Prenatal Vitamin D Deficiency - Wagner video
Vitamin D Deficiency: The Indicator of Suboptimal Prenatal Health - video by Dr. Carol Wagner
GLASP AI summary
- (00:07–02:15)
- Dr. Carol Wagner is a professor of pediatrics and neonatology who has conducted multiple NIH-supported randomized controlled trials on vitamin D supplementation in pregnancy, including with Dr. Bruce Hollis.
- (03:02)
- Vitamin D deficiency is framed as a "canary in the coal mine" —a warning sign of suboptimal health in pregnant women.
- It affects maternal and fetal health profoundly, especially during the first 1,000 days (from preconception to age 2).
- (05:18–07:52)
- The U.S. has the highest maternal mortality rate among high-income countries.
- Black women experience three times the rate of maternal death compared to white women, reflecting severe health inequities.
- (11:35–14:14)
- Vitamin D undergoes complex placental and immune-modulatory transformations during pregnancy.
- It influences immune tolerance and fetal development via active hormone (calcitriol) and gene expression effects.
- (18:25–21:16)
- Over 50% of pregnant women are deficient (<20 ng/mL) in vitamin D;
- the rate is >75% among Black American women .
- Optimal levels are ≥40 ng/mL (100 nmol/L), which supports proper 25D to 1,25D conversion.
(27:46–30:20)
Deficiency is associated with:
Higher risk of preeclampsia
Preterm birth
Gingivitis
Impaired fetal growth and enamel development
Increased risk of RSV and neurodevelopmental issues
(30:20–35:18)
- Supplementation of 4,000 IU/day (vs. 400 IU in prenatal vitamins) is safe and effective .
Factors influencing deficiency:
BMI ≥30 (2× risk)
Black race (20× risk vs. white)
Hispanic ethnicity (2.4× risk)
(45:51–50:46)
- Higher doses (2,000–4,400 IU/day) reduced maternal comorbidities and improved infant vitamin D status .
- ~hs` Preterm birth rates were significantly lower in women who achieved ≥40 ng/mL 25D.
- (52:34–57:22)
- Placental and immune biomarkers (e.g. IGF, VEGF, cytokines, vaginal microbiome) were favorably modulated by sufficient vitamin D levels. This suggests wide-reaching developmental and immune effects.
- (1:00:05–1:02:23)
- New studies (2025) confirm inverse relationship between 25D levels and risk of preterm birth. Women delivering before 37 weeks had significantly lower vitamin D levels.
- (1:06:17–1:08:30)
- Lifestyle factors like diet, stress, environment, physical activity , and sleep also influence pregnancy outcomes.
- A holistic approach including optimal vitamin D and healthy habits is advocated.
YouTube entry points
01:14 - Introduction & Dr. Wagner's Background Meet Dr. Carol Wagner and her pioneering work on vitamin D in pregnancy. 01:15
03:39 - Why Maternal Health Matters An overview of the maternal health crisis in the U.S. and globally. 03:40
04:59 - The First 1,000 Days of Life Why preconception to age 2 is critical for long-term health. 05:00
07:29 - Disparities in Maternal Outcomes Black maternal mortality and vitamin D deficiency risks. 07:30
09:59 - The Six Pillars of Health Modifiable lifestyle factors including stress, sleep, diet, and physical activity. 10:00
12:44 - What Is Vitamin D and How Do We Get It? Sunlight, skin pigmentation, and the vitamin D synthesis process. 12:45
13:49 - Beyond Bones: Vitamin D’s Immune Role How vitamin D supports immunity, especially during pregnancy. 13:50
15:09 - Vitamin D Transfer to the Fetus How vitamin D crosses the placenta and impacts fetal development. 15:10
16:54 - Deficiency and Pregnancy Risks Links between vitamin D deficiency and complications like preeclampsia, preterm birth, and more. 16:55
18:59 - A Potent Genetic Enabler Vitamin D’s influence on immune regulation and gene expression. 19:00
20:59 - Prevalence of Deficiency Global and U.S. statistics on vitamin D levels in pregnant women. 21:00
23:29 - Major Physiological Changes During Pregnancy How vitamin D metabolism shifts to meet pregnancy demands. 23:30
24:59 - Why Testing Matters The case for monitoring 25(OH)D levels in maternal care. 25:00
29:59 - RCT Findings: 400 vs. 4,000 IUs Results from key randomized controlled trials on supplementation. 30:00
33:59 - Dose-Response Effects Higher doses result in better maternal and neonatal vitamin D status. 34:00
35:59 - BMI, Skin Color, and Vitamin D Needs Why individualized dosing matters, especially for Black and Hispanic women. 36:00
38:59 - Hormonal Regulation During Pregnancy Vitamin D metabolism becomes independent of parathyroid hormone. 39:00
40:59 - The 40 ng/mL Threshold Why 40 ng/mL is the minimum level needed for optimal conversion. 41:00
43:59 - Is 4,000 IU Safe? Safety data from multiple clinical trials. 44:00
46:59 - Pregnancy Outcomes Improved by Supplementation Lower risks of preeclampsia, infection, and preterm birth. 44:00
50:59 - Vitamin D and Immune Gene Expression Findings from cytokine and placental gene studies. 51:00
54:59 - The Vaginal Microbiome and Vitamin D How vitamin D status influences microbial health. 55:00
56:59 - Summary of the Kellogg and Thrasher Studies Results from major vitamin D trials in pregnancy. 57:00
1:03:59 - Retrospective Study on Gestational Age Lower vitamin D = higher risk of early delivery. 1:04:00
1:06:00 - Final Takeaways on Risk and Prevention Vitamin D is essential, but not the only factor—lifestyle matters. 1:06:01
1:12:13 - Embracing a Holistic Approach
Related studies, a table, and a chart in VitaminDWiki
Prenatal VITAMIN D is more important than other prenatal vitamins
Prenatal vitamins – including vitamin D – reduced autism by 7X in some cases – May 2011
ALL of the top 10 health problems of women are associated with low vitamin D
Overview Pregnancy and vitamin D has
- Healthy pregnancies need lots of vitamin D
- Most were taking 2,000 to 7,000 IU daily for >50% of pregnancy
Click on hyperlinks for details
| ::Problem:: | Vit. D Reduces |
Evidence |
| 0. Chance of not conceiving | 3.4 times | Observe |
| 1. Miscarriage | 2.5 times | Observe |
| 2. Pre-eclampsia | 3.6 times | RCT |
| 3. Gestational Diabetes | 3 times | RCT |
| 4. Good 2nd trimester sleep quality | 3.5 times | Observe |
| 5. Premature birth | 2 times | RCT |
| 6. C-section - unplanned | 1.6 times | Observe |
| Stillbirth - OMEGA-3 | 4 times | RCT - Omega-3 |
| 7. Depression AFTER pregnancy | 1.4 times | RCT |
| 8. Small for Gestational Age | 1.6 times | meta-analysis |
| 9. Infant height, weight, head size within normal limits |
RCT | |
| 10. Childhood Wheezing | 1.3 times | RCT |
| 11. Additional child is Autistic | 4 times | Intervention |
| 12.Young adult Multiple Sclerosis | 1.9 times | Observe |
| 13. Preeclampsia in young adult | 3.5 times | RCT |
| 14. Good motor skills @ age 3 | 1.4 times | Observe |
| 15. Childhood Mite allergy | 5 times | RCT |
| 16. Childhood Respiratory Tract visits | 2.5 times | RCT |
RCT = Randomized Controlled Trial
- Ensure a healthy pregnancy and baby - take Vitamin D BEFORE conception
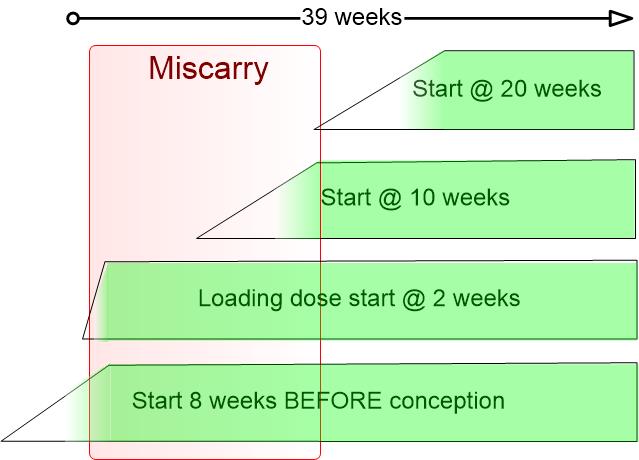
Additional benefits of higher levels of Vitamin D BEFORE conception
Best fertility if high level of vitamin D 3 months before ejaculation - May 2025
Birth rates doubled with Vitamin D - 300,000 IU for infertile men – RCT Nov 2017
Vitamin D is needed for human fertility – goal is 50 ng – Sept 2018
In-vitro Fertilization costs at least 10,000 dollars, Vitamin D costs 5 dollars
Live birth 1.7 X more likely after IVF if good level of vitamin D – meta-analysis Aug 2020
Conception was 3.7X more likely if the male had a good level of Vitamin D – July 2022
Vitamin D improves Infertility in 9 ways (50 references, PDF behind paywall) – May 2023
Pregnancy loss 9X more likely if male had less than 20 ng of Vitamin D – July 2021
Ensure a healthy pregnancy and baby - take Vitamin D before conception
Take prenatal Vitamins 1-3 months before conception, thru pregnancy, and then 6 months after birth
Note: Need 15X more vitamin D than in most prenatals (6,000 IU)