, metabolic acidosis, and vitamin D deficiency, are described as contributing to insulin resistance. Of these, vitamin D requires particular attention because of the kidney’s intricate role in vitamin D metabolism, the high prevalence of vitamin D deficiency in CKD, the availability of safe vitamin D analogs, and the pleiotropy of vitamin D that may cover multiple factors contributing to insulin resistance in CKD, such as inflammation and oxidative stress.6
Figure 1 summarizes alterations in glucose metabolism in CKD and potential roles for vitamin D compounds.
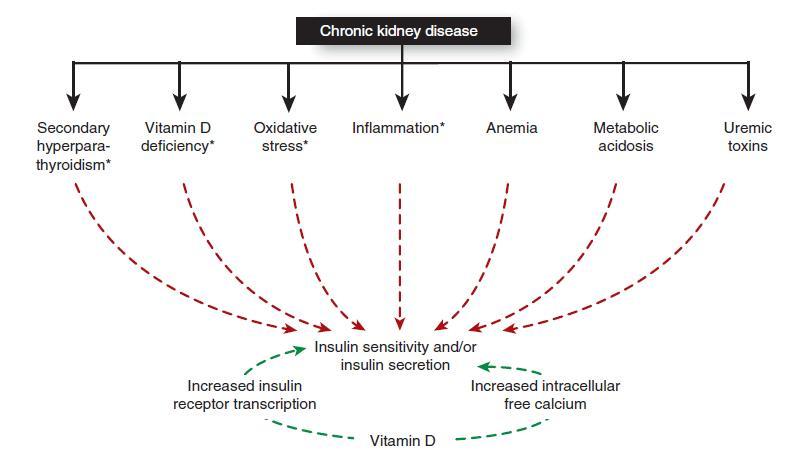
Alteration of glucose metabolism in chronic kidney disease and potential role of vitamin D compounds. Red arrows indicate deleterious effects, and green arrows indicate potential beneficial effects. In addition, vitamin D may affect glucose metabolism in chronic kidney disease through its effects on pathways marked with an asterisk.
Building the evidence pyramid
Vitamin D has long been implicated as having actions that mediate insulin secretion as well as insulin resistance. Early observations notable for worsening glucose control during the winter and spring in healthy and diabetic subjects were indicative of a possible role for vitamin D signaling in glucose metabolism.7 A number of cross-sectional studies reported an inverse association between vitamin D status and hyperglycemia.7 Vitamin D receptor is expressed in pancreatic β-cells, and calcitriol has been shown to improve islet-cell morphology in experimental animals.7 These investigations combined with the observational data set the stage for RCTs in this field. However, it is noteworthy that intervention trials on vitamin D supplementation using cholecalciferol or ergocalciferol have been largely inadequate to demonstrate any significant effect on glucose metabolism in the general population, whereas a number of small RCTs in hemodialysis patients using calcitriol report significant improvements in glucose metabolism.8, 9 These conflicting findings could result from different vitamin D formulations as well as differences in study populations. So if vitamin D administration optimizes glucose metabolism in hemodialysis patients,8, 9 then what will be its effects on glycemic parameters in CKD? Only a well-designed and adequately powered RCT can appropriately address this question. The study by de Boer et al. makes this attempt and contributes valuable information on this topic.3
Their trial addressed the effects of paricalcitol administration on glucose metabolism in nondiabetic subjects with stages 3–4 CKD.3 They followed a crossover design and enrolled 22 CKD subjects with baseline glucose intolerance. The study intervention, 2 μg oral paricalcitol daily for 8 weeks , was compared with a matching placebo with participants and investigators blinded to the randomly assigned sequence of intervention versus placebo. In the intent-to-treat analyses, changes in glucose tolerance assessed by an oral glucose tolerance test were not different between paricalcitol and placebo. Paricalcitol had no effect on measures of insulin sensitivity, insulin secretion, insulin action at adipose tissue, and oxidative stress.
The study was well powered for the primary outcome and was rigorously conducted, maximizing the ability to make accurate inferences about the true state of nature in the study setting (internal validity). However, a number of issues remain regarding the applicability of the findings to CKD patients and interventions in general (external validity). First, patients with overt diabetes, who comprise a significant proportion of CKD patients, were excluded, and as the authors acknowledge, results may be different in these patients. Second, it is possible that there are biological differences between the effects of paricalcitol and calcitriol on glucose metabolism, leaving the door open to study other active vitamin D analogs. Notable differences may exist in vitamin D repletion when cholecalciferol (D3 compound) is compared with ergocalciferol (D2 compound), with cholecalciferol being more potent. Among active agents, paricalcitol (D2 compound) has less affinity for vitamin D receptor and also for vitamin D-binding protein.10 Can the structural differences between paricalcitol and calcitriol—namely, the absence of a carbon 19-methylene group, the presence of a double bond between carbon 22 and 23, and the presence of an extra methyl group—contribute to differences in their effects on insulin mechanisms and secretion? Third, the majority of the patients were Caucasian and had relatively adequate vitamin D status as measured by 25-hydroxyvitamin D levels. Paricalcitol’s actions on glucose metabolism in the setting of vitamin D insufficiency or deficiency and in other populations including blacks and Hispanics remain unclear and should be taken into consideration in the planning of future studies. Nevertheless, even null findings of this study that glucose intolerance is not improved by paricalcitol administration in CKD patients provide essential information for the subject of glucose metabolism in CKD.
Lessons learned
A number of lessons are to be derived from the vitamin D RCTs in CKD patients. In addition to factors that address the internal validity of any RCT, such as sample size, intervention adherence, subject retention, and adequate follow-up length, future investigations should pay particular attention to hard clinical outcomes such as mortality or hospitalizations. This is easier said than done, but insisting on such hard outcomes will be an important step in moving the field forward. Intermediate outcomes provide valuable mechanistic insights and make trials efficient; however, their selection in future research needs to be very carefully thought through, especially as they may not be indicative of actual events, as was uncovered in the recently published PRIMO (Paricalcitol Capsule Benefits in Renal Failure-Induced Cardiac Morbidity) trial.11 Given the prevalent use of vitamin D analogs in advanced CKD patients primarily to address secondary hyperparathyroidism, it may also be worthwhile to pursue a pragmatic approach and undertake effectiveness trials rather than efficacy trials, where the emphasis would be on comparative effectiveness with the potential to compare different vitamin D compounds in a diverse population. Large simple trials are more likely to bring us closer to the truth than small complex trials,12 and future efforts in CKD should be directed toward them. Rigorously conducted efficacy studies, such as the one by de Boer et al.,3 with adequate power for a well-conceived objective intermediate outcome are to be encouraged in order to keep reducing critical knowledge gaps in the CKD field and to supply important information regarding study design and method to be applied in larger trials.
DISCLOSURE
Ravi I. Thadhani has received a research grant from Abbott Laboratories and is a consultant to Fresenius Medical Care North America.
Sagar U. Nigwekar declared no competing interests.
REFERENCES
Levey AS, Atkins R, Coresh J et al. Chronic kidney disease as a global public health problem: approaches and initiatives—a position statement from Kidney Disease Improving Global Outcomes. Kidney Int 2007; 72: 247–259. | Article | PubMed | ISI | CAS |
Samuels JA, Molony DA. Randomized controlled trials in nephrology: state of the evidence and critiquing the evidence. Adv Chronic Kidney Dis 2012; 19: 40–46. | Article | PubMed |
de Boer IH, Sachs M, Hoofnagle AN et al. Paricalcitol does not improve glucose metabolism in patients with stage 3–4 chronic kidney disease. Kidney Int 2013; 83 (this issue).
Thomas G, Sehgal AR, Kashyap SR et al. Metabolic syndrome and kidney disease: a systematic review and meta-analysis. Clin J Am Soc Nephrol 2011; 6: 2364–2373. | Article | PubMed |
Siew ED, Ikizler TA. Insulin resistance and protein energy metabolism in patients with advanced chronic kidney disease. Semin Dial 2010; 23: 378–382. | Article | PubMed |
Melamed ML, Thadhani RI. Vitamin D therapy in chronic kidney disease and end stage renal disease. Clin J Am Soc Nephrol 2012; 7: 358–365. | Article | PubMed |
Wolden-Kirk H, Overbergh L, Christesen HT et al. Vitamin D and diabetes: its importance for beta cell and immune function. Mol Cell Endocrinol 2011; 347: 106–120. | Article | PubMed |
Kautzky-Willer A, Pacini G, Barnas U et al. Intravenous calcitriol normalizes insulin sensitivity in uremic patients. Kidney Int 1995; 47: 200–206. | Article | PubMed | CAS |
Mak RH. 1,25-Dihydroxyvitamin D3 corrects insulin and lipid abnormalities in uremia. Kidney Int 1998; 53: 1353–1357. | Article | PubMed | CAS |
Slatopolsky E, Finch J, Ritter C et al. A new analog of calcitriol, 19-nor-1,25-(OH)2D2, suppresses parathyroid hormone secretion in uremic rats in the absence of hypercalcemia. Am J Kidney Dis 1995; 26: 852–860. | Article | PubMed | ISI | CAS |
Thadhani R, Appelbaum E, Pritchett Y et al. Vitamin D therapy and cardiac structure and function in patients with chronic kidney disease: the PRIMO randomized controlled trial. JAMA 2012; 307: 674–684. | Article | PubMed | CAS |
Peto R, Collins R, Gray R. Large-scale randomized evidence: large, simple trials and overviews of trials. J Clin Epidemiol 1995; 48: 23–40. | Article | PubMed | ISI | CAS |
PDF is attached at the bottom of this page