Vitamin D and pregnancy, preterm birth, preeclampsia - Whittle
Proper vitamin D3 supplementation: Pregnant women and their future children first!
Two or more lives hang in the balance. Be sure to avoid paracetamol / acetominophen.
Robin Whittle Nov 24, 2024
Click here to see the orginal Substack with excellent charts]
Here is further research on the need for proper vitamin D3 supplementation to attain at least the 50 ng/mL (125 nmol/L) circulating 25-hydroxyvitamin D (as measured in “vitamin D” blood tests) which the immune system needs to function properly.
This is true of all people - except perhaps those who get so much ultraviolet B skin exposure, all year, every year, that their bodies produce sufficient vitamin D3 cholecalciferol for their livers to hydroxylate into sufficient 25-hydroxyvitamin D (AKA calcifediol or “calcidiol”) to maintain at least 50 nanograms (billionths of a gram) per millilitre (gram) all year round. Such people would arguably be healthier if they reduced their UV-B skin exposure - and so skin-damage and risk of cancer - and supplemented vitamin D3 sufficiently to maintain the level of circulating 25-hydroxyvitamin D they need to be healthy.
There’s nowhere near enough vitamin D3 in food, fortified or not, to provide the vitamin D3 we need to be healthy, so full health requires proper vitamin D3 supplementation, or significant long-term and surely harmful levels of UV-B skin exposure, and then somewhat less, or perhaps no, vitamin D3 supplementation.
My very long page https://vitamindstopscovid.info/00-evi/ cites and discusses dozens of research articles which I believe show, beyond any doubt, that 50 ng/mL should be the minimum level for all people, from birth into old age.
This begins vitamindstopscovid.info/00-evi/#00-how-much with recommendations from New Jersey based Professor of Medicine Sunil Wimalawansa (CV, University of Texas Medical Branch at Galveston, Robert Wood Johnson Medical School - now Rutgers University) on how much vitamin D3 to supplement to achieve this, without the need for blood tests or medical monitoring. The amount depends on body weight and obesity status, and is applicable to all people, of all ages and body weights who are not subject to medical advice to the contrary.
For 70 kg 154 lb body weight without obesity, 125 micrograms a day, on average, is a good amount. This is 1/8000th of a gram, also known by the rather large number of 5000 IUs, since an IU is 1/40,000,000 of a gram. This is a gram every 22 years.
This is 5 to 8 times more than what governments and many doctors recommend, since they are only seeking to attain about 20 ng/mL circulating 25-hydroxyvitamin D, which is sufficient for the kidneys to perform their part in regulating calcium-phosphate-bone metabolism. I will write an article suggesting particular vitamin D3 capsules which I think are a good choice, including some which also contain vitamin K2. K2 reducing the risk of excessive levels of calcium in the bloodstream as well as including strengthening immune responses and bone.
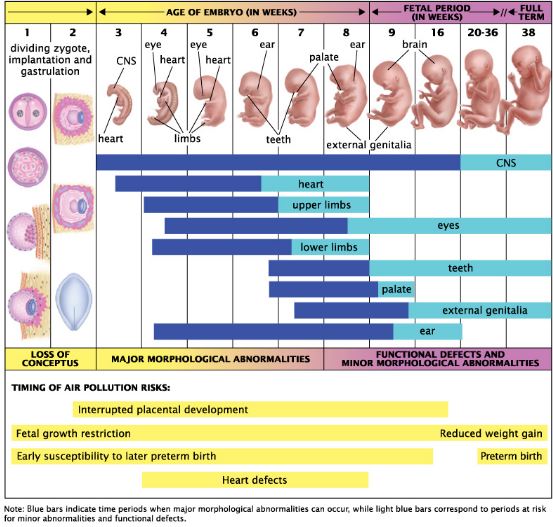
In-utero, the child-to-be’s brain is building itself
It is easy to see that in old age, vitamin D3 supplementation is badly needed to protect health generally, and especially to reduce the risk of dementia - though this takes decades to develop and the protection must start in mid-life. Yet most aged people do not supplement vitamin D3 at all.
See: Responsibility for vitamin D supplementation of elderly care home residents in England: falling through the gap between medicine and food Joseph and Carol Williams, BMJ Nutrition, Prevention & Health 2020-10-12: nutrition.bmj.com/content/early/2020/09/20/bmjnph-2020-000129.
My long page has a section vitamindstopscovid.info/00-evi/#3.3 on research which shows that low 25-hydroxyvitamin D greatly increases the risk of age-related neurodegeneration, including Alzheimer’s disease, and the three closely related movement disorders, which progress to dementia: Parkinson’s disease, multiple system atrophy and dementia with Lewy bodies.
Another section vitamindstopscovid.info/00-evi/#3.2 concerns low 25-hydroxyvitamin D in the mother, and so the fetus and newborn child, increasing the risks of preeclampsia, pre-term-birth, autism, ADHD, mental retardation and psychiatric symptoms in the child between ages 6 and 8.
These sections cover a small but pertinent subset of the research on these matters. Rather than expand them, I am writing Substack articles and linking to them from these sections.
I can’t think of any aspect of life, other than direct attack, more likely to motivate concerned individuals into action than contemplating the child-to-be - the adult, mother, father to be - building his or her own body, cell-by-cell, in Mother’s womb, and being prevented from doing so properly due to toxins, diseases or inadequate nutrition.
Neurons alter their growth patterns with exquisite sensitivity as they interact with other neurons and support cells, to attain shapes and make specific synapses which form the basis for all of the person’s life. Deficiencies in neurodevelopment in-utero and in early childhood can be devastating, as in schizophrenia, bipolar disorder and autism.
Low 25-hydroxyvitamin D is far from the only assault on these processes which increase the risk of autism. Fever, in the pregnant mother, the newborn or the child - including fever and other disturbances caused directly by vaccination - also raise the risk of autism. See the and the research cited at: popularrationalism.substack.com/p/three-years-later-after-ipak-alerted, petermcculloughmd.substack.com/p/febrile-seizures-after-childhood and kirschsubstack.com/p/over-300-pages-of-evidence-from-the. For a clear, tragic, case of 18 or so childhood catch-up vaccinations in one day putting a healthy 5 year-old into ICU, from which he emerged with profound autism, see the interview of David Ihben, with his children by his side: marcellapiperterry.substack.com/p/isaac-ihben-5-year-old-boy-force.
Another under-appreciated risk of autism and related life-long neurodevelopmental problems is the mother using paracetamol AKA acetaminophen during pregnancy. This is one of the most commonly used non-prescription drugs - including Tylenol and numerous other preparations in the USA and Panadol and the like in Australia. Supermarket shelves are loaded with this common analgesics which, when used to excess, as it often is by the suicidal, causes permanent liver damage often leading to death https://scholar.google.com.au/scholar?hl=en&as;_sdt=0%2C5&q;=paracetamol+toxicity.
Paracetamol/acetaminophen causes temporary emotional dulling and potentially excessive risk taking in adults when used as directed: https://academic.oup.com/scan/article/15/7/725/5897711.
Flooding the fetus’ brain with a drug which interferes with neuronal signaling, when it its billions of neurons are finding their way, determining how to differentiate, or which axons and dendrites to extend or withdraw, will reduce the brain’s ability to construct itself as needed for the rest of the person’s life. Although the precise details are not yet known, it is reasonable to assume that some of the cell-types which are involved in underdeveloped - guiding the growth and connections of neurons - rely on 25-hydroxyvitamin D —> calcitriol (1,25-dihydroxyvitamin D) intracrine and paracrine signaling. These systems work, respectively, within a single cell, and to nearby cells, typically of different types. See: https://vitamindstopscovid.info/02-intracrine/.
Over-the-counter drugs containing paracetamol/acetaminophen should carry clear warnings against use in pregnancy - and I think any use by children and adolescents. See: Avella Garcia et al. 2016 Acetaminophen use in pregnancy and neurodevelopment: attention function and autism spectrum symptoms academic.oup.com/ije/article/45/6/1987/2617189 and the consensus statement by Bauer et al., 2021, Paracetamol use during pregnancy — a call for precautionary action https://www.nature.com/articles/s41574-021-00553-7.
Below are three research items of interest regarding the risks in pregnancy posed by low levels of circulating 25-hydroxyvitamin D:
Pre-term birth.
Pre-eclampsia
Pre-eclampsia increasing the risk mother’s risk, in mid-life, of young onset dementia.
I also suggest strategies to get women of childbearing age supplementing vitamin D3 properly.
Pre-term birth
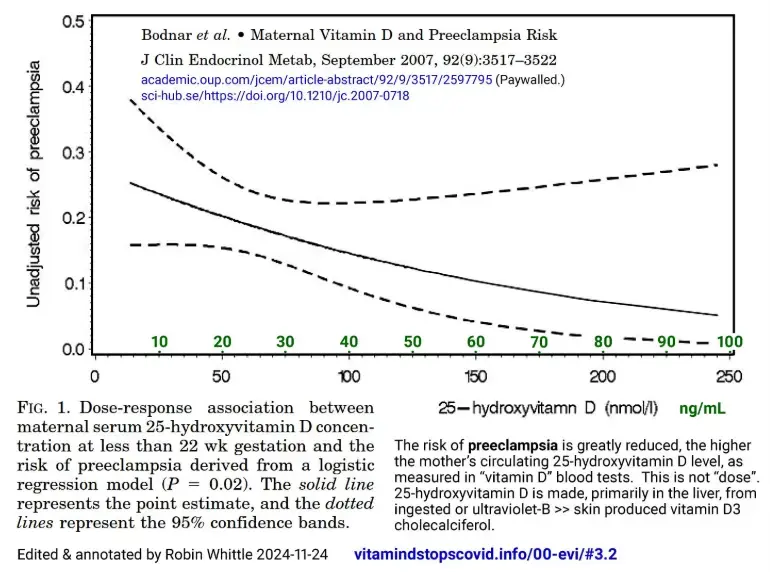
The graph at the start of this article is from:
Maternal Vitamin D Deficiency Increases the Risk of Preeclampsia
Lisa M. Bodnar, Janet M. Catov, Hyagriv N. Simhan, Michael F. Holick, Robert W. Powers and James M. Roberts
Journal of Clinical Endocrinology & Metabolism 92(9):3517–3522 2007-05-29
academic.oup.com/jcem/article-abstract/92/9/3517/2597795 (Paywalled.)
The PDF is available from at Alexandra Elbakyan's awesome, life-saving, science-powering, website Sci-Hub: https://sci-hub.se/10.1210/jc.2007-0718.
The researchers surveyed women with no pre-existing medical conditions, who gave birth for the first time, from “outpatient clinics at Magee-Womens Hospital in Pittsburgh, PA, and affiliated private practices from 1997–2001”.
The graph depicts the risk of preeclampsia declining monotonically (without any break or reversal in the trend) with increasing 25-hydroxyvitamin D levels. While there may be some confounding - such as inherently healthier women also happening to supplement more vitamin D3, and so have higher 25-hydroxyvitamin D levels - the trend is very strong.
The dotted lines represent upper and lower 95% confidence limits. The space between these encompasses the most likely range of possible true relationships between these two observations (preeclampsia or not and the mother’s 25-hydroxyvitamin D level, measured at 21 weeks gestation or earlier), which would actually exist, and so be found with greater certainty in a much larger survey, if there was a much larger population of such subjects than the number included in this survey. The uncertainty is inherent in the number of subjects sampled. The 95% limits indicate, that with a sample of this size, there is a 95% chance that the real position of the solid black curve for a much larger population lies within these boundaries. This is tortuous to explain in words alone. New Zealand math teacher Nicole Petty PhD has a most instructive video: www.youtube.com/watch?v=js09aLuFP4I.
I generally don’t fuss much about these confidence limits, but they are worth considering in this case. The decline in risk - as best we know from this data, the improvement in health outcomes - with 25-hydroxyvitamin D levels above 50 ng/mL is highly significant: a 12% risk of preeclampsia at 50 ng/mL seems to fall to 5% at 100 ng/mL.
If the solid black line truly represented the health improvement due solely to higher 25-hydroxyvitamin D levels, then, all over the world, we could improve outcomes, exactly this much, by ensuring hundreds of millions of women, for their entire pregnancies or probably their whole lives to date, had 100 ng/mL circulating 25-hydroxyvitamin D, rather than 50 ng/mL or any lower level.
I am highly confident (for what its worth - I have no medical training or experience) that the great majority of the risk reduction depicted here between the lowest levels of 25-hydroxvitamin D - 25% risk at 6 ng/ML - and 12% at 50 ng/mL is real. There’s no way multiple cell types, including many of the immune system, can respond to their changing circumstances properly when they are starved for 25-hydroxyvitamin D, which needs to be present in their cytosols (cell interior fluids) and rapidly replenished as it is used, when their 25-hydroxyvitamin D —> calcitriol intracrine and paracrine signaling systems are activated. These systems will work fine with 50 ng/mL but will at best only work to a limited extent with 6 ng/mL.
It is uncommon to see measurements of health benefits improving so strongly - a halving in risk of serious complications in this case - in the 50 ng/mL to 100 ng/mL range of 25-hydroxyvitamin levels. I believe that there often are improvements, but probably not as dramatically as this. (I am 67 kg, supplement about 0.2 mg 8000 IU a day vitamin D3 on average and my 25-hydroxyvitamin D level was close to 100 ng/mL on the one occasion in the last decade or so on which it was measured.)
The 95% error margins open up at the left and right of the graph, since there are fewer women in the sample with these values. I guess that quite a lot of this downward trend of the solid black risk line, to the right of 50 ng/mL, is due to the inherently healthiest women (through good fortune, economic security and healthy lifestyle choices born of education and good advice) having a higher probability for supplementing the larger amounts of vitamin D3 which bring their 25-hydroxyvitamin D levels closer to 100 ng/mL.
So I guess that some, perhaps, most, but probably not all, of the halving of risk we see in the graph between 50 and 100 ng/mL is due to confounding. The likely actual benefits from these higher levels are probably not so dramatic, and I would still think that 80 to 100 ng/mL is a better level than 50 to 60 ng/mL.
Pre-term birth
The next pair of graphs is from:
Maternal 25(OH)D concentrations 40 ng/mL associated with 60% lower preterm birth risk among general obstetrical patients at an urban medical center
Sharon L. McDonnell, Keith A. Baggerly, Carole A. Baggerly, Jennifer L. Aliano, Christine B. French, Leo L. Baggerly, Myla D. Ebeling, Charles S. Rittenberg, Christopher G. Goodier, Julio F. Mateus Niño, Rebecca J. Wineland, Roger B. Newman, Bruce W. Hollis and Carol L. Wagner
PLOS One 2017-07-24 doi.org/10.1371/journal.pone.0180483
(Full-res: 5nn.info/temp/2017-McDonnell.png)
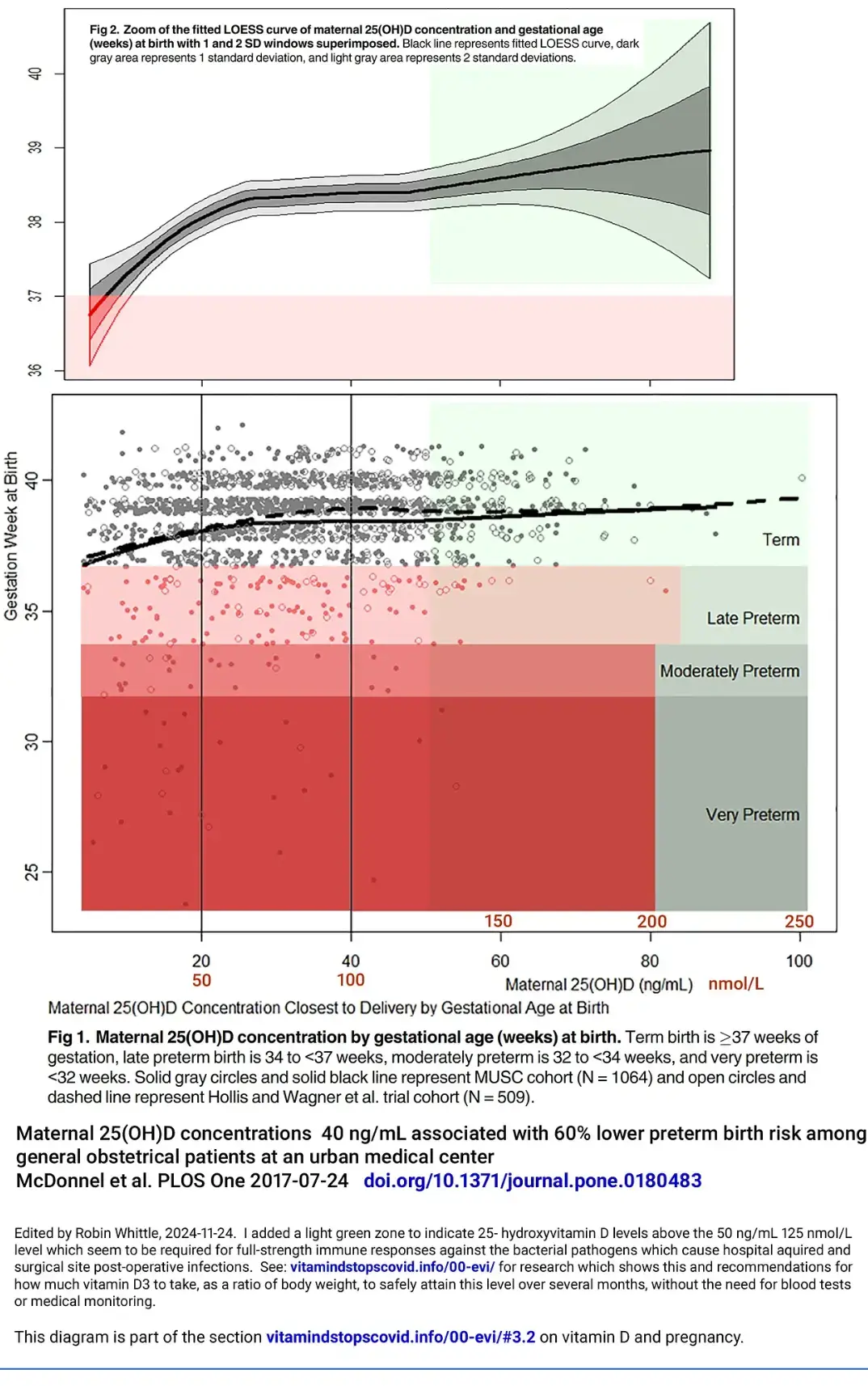
The subjects were women aged 18 to 45, who may have given birth before and who gave birth to a single child between September 2016 and October 2016 at the Medical University of South Carolina. Two of the authors, Professors Hollis and Wagner, are among the top dozen or so vitamin D researchers worldwide with awesome publication histories spanning decades of research.
The uptick in gestational length with 25-hydroxyvitamin D levels above 45 ng/mL, with its trombone horn of expanding statistical uncertainty, is a curiosity I discuss below.
The most important finding is that gestational age at birth declines precipitously the further the circulating 25-hydroxyvitamin D level is below 27 ng/mL (68 nmol/L = 1 part in 37,000,000 by mass).
While it is possible for women to give birth, after healthily long gestations (the upper left dot next to the “40”, with disastrously low 25-hydroxyvitamin D level), this rapid decline in the mean gestational length, with its narrow statistical uncertainty bars, shows that one or more bodily systems, in at least some women - surely more and more with the lower 25-hydroxyvitamin D levels - are failing seriously.
In electronic design, if some aspect of the system - especially a power supply voltage - was so frequently drifting towards the rocks like this, we would fix it by lunchtime.
In medicine, despite its numerous wonders (most of dentistry, a lot of acute medicine) next to nothing happens from decade to decade when simple nutritional inadequacies harm millions of people like this. (Don’t get me started on the reasons - it is a massive topic.)
From the article:
There were 15 million preterm births (PTB) (less than 37 weeks) worldwide and more than 1 million infant deaths from PTB complications in 2010. PTB rates ranged from 5% to 18% around the world and the rate in the United States was disproportionately high (12%) compared to other developed counties.
Substantial racial disparities in PTB rates have also been found in the United States: 18% among African Americans, 12% among Hispanics, and 11% among whites in 2009.
Since PTB is the leading cause of neonatal death and multiple short and long term health problems, it is critical to identify modifiable maternal risk factors that could significantly reduce PTB risk at the population level.
Results:
Among women with a live, singleton birth and at least one 25(OH)D test during pregnancy (N = 1,064), the overall PTB rate was 13%. The LOESS curve showed gestational age rising with increasing 25(OH)D.
Women with 25(OH)D greater than or equal to 40 ng/mL had a 62% lower risk of PTB compared to those with less than 20 ng/mL (p less than 0.0001).
The women with 40 ng/mL or more circulating 25-hydroxyvitamin D had 38% the overall rate of pre-term birth than those with 20 ng/mL or less.
“(p less than 0.0001)” means that, given the sampling error in this particular study, the probability of the real relationship between pre-term birth and 25-hydroxyvitamin D being none (the two not being related at all), indicating that the particular subset of pregnancies included in the study happened, by chance, to be skewed in a way which made it appear there was such a strong relationship, is less than one in 10,000. en.wikipedia.org/wiki/P-value. In other words, one would have to conduct over 10,000 trials of this nature, in a population of women in which there was genuinely no relationship between pre-term birth and 25-hydroxyvitamin D level, to, on average, for one of these trials to sample a particular subset of this much larger population of women, with this subset exhibiting as strong a relationship as was found in this study.
After adjusting for socioeconomic variables, this lower risk remained (OR = 0.41, p = 0.002).
After the researchers attempted to correct for confounding relationships they were able to identify, the lower risk of pre-term birth for women with 40 ng/mL or more circulating 25-hydroxyvitamin D with respect to those with 20 ng/mL was 41%, which is not much different from the unadjusted rate of 38%.
The researchers were unable to attribute much of the very strong relationship they observed to confounding. This means it is reasonable to assume that the strong variation in pre-term birth rates was caused by the women’s 25-hydroxyvitamin D levels.
Here I am going to be rather pedantic: The levels measured in this survey did not result from any supplementation intervention by the researchers. So, while pregnant women are encouraged to supplement vitamin D (albeit, often in quantities too small to attain 50 ng/mL after any amount of time, much less in a few months), the measured 25-hydroxyvitamin D levels would generally be strongly correlated with the levels the women had had for years before, perhaps for most or all of their lives.
So we are witnessing, in the stark results here, the impact not just of the 25-hydroxyvitamin D levels during pregnancy, but the longer term health impacts of the very low 25-hydroxyvitamin D levels of some women, from previous years or decades with their immune systems and other bodily systems running from only a small fraction of the 25-hydroxyvitamin D level they need to be healthy.
These researchers would probably tell you that 40 ng/mL or more circulating 25-hydroxyvitamin D is healthy and that less is not.
Governments and many doctors are happy with 20 ng/mL. (Some doctors aim for 30 ng/mL 75 nmol/L.) Yet we see the pre-term birth risk escalating the further the level falls below 27 ng/mL. Looking at the dots, I estimate that 40% of these women had levels of 27 ng/mL or less.
The authors do not comment on slight increase in gestational age with 25-hydroxyvitamin D levels above 45 ng/mL. Are these babes-about-to-be having such a fine time in the womb that they are in no hurry to progress to their next life stage? Are they busy composing their sonnets of the belly while they still have the full experience?
Is this just confounding: inherently healthier women being statistically more likely to supplement vitamin D3 properly, which is the most common way of attaining these levels? We can’t tell. The authors express no concern. There children’s brains will have built themselves in-utero with a perfectly good supply of 25-hydroxyvitamin D.
Preeclampsia and early-onset dementia
Young-onset (early onset) dementia is defined as that which occurs before the age of 65. Here we consider research which showed that women who had suffered preeclampsia in pregnancy have a very significantly greater risk of suffering early onset dementia. The articles and discussion are:
https://jamanetwork.com/journals/jamanetworkopen/article-abstract/2819207
Many studies have shown this disorder has consequences that last decades after pregnancy, with an increased risk of cardiovascular and kidney morbidity and mortality in individuals with a history of preeclampsia.
Recently, those with preeclampsia were described as having a 3-fold higher risk of late-onset vascular dementia after a mean follow-up of 20 years. This cohort study investigated whether preeclampsia and other hypertensive disorders of pregnancy (HDPs) were associated with an increased risk of young-onset dementia years after the pregnancy.
https://jamanetwork.com/journals/jamanetworkopen/article-abstract/2819208
For 2 centuries, clinicians have appreciated the worrisome consequences of high blood pressure and proteinuria [WP, protein in the urine, indicating kidney dysfunction] appearing during pregnancy. These symptoms herald the onset of preeclampsia, a major obstetric complication that not only causes serious morbidity but also threatens the lives of both the pregnant individual woman and the unborn child.
. . . data from the French Conception study, a nationwide prospective study in which 1,966,323 pregnancies were followed-up for a mean of 9 years. The team found that having had preeclampsia incurred a 2.65-fold increased risk of young-onset dementia compared with unaffected pregnancies. Furthermore, the hazard ratio increased to 4.15 (95% confidence interval, 1.30-13.14) if the preeclampsia occurred at a preterm gestation.
journals.lww.com/jhypertension/abstract/2024/05001/preeclampsiaandyoungonsetdementiatimeto.860.aspx
This highlights a need for close follow-up among women who have experienced pre-eclampsia, covering neurological health as well as the metabolic, cardiovascular and renal systems.
None of these peer-reviewed articles mention the word “vitamin”.
These researchers seem to be unaware that low 25-hydroxyvitamin D is a serious risk factor for both preeclampsia and dementia. This alone would explain the correlation between incidences of the two conditions, since women with low 25-hydroxyvitamin D in pregnancy are likely to also have lower levels in later decades.
We can reasonably assume that the correlation will remain strong with the much more prevalent mainstream forms of dementia, occurring at ages 65 and beyond.
There’s surely more to this tragic - individually and for all friends and family, disastrous - raised incidence of dementia.
I have avoided mentioning what actually goes wrong in preeclampsia, since I figure some people read Nutrition Matters while having breakfast. This will do: https://en.wikipedia.org/wiki/Pre-eclampsia. (Ideally I would fix this statement, which is surely false regarding vitamin D at least: “Supplementation with antioxidants such as vitamin C, D and E has no effect on pre-eclampsia incidence.” However, it can take hours wrangling with those who busy themselves ensuring that Wikipedia pages conform to mainstream dogma, with no guarantee of success.)
The vascular and general organ damage which occurs in preeclampsia could easily alter the brain’s delicate circulatory system, including reducing, forever, its ability to adequately supply oxygen. This would probably entail damage to the lymphatic and glymphatic [WP] systems, permanently curtailing their ability to remove waste, and so contributing to the risk of the inflammatory processes which drive dementia.
The impact on the surviving child is not mentioned. What lasting harm do they suffer, which might have most effect when they reach their 60s and beyond?
Women’s health and survival are threatened in many ways when they become pregnant, give birth and their bodies sacrificing their own minerals and other nutrients in breast feeding.
Its a scandal, disaster and horror that so many women and their children face elevated risks of these damaging or deadly conditions for lack of a few tens of milligrams of vitamin D3 a year.
Priorities for proper vitamin D3 supplementation
If we are to focus attention on particular sub-groups of society in the hope of them adopting (freely, in full knowledge, without manipulation, mandates or undue influence) the vitamin D3 supplementation they need to be healthy, who should this be?
The elderly, in care homes, are one such group. They are helpless and often devoid of hope and personal connection. They are already in the care of highly organised institutions, who could easily dole out the daily capsules which would greatly improve their lives. But then they would remain, happier than before, in the homes for years more, and more such homes would need to be built. So this will be hard to get past the committees and stakeholders who control these things, not least because the results would show how derelict these institutions have been in caring for these unfortunate souls.
Prisoners are another group - again all in the care of institutions which could easily provide the daily or weekly capsules. This would probably be easier to get approved, especially if it could be shown that the result was less conflict and illness, which I am sure would be the case.
However those most urgently in need of proper vitamin D3 supplementation are the babes to be, with their bodies and brains building themselves from simple beginnings, in the wombs of their moms-to-be.
Women may have advanced two or more months into pregnancy by they time they realise they are carrying a developing child, or perhaps two or more. Ordinary vitamin D3 supplementation takes months to build up the 25-hydroxyvitamin D level, so it is already too late if we target women who know they are pregnant.
The proper target group to prioritise is women of childbearing age. Birth control doesn’t matter, since it is unreliable and women change their mind.
Women, especially teenagers, who are convinced they can’t get pregnant . . . These are most likely to become pregnant since they won’t use birth control.
So I vote for prioritising women of childbearing age.
Pitch this in terms of actual pregnancy and the long-term outcome for their children, will only impress a small, wonderful, subset of such women who are not yet mothers.
Unfortunately, many young women of childbearing age have other priorities. Some will smoke because they think it helps them loose weight. Many of them are borderline bonkers - look at their plastic fingernails. Bless them! Its a phase.
We need research articles focusing on the benefits for the skin and hair of proper vitamin D3 supplementation. Anna Piotrowska et al. 2016: Vitamin D in the skin physiology and pathology https://bibliotekanauki.pl/articles/1038837.pdf is heading in the right direction:
Unfortunately, UVB, which is required for vitamin D production, is also known as the main cause of a skin cancer, including melanoma. Here, we are going to review benefits of vitamin D and its analogues in the maintenance of epidermal barrier and its potential use in the treatment of common skin diseases.
We need a bunch of research studies, with attractive, gutsy women and men to explain them on YouTube.
We need social media influencers and young women as annoying as this one. with 1.4M Likes: www.tiktok.com/@the444agency/video/7311839695346879776 (HOW TO COMMAND THE UNIVERSE TO GET WHAT YOU WANT), leaning into their cell-phone cameras, exhorting their viewers to avoid the worst of the UV rays AND to keep their skin, their hair - and their lively, fluid, brains - well nourished with at least fifty-nanograms-per-millilitre twenty-five-hydroxyvitamin D.
If they are supplementing vitamin D3 properly for a few months at least before they begin to bring their child into the world, everything will work out for the best.
Ideally, vitamin K2, omega 3 fatty acids, zinc, magnesium as well - but first and foremost, vitamin D3, according to body weight and obesity status:
https://vitamindstopscovid.info/00-evi/#00-how-much
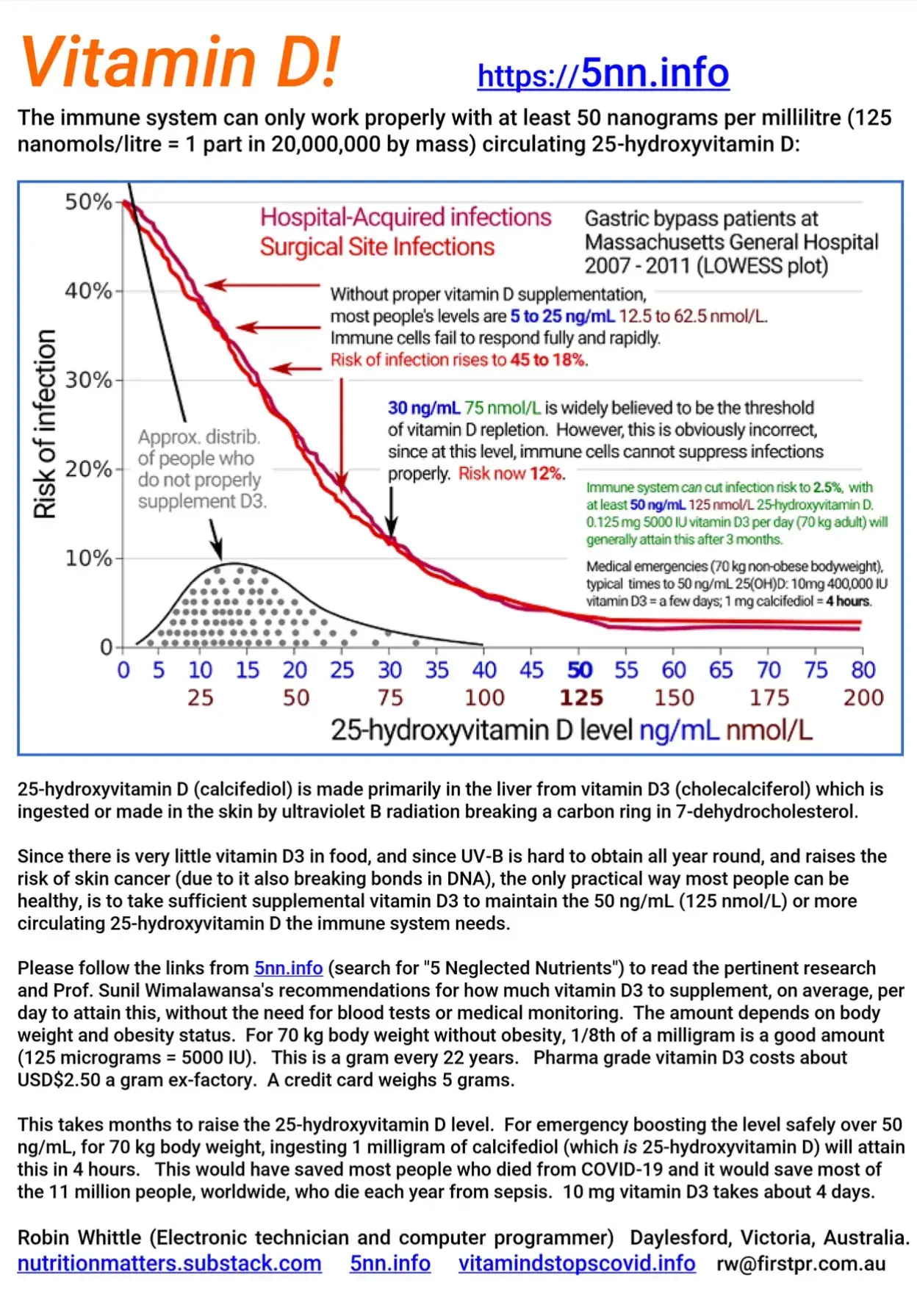
If you ever want to tell a friend about vitamin D supplementation and research, you can point them to, or look up on their cellphone:
5nn.info or search for 5 Neglected Nutrients.
This links to NutritionMatters.Substack.com, my vitamin D pages and carries some preliminary notes on other nutrients. It also has a printable PDF vitamin D flyer with the graphs showing 50 ng/mL or more pre-operative 25-hydroxyvitamin D squashing the risk of post-operative infections down to just 2.5%, from 25% at 18 ng/mL:
Pregnancy topics (and # of studies) in VitaminDWiki as of Oct 2024
Breastfed (38+)
Caesarean (15+)
Depression (21+)
Dark Skin (30+)
Gestational Diabetes (41+)
In Vitro Fert. (18+)
Iodine (21+)
Low Birth Weight (23+)
Magnesium (30+)
Miscarriage (31+)
Multiple Sclerosis (13+)
Omega-3 before and during (49+)
PCOS (15+)
Preeclampsia (55+)
Preterm (125+)
Preterm - Omega-3 (13+)
Stillbirth (8+)
Infant-Child topics (and # of studies) in VitaminDWiki as of Oct 2024
Infant/Child (850+)
Allergy (36+)
Cancer (13+)
Cerebral Palsy (15+)
Down Syndrome (5+)
Fracture, low energy (10+)
Growing Pains (10+)
Pneumonia (25+)
Preemie (25+)
Respiratory (21+)
RSV (25+)
Tonsils (9+)
Vaccination (10+)
Virus (42+)
Vitamin D is needed as soon as possible after conception
Details at Ensure a healthy pregnancy and baby - take Vitamin D before conception
VitaminDWiki - Pregnancy category contains
{include}
VitaminDWiki – Healthy pregnancies need lots of vitamin D contains
{include}