100,000 IU single dose of vitamin D - 2010
Pharmacokinetics of a single, large dose of cholecalciferol
Marium Ilahi, Laura AG Armas, and Robert P Heaney
.Am J Clin Nutr 2008;87:688-91. Printed in USA. © 2008 American Society for Nutrition
📄 Download the PDF from VitaminDWiki
Background: There is much interest in dosing vitamin D intermittently for patient convenience and long-term adherence.
Objective: The objective was to characterize the time course and response of 25-hydroxyvitamin D (calcidiol) to a large oral dose of cholecalciferol.
Design: One group (30 subjects) was supplemented with a single oral dose of 100 000 IU cholecalciferol. A second group (10 subjects) served as a control group to assess the seasonal change of calcidiol. Serum calcidiol concentrations were followed for 4 mo. The subjects were healthy with limited sun exposure (< 10 h/wk) and milk consumption (<0.47 L daily). We excluded subjects with granulomatous conditions, liver disease, kidney disease, or diabetes and subjects taking anticonvulsants, barbiturates, or steroids.
Results: Serum calcidiol rose promptly after cholecalciferol dosing from a mean (± SD) baseline of 27.1 ± 7.7 ng/mL to a concentration maximum of 42.0 ± 9.1 ng/mL. Seven percent of the supplemented cohort failed to achieve 32.1 ng/mL at any time point. The highest achieved concentration in any subject was 64.2 ng/mL. The control group had a nonsignificant change from baseline of —0.72 ± 0.80 ng/mL during 4 mo.
Conclusions: Cholecalciferol (100 000 IU) is a safe, effective, and simple way to increase calcidiol concentrations. The dosing interval should be <2 mo to ensure continuous serum calcidiol concentrations above baseline. This trial was registered at www.clinicaltrials. gov as .
INTRODUCTION
Vitamin D deficiency is a common problem (1, 2). Most vitamin D is obtained from the skin's exposure to sunlight, with a limited amount from the diet (3). Supplements are used to improve vitamin D concentrations, but there are few data on what doses to give and how often to give them. Serum calcidiol, the functional indicator for vitamin D status, has a long half-life, so there is much interest in intermittent dosing for patient convenience and long-term adherence. Although single, large oral doses were studied, no one has determined the optimum dosing frequency. A small amount of data from prior studies have shown that a single large dose of vitamin D raises calcidiol concentrations (4-9). The doses used in those studies ranged from 50 000 to 240 000 IU, and calcidiol concentrations were measured at intervals of 10 d to 6 mo after dosing. Data show that those doses of vitamin D are clinically useful. Khaw et al (10) showed a decrease in parathyroid hormone after a single dose of 100 000
IU cholecalciferol (vitamin D3) in an elderly population, and Trivedi et al (11) showed a decrease in fractures with dosing of 100 000 IU cholecalciferol every 4 mo. However, no studies have measured the time course of serum calcidiol concentrations after a large oral dose of cholecalciferol. Thus, although a single large dose will clearly elevate serum calcidiol, the degree of elevation and its duration are unknown. It is also not known whether the response [ie, area under the curve (AUC)] is linearly related to dose. In our previous study, comparing the time course of ergocalciferol with cholecalciferol, we had noted that after a single dose of50 000 IU cholecalciferol, calcidiol concentrations were still elevated 28 d after the dose (12). The current study was designed to assess the time course and response of serum calcidiol with a single oral dose of 100 000 IU cholecalciferol.
SUBJECTS AND METHODS
Setting and participants
The subjects were 40 healthy, community-dwelling, predominantly white men and women divided into 3 groups. (The subjects did include 1 African American and 1 Pacific Islander.) A group of 20 older subjects (aged 61- 84 y; 15 women, 5 men) and a group of 10 younger subjects (aged 27-47 y; 6 women, 4 men) were given a single large dose of cholecalciferol. A group of 10 subjects (aged 63-91 y; 9 women, 1 man) served as a concurrent untreated control group to assess the seasonal change of calcidiol. The subjects had limited sun exposure of <10 h/wk and daily milk consumption of <0.47 L (16 oz). We excluded subjects with reported granulomatous conditions, liver disease, kidney disease, or diabetes and subjects taking anticonvulsants, barbiturates, or steroids in any form. Twenty-six of the 40 subjects were taking calcium or multivitamin supplements that they continued to take throughout the study. Two control subjects did not complete the study because of travel to a sunny climate during the study months. All subjects were from Omaha, NE, and surrounding communities. Pertinent personal characteristics are set forth in Table 1. The project was approved by the Institutional Review Board of Creighton University, and all subjects gave written informed consent.
.TABLE 1
Demographic and intake data'
.!!Design overview
Enrollment for this open-label study was conducted in October. Subjects in the older age group were randomly assigned sequentially, using previously generated random numbers, to groups receiving either 2 capsules each labeled to contain 50 000 IU (1.25 mg) cholecalciferol or no supplement (control group). All the subjects in the younger age group received 2 capsules each labeled to contain 50 000IU(1.25mg) cholecalciferol. [The vitamin D capsules were supplied by Tishcon Corp (Salisbury, MD). The product was assayed on August 29, 2006, and found to contain 56 220 IU cholecalciferol/capsule.]
At the initial visit, each subject's height and weight were measured. Height was measured 3 times with the use of a Harp-enden stadiometer (Seritex Inc, Carlstadt, NJ), and the average was used. Weight was measured 2 times with the use of a Health-O-Meter balance beam scale (Continental Scale Corp, Chicago, IL), and the average was used. The supplemented subjects had blood drawn on days 0, 1, 3, 5, 7, 14, 21, 28, 42, 56, 70, 84, 96, and 112 for serum calcidiol concentrations. Blood for serum calcium was drawn on days 0,1, 3,5, and 112. Intact parathyroid hormone was drawn on days 0 and 112. After the baseline blood was obtained, the subjects were observed while they took the assigned vitamin D supplement dose. The control group had blood drawn for calcidiol, calcium, and parathyroid hormone on day 0 and 112. All subjects had blood drawn between 0800 and 1400, at approximately the same time at each visit.
Analytic methods
Serum calcidiol was measured by radioimmunoassay, with the use of the IDS kit (Nichols Institute, San Clemente, CA). The assay has an intraassay CV of 5.3-6.1% and an interassay CV of 7.3-8.2%. All calcidiol measurements for a given subject were assayed at the same time and with the same kit in the laboratory of the Creighton University Osteoporosis Research Clinic. Intact parathyroid hormone was measured by radioimmunoassay (Dia-sorin, Stillwater, MN) in the laboratory of the Creighton University Osteoporosis Research Clinic. Calcium was measured by Roche Cobas Integra autoanalyzer (F Hoffmann-La Roche Ltd, Basel, Switzerland) in the medical laboratory of Creighton University.
Statistical methods
We estimated the sample size for our study from a previous study of calcidiol concentrations in a population of young, healthy subjects (12). Thirty subjects allowed us to measure a change in calcidiol of 4 ng/mL from baseline with a power of >90%anda P < 0.05.
AUC of serum calcidiol increments was calculated by the trapezoidal method individually for each subject, and the resulting AUC values were aggregated for descriptive statistics. AUC is the integrated blood concentration over time. The other standard pharmacokinetic markers [time to reach maximumconcen-tration (rmax) and concentration maximum (Cmax)] were also recorded individually for each participant, and these values were aggregated as well. MICROSOFT OFFICE EXCEL, version 2003 (Microsoft Corporation, Redmond, WA), orSPSS, Version 14 (SPSS Inc, Chicago, IL), was used for statistical calculations.
RESULTS
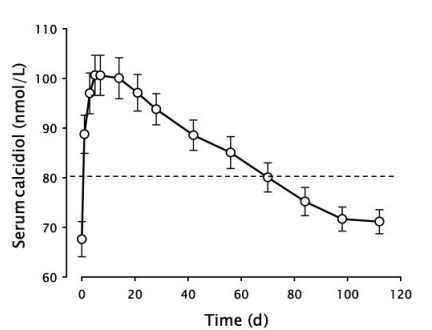
Serum calcidiol rose promptly after cholecalciferol dosing from a mean (±SD) baseline of 27.1 ± 7.7 ng/mL to a Cmax of 42.0 ± 9.1 ng/mL (Figure 1). The mean Cmax rise from baseline was 14.9 ± 5.1 ng/mL. The peak occurred at 7 d (median Tmax), and the serum concentration declined approximately linearly thereafter. Mean values no longer significantly different from baseline were reached by 84 d, and the mean calcidiol concentration also fell below 32.1 ng/mL by 84 d. Figure 2 expands the early portion of the time course and displays the dispersion around the mean values as ± 1 SD, thus giving a visual indication of the spread of the individual values. Two points stand out: 7)1 SD below the mean extends <32.1 ng/mL even at the Tmax (7% of our participants never reached 32.1 ng/mL) and 2) 1 SD above
.FIGURE 1. Time course of serum calcidiol for 112 d (16 wk) after asingle oral dose of 100 000 IU cholecalciferol (n = 30). The error bars are 1 SEM. The horizontal dashed line demarcates values above and below 80 nmol/L. To convert nmol/L to ng/mL, divide by 2.496.
.
FIGURE 2. Time course, as for Figure 1, except concentrating on the first 60 d after dosing (n = 30). In addition, the error bars here are 1 SD. To convert nmol/L to ng/mL, divide by 2.496.
the mean, even at Cmax, is barely >48.1 ng/mL. Thus, even a dose this large did not produce values remotely close to those associated with vitamin D intoxication, even in subjects who started with concentrations > 32.1 ng/mL.
The untreated controls had a mean change in serum calcidiol across the period of the study of —0.72 ± 0.80 ng/mL. Because this change was both small and not significantly different from zero, no attempt was made to adjust the values of the treated subjects.
A second feature of the data are the period of time for which subjects continued at serum calcidiol values above any arbitrary target concentration. As Figure 1 shows, the group taken as a whole was >32.1 ng/mL for «70 d. The group as a whole remained at >3 arbitrary cutoff values of 32.1, 36.1, and 40.1 ng/mL for 70,35, and 14 d, respectively. It should be stressed that these calculations are for the mean of the group and that some subjects never made it above certain of those cutoffs. (By the same token, some never fell below certain of them, either.)
When we separated the subjects by age, the younger subjects had a steeper rise, achieved a higher Cmax, and then had a more rapid rate of decline than did the older subjects. The AUC28 was 751.4 ± 218.4 nmol • d/L in the older group and 968.6 ± 451.6 nmol • d/L in the younger group. This difference was not statistically significant, and the AUC at 112 d was virtually identical.
Because of a suggestion that high initial concentration of serum cholecalciferol might displace calcitriol from the circulating D-binding protein and hence might induce hyperabsorption of calcium, we monitored serum calcium during the first 5 d after the cholecalciferol dose, a time when serum cholecalciferol concentrations would be highest. Serum calcium did not rise at any time point in either age group; in fact, a biologically small but statistically significant fall (—0.30 ± 0.38 mg/dL) occurred in serum calcium by 5 d after dosing. No subject experienced hypercalcemia at any of the measured time points.
Parathyroid hormone values for the supplemented group were
22.1 ± 7.41 pg/mL at baseline and 23.6 ± 9.22 pg/mL at the
conclusion of the study. Parathyroid hormone values for the control group were 29.0 ± 16.87 pg/mL at baseline and 31.4 ± 22.88 pg/mL at the conclusion of the study.
DISCUSSION
Trivedi et al (11) showed that dosing with 100 000 IU chole-calciferol every 4 mo reduced osteoporotic fractures, but those investigators supplied no information on optimal dosing frequency, because the time course of the response in their subjects was not measured. Similarly, Wigg et al (13) recently reported that 100 000 IU every 3 mo worked well to improve vitamin D nutrition in a residential care setting, but they, too, provide no data on time course and no information about how long the induced rise in serum calcidiol lasted. Thus, neither study, although using intermittent 100 000 IU doses, provides the information needed to devise an optimal dosing regimen. The present study is the first to do so. As shown in Figure 1, mean values had fallen below the desirable 32.1 ng/mL concentration by «70 d. Thus, clearly, a 121-d dosing schedule, as was used by Trivedi et al (11), does not provide continuous support of optimal calcidiol concentrations. Even the 90-d schedule used by Wigg et al (13) is probably suboptimal.
We saw that in several of our subjects even this large dose did not raise their calcidiol concentrations >32 ng/mL. Distinguishing features of these subjects were their low baseline calcidiol concentrations (between 15 and 18 ng/mL) and 1 subject was African American. We did not note any relation between baseline calcidiol concentrations and incremental response to treatment. A significant inverse correlation was observed of Cmax and body mass index (in kg/m2) (Spearman's R, 2-tailed significance. P < 0.01, with R2 = 0.466) but no correlation with baseline value (hence effectively eliminating regression to the mean as an important source of the observed variation).
We noted that the control subjects had little change in calcidiol during the 4 mo the study was conducted. Many were taking a multivitamin or calcium supplement that provided some vitamin D. This was consistent with previous work (3) that predicted a rise in calcidiol of 2 ng/mL with the small amounts of vitamin D those subjects were taking. It is important to note that these small amounts of vitamin D did maintain calcidiol concentrations throughout winter, but they did not increase the subjects' concentrations to optimal.
One of the questions raised at the outset was the linearity of the response. We addressed this issue by comparing the AUC developed for this dose to our previously reported study of a single dose of 50 000 IU cholecalciferol (12). Figure 3 makes that comparison graphically. Because the earlier study had data for only 28 d, AUC values for both studies had to be calculated for that time period. In addition, because the earlier study had enrolled only younger subjects and because the present study showed that the time course for the 2 age groups differed somewhat, it was necessary to use only the data from the younger subjects in the present study for this comparison. As is visually evident in the figure, the mean AUC for the present 100 000-IU dose is just about twice that for the 50 000-IU dose. Further, both doses, as referred to in this analysis, are for the labeled content. As noted earlier, the measured content of the preparation used in this study was «12% higher than labeled, and a similar departure occurred with the earlier study. When suitable correction is made for the actually ingested doses, the AUC values for the 2 differ by a factor of almost exactly 2-fold. Hence, one can reasonably infer that other doses will probably produce results that can be calculated from these 2 studies. Briefly, the 2 studies show that an o
.
FIGURE 3. Area under the curve (AUC) for the increment in serum calcidiol concentration above individual baseline values to 28 d (AUC28), for the younger persons in the present study (n = 10), contrasted with the corresponding AUC for the cholecalciferol supplemented group from the earlier study (n = 20) of Armas et al (12). Heights of the bars are the respective means of the individual incremental AUCs, and the error bar is 1
SEM.
AUC28 of «34.5 ng • d/L will be produced by each 10 000 IU cholecalciferol given as a single dose.
The reason for the possible difference in pattern for young and old subjects is uncertain. The higher body mass index in the older group could have had an effect or possibly the liver 25-hydroxylase reached its maximum capacity earlier (ie, at a lower precursor concentration) in the older subjects, thus blunting the induced rise in calcidiol. Some other explanation must be sought for the slower rate of decline in the older subjects. Obviously, metabolic consumption appears to be slower. By itself, this would have been predicted to lead not only to a slower clearance but to a higher initial concentration as well. So there is seemingly a need to invoke 2 differences in the handling of vitamin D between the younger and older ages. One possible unifying mechanism is a greater buildup of precursor cholecalciferol in body stores in the elderly after dosing, thus explaining both the lower initial rise and whether that buildup was then slowly released and converted to calcidiol during an extended time; then a single mechanism might account for both differences. However, because we have no data on serum cholecalciferol concentrations, we cannot distinguish between these possibilities.
We had subjects of both sexes, which is one possible limitation of this study, although there is no reason to believe a difference in calcidiol response would occur between sexes. Another limiting factor was the sample size. Although adequate for descriptive data, as was our original intent, it did limit our ability to confirm the apparent difference in responses between the different age groups. Further studies, with larger numbers of subjects, would be needed to determine whether this is a true difference.
Our study highlights that 100 000 IU cholecalciferol is a safe, efficient, and cost-effective means to increase calcidiol concentrations in the elderly. From this study we can safely recommend 100 000 IU cholecalciferol dosed every 2 mo in persons with moderate baseline calcidiol concentrations. However, in those persons with baseline calcidiol concentrations < 20 ng/mL, even this large dose will not adequately raise their calcidiol concentrations.
The author's responsibilities were as follows—MI: collected data and prepared the manuscript; LAGA: designed the study, collected and analyzed data, and prepared the manuscript; RH: designed the study, analyzed data, and prepared the manuscript. None of the authors had a personal or financial conflict of interest.
REFERENCES
Vieth R. Vitamin D supplementation, 25-hydroxyvitamin D concentrations, and safety. Am J Clin Nutr 1999;69:842-56.
Utiger RD. The need for more vitamin D. N Engl J Med 1998;338: 828-9.
Heaney RP, Davies KM, Chen TC, Holick MF, Barger Lux MJ. Human serum 25-hydroxycholecalciferol response to extended oral dosing with cholecalciferol. Am J Clin Nutr 2003;77:204-10.
Matsuoka LY, Wortsman J, Haddad JG, Hollis BW. Elevation of blood vitamin D2 levels does not impede the release of vitamin D3 from the skin. Metabolism 1992;41:1257-60.
Davies PD. A possible link between vitamin D deficiency and impaired host defence to mycobacterium tuberculosis. Tubercle 1985;66:301-6.
Whyte MP, Haddad JG Jr, Walters DD, Stamp TC. Vitamin D bioavail-
ability: serum 25-hydroxyvitamin D levels in man after oral, subcutaneous, intramuscular, and intravenous vitamin D administration. J Clin Endocrinol Metab 1979;48:906-11.
SternPH, TaylorAB, BellNH, EpsteinS. Demonstrationthatcirculating 1 alpha, 25-dihydroxyvitamin D is loosely regulated in normal children. J Clin Invest 1981;68:1374-7.
Scragg R, Holdaway I, Singh V, Metcalf P, Baker J, Dryson E. Serum 25-hydroxycholecalciferol concentration in newly detected hypertension. Am J Hypertens 1995;8:429-32.
Weisman Y, Schen RJ, Eisenberg Z, et al. Single oral high-dose vitamin D3 prophylaxis in the elderly. J Am Geriatr Soc 1986;34:515-8.
Khaw K, Scragg R, Murphy S. Single-dose cholecalciferol suppresses the winter increase in parathyroid hormone concentrations in healthy older men and women: a randomized trial. Am J Clin Nutr 1994;59:1040 -44.
Trivedi DP, Doll R, Khaw KT. Effect of four monthly oral vitamin D3 (cholecalciferol) supplementation on fractures and mortality in men and women living in the community: randomized double blind controlled trial. BMJ 2003;326:469-74.
Armas LA, Hollis BW, Heaney RP. Vitamin D2 is much less effective than vitamin D3 in humans. J Clin Endocrinol Metab 2004;89:5387-91.
Wigg AER, Prest C, Slobodian P, Need AG, Cleland LG. A system for improving vitamin D nutrition in residential care. Med J Aust 2006;185: 195-8.