Vitamin D in Cancer Patients: Above All, Do No Harm – 2009
Journal of Clinical Oncology May 1, 2009 vol. 27 no. 13 2117-2119
Pamela J. Goodwin
Samuel Lunenfeld Research Institute, Mount Sinai Hospital and Princess Margaret Hospital, University of Toronto, Toronto, Ontario, Canada
In this issue of Journal of Clinical Oncology, Crew et al 1 report results of an examination of vitamin D in 103 premenopausal breast cancer patients who participated in a 1-year trial of zoledronate compared with placebo, in which all women received daily vitamin D (400 IU) and calcium (1,000 mg). Seventy-four percent of women were vitamin D deficient at study entry shortly after diagnosis; deficiency was more common in black and Hispanic women than in white women. After 1 year, less than 15% of the white women (but no Hispanic or black women) who had been vitamin D deficient at baseline achieved sufficient levels in their blood. The authors conclude, “…our study suggests that a dose of 400 IU daily is inadequate in breast cancer patients even to maintain skeletal health, and is probably too low for meaningful anticancer effects.” They go on to comment that controversy exists as to the upper safe daily limit of vitamin D supplementation and suggest “…it may be prudent to follow serum levels of 25-OHD [25-hydroxyvitamin D]…” This carefully conducted study echoes results recently reported by Neuhouser et al 2 (that approximately three fourths of patients with breast cancer from Los Angeles had inadequate blood levels of vitamin D) and by our group3 (that the same proportion of patients with breast cancer in Toronto had inadequate levels).
A search on PubMed using the terms “vitamin D,” “vitamin D and cancer,” or “vitamin D and breast cancer” from 1990 to November 2008 yielded the results shown in Table 1. The total number of articles relating to vitamin D published annually during that period has more than doubled, the number relating to cancer and vitamin D has almost tripled, and the number relating to breast cancer and vitamin D has increased almost six-fold. It is likely this increase reflects both a desire to generate evidence on effects of vitamin D that are now recognized to extend beyond bone health and calcium metabolism (including effects on neuromuscular and cardiovascular health, autoimmunity, infection, and cancer)4 and a belief, not fully supported by evidence, that vitamin D deficiency is a cause of ill health in the general population that should be treated with increasingly high doses of vitamin D.5 A recent meta-analysis 6 of nine studies of vitamin D supplementation showing that vitamin D supplementation in doses that ranged from 300 to 2,000 IU/d (mean, 528 IU/d) was associated with a modest but significant reduction in mortality (relative risk, 0.93; 95% CI, 0.87 to 0.99) provides some support for this belief; however, evidence for other health effects is weaker, and the authors recommended further study.
Table 1.
PubMed Search Results: Vitamin D (1990 to 2008)
When one looks at the association of vitamin D with cancer, the evidence is intriguing.5,7,8 For breast cancer,9 the strongest evidence is obtained from ecological studies that concluded that higher cancer rates in northern (v southern) latitudes were due to vitamin D deficiency. Observational studies examining the association between vitamin D intake or blood levels in relation to cancer risk in general, and breast cancer risk in particular, have yielded inconsistent results.6–8 Evidence of an adverse effect of vitamin D deficiency in colorectal cancer has been most consistent.10,11 Randomized trials, designed primarily for bone end points, have also yielded inconsistent results. Lappe et al 12 reported a reduction of overall cancer risk (a secondary end point) in postmenopausal women randomly assigned to receive calcium alone or calcium plus vitamin D (1,100 IU/d) versus placebo; there was no vitamin D–only arm and cancer risk did not differ between the two calcium-containing arms. In contrast, a recent report from the Women's Health Initiative13 failed to identify a beneficial effect of vitamin D supplementation (at a lower dose of 400 IU/d) on breast cancer risk compared with placebo. A note of caution is injected by reports that higher blood levels of vitamin D (well below the range considered toxic) may be associated with increased esophageal and prostate cancer risk or with more aggressive prostate cancer.14,15 Taken together, the available information is inadequate to conclude whether vitamin D influences cancer risk or mortality; furthermore, in individual studies in which vitamin D has been associated with cancer, it is not clear whether it is vitamin D or the company that it keeps (eg, diet, outdoor activity, healthy weight, higher socioeconomic class) that is the potentially responsible agent. The issue of causality is of particular concern given previous failed attempts to confirm the potential cancer-lowering effects of micronutrients such as ?-carotene in cancer in randomized trials, even though observational studies suggested important effects.16
Notwithstanding lack of high-level evidence, an effect of vitamin D on cancer risk or outcome is biologically plausible.17–20 Recent research has demonstrated that many tissues express 1,25-vitamin D hydroxylase, and are thus able to convert the predominant circulating form of vitamin D (inactive 25-OHD) to active 1,25-dihydroxyvitamin D. This 1,25-dihydroxyvitamin D can bind to vitamin D receptors, which are present on the nuclei of most cells. These vitamin D receptors are nuclear transcription factors that regulate the expression of more than 200 genes responsible for cell differentiation, proliferation, and apoptosis. The potential for major biologic effects underscores the critical importance of understanding the clinical impact of vitamin D on cancer risk and outcome, and should serve as stimulus for a targeted, adequately funded program of research in this area.
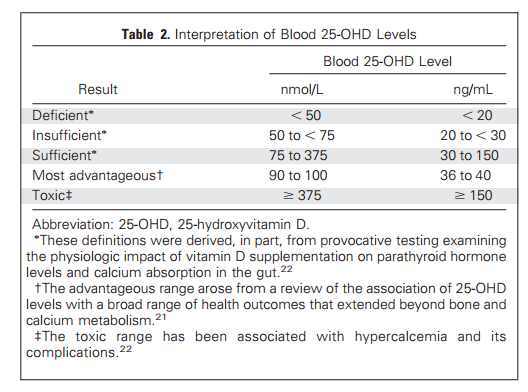
While awaiting results of this future research, as oncologists, we are being asked to advise our patients about whether they should take vitamin D supplements and, if so, what dose they should take. The unpredictable relationship between vitamin D intake and blood levels13,21 (likely reflecting individual variability in diet, absorption, metabolism, and adiposity, and in sun exposure as an alternate source of vitamin D) makes it difficult to recommend a standard supplement dose and supports incorporating measurement of blood levels into recommendations. Although there is some minor disagreement about specific cut points,4,21–24 most authorities suggest that a blood level of 25-OHD (the best marker of vitamin D status) of approximately 75 nmol/L (30 ng/mL) is required for vitamin D sufficiency, and levels above 375 nmol/L (150 ng/mL) are potentially toxic (associated with increased risk of hypercalcemia 4; Table 2). One recent review 21 suggests that there may be a “most advantageous” range of 25-OHD that starts at 75 nmol/L (30 ng/mL) and is ideally 90 to 100 nmol/L (36 to 40 ng/mL) that is associated with optimal musculoskeletal, neuromuscular, and cardiovascular health and immune function. Evidence regarding the safety of higher blood levels of vitamin D or supplementation with large doses of vitamin D focuses almost exclusively on short-term (up to 6 months) effects on calcium metabolism. Hypervitaminosis D (25-OHD > 375 nmol/L or > 150 ng/mL) is associated with hypercalcemia and resulting complications, including renal stones and bone demineralization.22,24 Information regarding effects of high levels of vitamin D on cell proliferation, differentiation, and apoptosis (of great relevance to cancer) or on other non–calcium-related health outcomes is lacking and is urgently needed.
Table 2 Interpretation of Blood 25-OHD Levels
With this background, what can we recommend to our patients? Current recommendations in the United States are 200, 400, and 600 IU per day of vitamin D3 (available in over-the-counter preparations) in individuals age younger than 50, 50 to 70, and older than 70 years, respectively; an equal dose of vitamin D2 (available by prescription) is approximately 30% as effective in maintaining vitamin D blood levels.24 There is sufficient evidence that vitamin D supplementation at these doses is associated with reduced mortality 6 and improved bone health that we should feel comfortable with these doses as a starting point. However, as Crew et al 1 point out, many of our cancer patients will be vitamin D deficient with this approach, and higher supplement doses will often be warranted, particularly in those whose therapy (eg, breast cancer patients receiving aromatase inhibitors) puts them at increased risk for adverse effects of vitamin D deficiency. In considering higher doses, oncologists should aim to achieve the benefits of adequate vitamin D levels but they should also be guided by the principle primum non nocere (above all, do no harm) . Some oncologists may be comfortable endorsing a higher dose in all patients; a dose of 1,000 IU/d is often suggested.5 However, rather than endorsing an arbitrary higher dose, measurement of blood levels of 25-OHD is the most prudent approach to determine those who might benefit from vitamin D supplements, and to ensure that levels are in the advantageous range (90 to 100 nmol/L, or 36 to 40 ng/mL ) in patients who are taking them. This approach should maximize known benefits and avoid both known (hypercalcemia and its associated complications) and potential unknown (cancer-related) adverse effects.
This advice should be viewed as interim. There may be specific benefits and harms associated with vitamin D supplementation in cancer patients that are not present in the general population, despite the fact that these benefits and harms have not been conclusively demonstrated. As a result, oncologists making recommendations to individual patients should take a cautious approach. Although this advice may be controversial, these recommendations should have a high chance of benefit and they should not harm our patients. As results of ongoing and planned research become available, many unanswered questions will be resolved, and more definitive recommendations that can be embraced by oncologists will be forthcoming.
AUTHOR'S DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
The author(s) indicated no potential conflicts of interest.
REFERENCES {# added by VitaminDWiki}
Crew KD, Shane E, Cremers S, et al. (2009) High prevalence of vitamin D deficiency despite supplementation in premenopausal women with breast cancer undergoing adjuvant chemotherapy. J Clin Oncol 13:2151–2156.
Neuhouser ML, Sorensen B, Hollis BW, et al. (2008) Vitamin D insufficiency in a multiethnic cohort of breast cancer survivors. Am J Clin Nutr 88:133–139. Abstract/FREE Full Text
Goodwin PJ, Ennis M, Pritchard KI, et al. (2008) Vitamin D deficiency is common at breast cancer diagnosis and is associated with significantly higher risk of distant recurrence and death in a prospective cohort study of T1-3, N0-1, M0 breast cancer. J Clin Oncol 26(suppl):9s, abstr 511. CrossRef
Norman AW (2008) From vitamin D to hormone D: Fundamentals of the vitamin D endocrine system essential for good health. Am J Clin Nutr 88:491S–499S. Abstract/FREE Full Text
Beres S (2008) Vitamin D: Cancer prevention's sunny future? J Natl Cancer Inst 100:292–297. FREE Full Text
Autier P, Gandini S (2007) Vitamin D supplementation and total mortality: A meta-analysis of randomized controlled trials. Arch Intern Med 167:1730–1737. Abstract/FREE Full Text
Davis CD (2008) Vitamin D and cancer: Current dilemmas and future research needs. Am J Clin Nutr 88:565S–569S. Abstract/FREE Full Text
Giovannucci E, Liu Y, Rimm EB, et al. (2006) Prospective study of predictors of vitamin D status and cancer incidence and mortality in men. J Natl Cancer Inst 98:451–459. Abstract/FREE Full Text
Rohan T (2007) Epidemiological studies of vitamin D and breast cancer. Nutr Rev 65:S80–S83. CrossRefMedline
Freedman DM, Looker AC, Chang SC, et al. (2007) Prospective study of serum vitamin D and cancer mortality in the United States. J Natl Cancer Inst 99:1594–1602. Abstract/FREE Full Text
Wu K, Feskanich D, Fuchs CS, et al. (2007) A nested case control study of plasma 25-hydroxyvitamin D concentrations and risk of colorectal cancer. J Natl Cancer Inst 99:1120–1129. Abstract/FREE Full Text
Lappe JM, Travers-Gustafson D, Davies KM, et al. (2007) Vitamin D and calcium supplementation reduces cancer risk: Results of a randomized trial. Am J Clin Nutr 85:1586–1591. Abstract/FREE Full Text
Chlebowski RT, Johnson KC, Kooperberg C, et al. (2008) Calcium plus vitamin D supplementation and the risk of breast cancer. J Natl Cancer Inst 100:1581–1591. Abstract/FREE Full Text
Ahn J, Peters U, Albanes D, et al. (2008) Serum vitamin D concentration and prostate cancer risk: A nested case-control study. J Natl Cancer Inst 100:796–804. Abstract/FREE Full Text
Chen W, Dawsey SM, Qiao YL, et al. (2007) Prospective study of serum 25(OH)-vitamin D concentration and risk of oesophageal and gastric cancers. Br J Cancer 97:123–128. CrossRefMedline
Greenwald P, Anderson D, Nelson SA, et al. (2007) Clinical trials of vitamin and mineral supplements for cancer prevention. Am J Clin Nutr 85:314S–317S. Abstract/FREE Full Text
Townsend K, Banwell CM, Guy M, et al. (2005) Autocrine metabolism of vitamin D in normal and malignant breast tissue. Clin Cancer Res 11:3579–3586. Abstract/FREE Full Text
Townsend K, Evans KN, Campbell MJ, et al. (2005) Biological actions of extra-renal 25-hydroxyvitamin D-1alpha-hydroxylase and implications for chemoprevention and treatment. J Steroid Biochem Mol Biol 97:103–109. CrossRefMedline
Chen WY, Bertone-Johnson ER, Hunter DJ, et al. (2005) Associations between polymorphisms in the vitamin D receptor and breast cancer risk. Cancer Epidemiol Biomarkers Prev 14:2335–2339. Abstract/FREE Full Text
Carlberg C (2003) Current understanding of the function of the nuclear vitamin D receptor in response to its natural and synthetic ligands. Recent Results Cancer Res 164:29–42. Medline
Bischoff-Ferrari HA, Giovannucci E, Willett WC, et al. (2006) Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am J Clin Nutr 84:18–28. Abstract/FREE Full Text
Holick MF (2009) Vitamin D Status: Measurement, interpretation, and clinical application. Ann Epidemiol 19:73–78. CrossRefMedline
Heaney RP (2005) The Vitamin D requirement in health and disease. J Steroid Biochem Mol Biol 97:13–19. CrossRefMedline
Holick MF (2007) Vitamin D deficiency. N Engl J Med 357:266–281. CrossRefMedline
PDF is attached at the bottom of this page