Maternal pregnancy problems if Vitamin D is less than 40 ng – meta-analysis
Vitamin D-Related Risk Factors for Maternal Morbidity and Mortality during Pregnancy: Systematic Review and Meta-Analysis
Nutrients 2022,14, 4124. https://doi.org/10.3390/nul4194124
María Morales-Suárez-Varela 1,2 , Nazli Uçar1, José Miguel Soriano 3, Agustín Llopis-Morales 1, Beth S. Sanford 4 and William B. Grant5,*
Area of Preventive Medicine and Public Health, Department of Preventive Medicine and Public Health, Food Sciences, Toxicology, and Legal Medicine, School of Pharmacy, University de Valencia, 46100 Burjassot, Spain
Biomedical Research Center Network on Epidemiology and Public Health (CIBERESP), Institute of Health Carlos III, 28029 Madrid, Spain
Food & Health Lab, Institute of Materials Science, University of Valencia, 46980 Paterna, Spain
College of Nursing, Rasmussen University, 4012 19th Ave S, Fargo, ND 58103, USA
Sunlight, Nutrition, and Health Research Center, PO. Box 641603, San Francisco, CA 94164, USA
* Correspondence: wbgrant@infionline.net
Vitamin D deficiency (serum 25-hydroxyvitamin D [25(OH)D] levels <20 ng/mL in serum) is a common health condition among pregnant women, especially in high-risk groups. Evidence has connected vitamin D levels with many health-related problems during pregnancy, including gestational diabetes and preeclampsia. Because of vitamin D's effect on both mother and fetus, we systematically review the association between 25(OH)D level and its health effects. From a total of 143 studies, 43 came from PubMed, 4 from Cochrane, and 96 from EMBASE. After screening, we identified 38 studies as candidates for inclusion. Ultimately, we limited this review to 23 articles originating from 12 countries, written in English or Spanish, and conducted between 2010 and 2022. We conducted this review according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines and evaluated the quality and strength of the evidence by using the Navigation Guide Systematic Review Methodology (SING). These systematic reviews summarize findings that support vitamin D's role in reducing risks of multiple outcomes and the possible contribution of adequate vitamin D levels to a healthy pregnancy.
📄 Download the PDF from VitaminDWiki
Discussion
The most common causes of maternal mortality are
severe bleeding,
infections/sepsis,
embolisms (blockage in the heart or lungs),
stroke (can be a blown blood vessel or an embolus),
blood pressure disorders (preeclampsia/eclampsia), and
gestational diabetes.
According to the WHO , the leading causes of maternal mortality (nearly 75%) are severe bleeding, postnatal infections, blood pressure disorders, and complications of labor and delivery [49]. In the US, the top causes of maternal mortality are hemorrhage, cardiovascular complications, infections/sepsis, embolism (pulmonary embolism or other embolisms), cerebrovascular accidents, and noncardiovascular medical conditions such as gestational diabetes mellitus (GDM) [51].
In this review, we aimed to evaluate the current evidence on the effect of vitamin D and vitamin D supplementation on maternal mortality and morbidity. Interventions yielded significant effects, albeit with sparse evidence in some areas.
In recent years, scientific interest has increasingly focused on the consequences of VDD on pregnant women, in particular, the impact of its deficiency on adverse maternal health outcomes. With all significant effects taken together, vitamin D supplementation was associated with a reduced risk of maternal mortality and morbidity-related outcomes.
Many observational studies did report that vitamin D levels were associated with adverse maternal, fetal, and neonatal outcomes, including increased risk of developing preeclampsia, preterm labor, gestational diabetes, being small for gestational age, low birth weight, an increased rate of Cesarean delivery, and infertility [50]. Since vitamin D RCTs have not yielded much useful information regarding the role and requirements for vitamin D for many health outcomes while observational studies have [52], results from observational studies are highlighted in the following paragraphs.
Hemorrhage
Low maternal 25(OH)D concentrations have been found to be associated with an increased risk of postpartum hemorrhage. An observational study from Taiwan involving 600 pregnant women with 25(OH)D concentrations measured in the 36th week of pregnancy found that 25(OH)D below 30 ng/mL was associated with a factor of four-to-five increased risk of postpartum hemorrhage [53].
Gestational Diabetes
In a meta-analysis of 31 observational trials, low vitamin D levels increased the risk of gestational diabetes by 49 (OR = 1.49; 95% CI, 1.18-1.89) [54]. Another meta-analysis of 24 observational studies showed similar results [22]. Observational studies also have shown VDD in pregnancy increases the risk of preeclampsia and that vitamin D supplementation, with or without calcium, may reduce that risk [55].
Pulmonary Embolism or Other Embolism
The incidence of pulmonary embolism, a common cause of maternal mortality, has been found in many studies to be increased in a state of maternal VDD, and the risk decreased with supplementation [27,28,30,33,35,37,42-46]. Other studies concluded pulmonary embolism was not influenced by supplementation [31] or that the connection was unclear [34].
Preterm Birth Risk
Reports have conflicting findings on the role of vitamin D in reducing preterm birth risk. Some studies identified the association of VDD and the inflammatory response with premature rupture of the amniotic membrane and preterm delivery [56,57]. Pooled analysis of four randomized controlled trials in that study showed no significant effect of vitamin D supplementation in preventing preterm birth. Other publications have reported alterations in the cervicovaginal fluid content of vitamin D and vitamin D binding protein as biomarkers of vaginal inflammation and preterm birth risk several weeks before delivery [58]. A review published in 2017 reported that based on 6 vitamin D RCTs, vitamin D supplementation could significantly reduce the risk of preterm birth (pooled RR = 0.57 (95% CI, 0.36-0.91)) and from 18 observational studies that maternal 25(OH)D <20 ng/mL was associated with a pooled OR = 1.25 (95% CI, 1.13-1.38) [59]. The best observational study on preterm delivery to date was conducted at the Medical University of South Carolina [60]. A total of 1064 consecutive pregnant women were enrolled at their first prenatal visit around the 12th to 14th week of pregnancy. The participants included 488 whites, 395 African Americans, 117 Hispanics, 19 Asians, and 29 multiple or other ethnicities. Their serum 25(OH)D concentration was measured, and they were given bottles of 5000IU vitamin D3 and counseled on how to achieve 25(OH)D >40 ng/mL. Achieved 25(OH)D was also measured during pregnancy. Those who achieved >40 ng/mL had a 62% lower risk of PTB compared to those <20 ng/mL (p < 0.0001). There was no effect of race/ethnicity on the outcomes.
The journal literature on vitamin D and maternal mortality is relatively limited. However, there is a reasonable body of literature on the role of vitamin D in reducing the risk of adverse pregnancy and birth outcomes for both the developing fetus and mother, e.g., [61]. The review by Wagner et al. [62] outlines important findings regarding complications, including preterm birth, preeclampsia, and gestational diabetes, as well as adverse effects that appear in early childhood, such as asthma and neurological development. This review also points out that vitamin D regulates gene expression through DNA methylation, which has profound effects on fetal development and life after birth. They point out that pregnant women should supplement with 4000-5000 IU/d vitamin D3 and achieve 25(OH)D concentrations >40 ng/mL.
Strengths and Limitations
An important strength of this review is that it presents an overview of reviews of the effect of vitamin D on the risk of many risk factors for maternal morbidity and mortality during pregnancy. Table 1 can serve as a starting point for those wanting to know the results to date and can help guide future research efforts. The studies included here show significant methodological differences, including mixed ethnicities and genetic reservoirs, countries, times and conditions of vitamin D evaluation, and different brands and qualities of vitamin D supplements among studies. Those factors all contributed to the heterogeneity of the included studies. A limitation is that we may not have been able to access all publications on the relationship between vitamin D and maternal mortality and morbidity during pregnancy because we limited our analysis to studies published in English and Spanish and available through the PubMed, Cochrane, and Embase databases.
Conclusions
Our meta-analysis showed evidence to support vitamin D supplementation as a cost- effective public health strategy to minimize adverse maternal health outcomes. Whenever possible, supplementation should be based on initial vitamin D serum levels with the intent to obtain and maintain optimal levels of a minimum of 40 ng/mL throughout the pregnancy for maximum impact [61]. In venues where testing is not affordable or convenient, innovative evidence-based technologies such as the Vitamin D Deficiency Risk Assessment Quiz (beta) and the Vitamin D*Calculator can aid providers of prenatal care in assessing individual VDD risk and calculating an individualized evidence-based loading and maintenance doses based on target optimal blood levels of 40 ng/mL, respectively (GrassrootsHealth.net, accessed 15 September 2022) In light of the results of the present review, further studies should be conducted. Randomized, controlled, blinded vitamin D supplementation trials must be conducted with pregnant women using standard nutrient physiological design criteria to ensure homogeneity of study design [62], including vitamin D levels (baseline and at time of birth) for all participants, to facilitate future systematic review and meta-analyses, In addition, RCT design may not be ideal for vitamin D outcomes studies because vitamin D intake is difficult to quantify from other sources, as well as lack of compliance, which can lead to unclear study results. Alternatively, they could be observational studies with vitamin D supplementation as done at the Medical University of South Carolina [59]. These studies must include large enough sample sizes to permit evaluating the prevalence of maternal mortality and morbidity.
VitaminDWiki - Pregnancy meta-analyses
This list is automatically updated
{category}
VitaminDWiki - Pregnancy and infant-child studies (not covered by this study)
This list is automatically updated
{category}
VitaminDWiki - Pregnancy category contains
{include}
VitaminDWiki - Healthy pregnancies need lots of vitamin D contains
{include}
VitaminDWiki - How to eventually get >40 ng level
- Same dose of vitamin D for everyone is virtually impossible - Dec 2015 based on 36 studies has
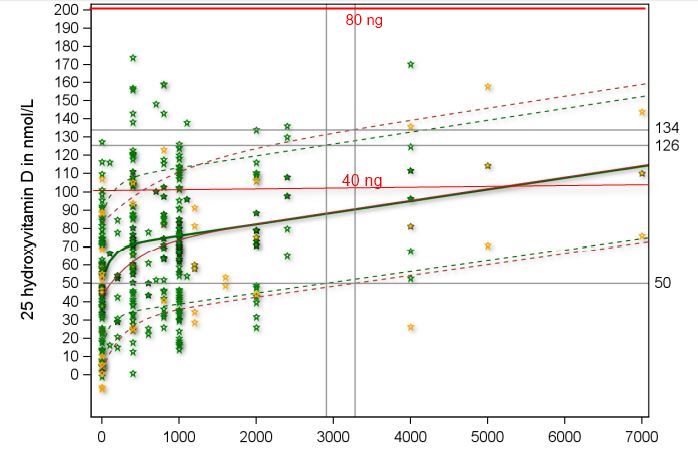
VitaminDWiki - How to quickly get to >40 ng
Overview Loading of vitamin D has the following charts
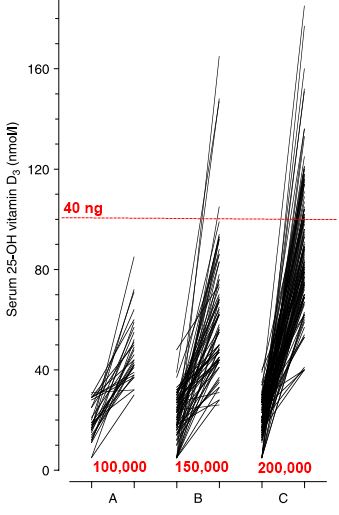
for a total of 100,000 IU, 150,000 IU, and 200,000 IU vary a lot between individuals
There is a HUGE variation in response between individuals
Need a loading dose of at least 4,000 IU/kg to get to get half of people to 40 ng
160lbs = 73 kg ==> 290,000
Thus need 400,000 IU in the first week followed by 50,000 IU weekly
preferably lhave the oading dose before conception - see green chart above
People with poor guts need a gut-friendly form of vitamin D
Can get 50,000 IU Vitamin D anywhere on the globe
For less than $30: Improved conception, Healthy pregnancy aw well as a Healthy infant-child
Continue with 50,000 IU every two weeks after birth
fOmega-3 also makes for healthy preganacies
VitaminDWiki - 40 - 50 ng greatly improves fertility (man as well as woman)
Vitamin D is needed for human fertility – goal is 50 ng – Sept 2018
IVF 4X more successful for white women with lots of vitamin D – many studies
Birth rates doubled with Vitamin D - 300,000 IU for infertile men – RCT Nov 2017