Rationale and Plan for Vitamin D Food Fortification
Rationale and Plan for Vitamin D Food Fortification: A Review and Guidance Paper
published: 17 July 2018 doi: 10.3389/fendo.2018.00373
Risk of Death (for any reason)
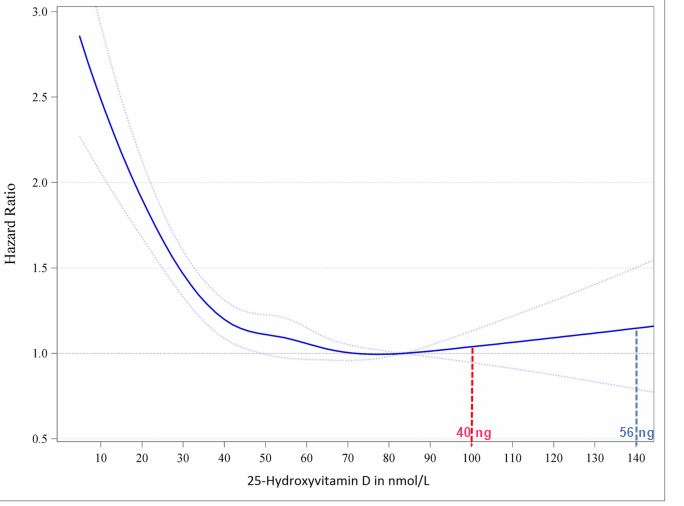
Chart adapted from Much more likely to live longer if higher vitamin D – 27,000 seniors Feb 2017
Chart fails to consider increased deaths if raise vitamin D but not adjust cofactors
such as too much Calcium and to little Magnesium due to increased Vitamin D,
The excess Calcium is then deposited in arteries, muscles, heart organs, etc.
There might be no increased death rate for higher vitamin D levels if the cofactors were also adjusted
More than 800 mg of Calcium increases Cardiovascular events by 85 percent– Nov 2011
Drinking 3 glasses of milk daily associated with doubling the death rate – Oct 2014
Risk of Ischemic Stroke doubles if take more than 1 gram of Calcium daily for years – May 2017
Authors: Piiz S, Marz W , Cashman KD, KieiyME, Whiting SJ, Hoick MF, Grant WB, Piudowski P Hiiigsmann M, Trummer C, Schwetz V, Lerchbaum E, Pandis M, Tomaschitz A, Grubier MR, Gaksch M, Verheyen N, Hoiiis BW, Rejnmark L, Karras SN, Hahn A, Bischoff-Ferrari HA, Reichrath J, Jorde R, Eimadfa I, Vieth R, Scragg R, Caivo MS, van Schoor NM, Bouiiion R, Lips P, Itkonen ST, Martineau AR, Lamberg-Aiiardt C and Zittermann A Draft authors are bolded
Vitamin D deficiency can lead to musculoskeletal diseases such as rickets and osteomalacia, but vitamin D supplementation may also prevent extraskeletal diseases such as respiratory tract infections, asthma exacerbations, pregnancy complications and premature deaths. Vitamin D has a unique metabolism as it is mainly obtained through synthesis in the skin under the influence of sunlight (i.e., ultraviolet-B radiation) whereas intake by nutrition traditionally plays a relatively minor role. Dietary guidelines for vitamin D are based on a consensus that serum 25-hydroxyvitamin D (25[OH]D) concentrations are used to assess vitamin D status, with the recommended target concentrations ranging from >25 to >50 nmol/L (>10->20ng/mL), corresponding to a daily vitamin D intake of 10 to 20 microgram (400-800 international units). Most populations fail to meet these recommended dietary vitamin D requirements. In Europe, 25(OH)D concentrations <30 nmol/L (12ng/mL) and <50 nmol/L (20ng/mL) are present in 13.0 and 40.4% of the general population, respectively. This substantial gap between officially recommended dietary reference intakes for vitamin D and the high prevalence of vitamin D deficiency in the general population requires action from health authorities. Promotion of a healthier lifestyle with more outdoor activities and optimal nutrition are definitely warranted but will not erase vitamin D deficiency and must, in the case of sunlight exposure, be well balanced with regard to potential adverse effects such as skin cancer. Intake of vitamin D supplements is limited by relatively poor adherence (in particular in individuals with low-socioeconomic status) and potential for overdosing. Systematic vitamin D food fortification is, however, an effective approach to improve vitamin D status in the general population, and this has already been introduced by countries such as the US, Canada, India, and Finland. Recent advances in our knowledge on the safety of vitamin D treatment, the dose-response relationship of vitamin D intake and 25(OH)D levels, as well as data on the effectiveness of vitamin D fortification in countries such as Finland provide a solid basis to introduce and modify vitamin D food fortification in order to improve public health with this likewise cost-effective approach.