Serious respiratory infection 33% more likely if low Vitamin D
Related in VitaminDWiki
- Respiratory problem 1.9 X more likely if age 2-4 and low Vitamin D
- Respiratory infection, children and Vitamin D - many studies
Hospitals
- People entering hospital with pneumonia with low Vitamin D were 3.5 X more likely to die in 3 months - Nov 2025
- 5,000 IU of Vitamin D daily resulted in far fewer hospitalizations - RCT
- Hospital patients with Vitamin D Deficiency: estimates per 100 vary from 59 to 91 (Nepal)
- 34 percent increase in hospital admissions for low vitamin D in a single year (UK)
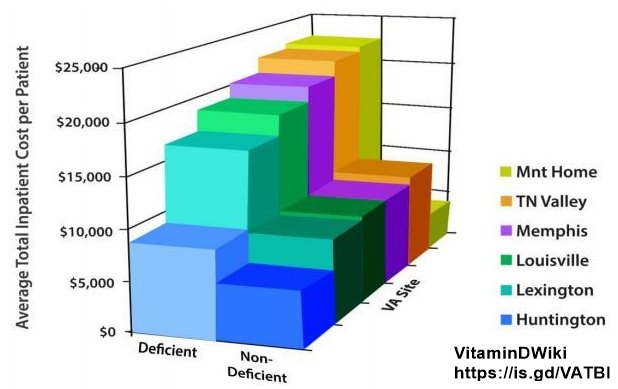
- Hospital costs higher for those with low vitamin D (7,000 Germans in their 50's)
- 5,000 ICU patients have benefited from Vitamin D – need more data
- Vitamin D is needed before many surgeries – many studies and RCTs
VA showed increased vitamin D associated with lower health costs - Lancet May 2012
COVID and Vitamin D
- Children in hospital: those with COVID had lower Vitamin D, Iron, etc.
- COVID infection (without hospitalization) – 1.7X more likely to die in 6 months if low Vitamin D
- 10,000 COVID infections: Hospitalization 2.4X more likely if low vitamin D
- 15.3 X fewer COVID deaths in those getting Vitamin D injections in ICU – RCT
BBC and Vitamin D - Dr. Campbell video
UK Study Links Severe Vitamin D Deficiency to 33% Increased Risk of Respiratory Hospitalization Perplexity AI - Jan 2026
A landmark UK Biobank study published in The American Journal of Clinical Nutrition in January 2026 demonstrates that severe vitamin D deficiency substantially elevates the risk of hospitalization for respiratory tract infections. Led by researchers from the University of Surrey, University of Reading, and University of Oxford, this analysis of 36,258 adults tracked over nearly 15 years reveals that individuals with serum vitamin D levels below 15 nmol/L face a 33% higher risk of hospital admission for respiratory infections—including pneumonia and bronchitis—compared to those with sufficient levels (≥75 nmol/L). Additionally, for every 10 nmol/L increase in vitamin D status, the hospitalization rate decreases by 4%. These findings carry profound implications for public health policy, particularly given that over 50% of UK Asians and more than one-third of Black Africans experience severe vitamin D deficiency during winter months. medicalnewstoday
Study Design and Methodology
Research Framework
The investigation employed an unmatched case-control design utilizing data from the UK Biobank, a comprehensive biomedical research repository encompassing approximately 500,000 adults with linked hospital episode records. The research team analyzed baseline serum 25-hydroxyvitamin D (25[OH]D) measurements—the established biomarker for vitamin D status—alongside long-term hospitalization outcomes captured through the National Health Service (NHS) administrative data. surrey.ac
Lead author Abi Bournot, a BBSRC Food Biosystems PhD Research Fellow at the University of Surrey, designed the study to address a critical gap in understanding the relationship between vitamin D status and respiratory tract infection (RTI) severity across diverse ethnic populations in the UK. The research focused specifically on RTIs requiring hospital admission rather than mild community-managed infections, thereby capturing the most severe and resource-intensive cases. emjreviews
Participant Characteristics and Follow-up
The final analytical cohort comprised 36,258 participants with complete baseline vitamin D measurements and hospital follow-up data. The demographic composition reflected substantial ethnic diversity: 34% White European, 28% Asian, 19% Black African/Caribbean, 11% other ethnicities, and 7% mixed ethnicity. This ethnic heterogeneity was intentional, as vitamin D deficiency prevalence varies dramatically across ethnic groups in the UK population. pubmed.ncbi.nlm.nih
Over a median follow-up period of 14.8 years, 8.5% of participants (3,085 individuals) experienced at least one hospitalization for a respiratory tract infection. These hospitalizations encompassed both upper and lower respiratory tract infections, including bronchitis, pneumonia, and other serious respiratory conditions requiring inpatient medical care. newatlas
Statistical Analyses
The research team employed Cox proportional hazards survival analyses and binary logistic regression models to quantify the association between vitamin D status and RTI hospitalization risk. These statistical approaches allowed researchers to calculate hazard ratios (HRs) while controlling for potential confounding variables including age, sex, and seasonal variation in vitamin D levels. pmc.ncbi.nlm.nih
Vitamin D status was analyzed both as a continuous variable (assessing the impact of each 10 nmol/L increment) and categorically, with participants stratified into five groups: <15 nmol/L (severe deficiency), 15-24 nmol/L (deficiency), 25-49 nmol/L (insufficiency), 50-74 nmol/L (adequacy), and ≥75 nmol/L (optimal/reference category). The research team also tested for potential effect modification by ethnicity using interaction terms in the survival models. pubmed.ncbi.nlm.nih
Primary Findings
Severe Deficiency Confers 33% Elevated Risk
The study's central finding reveals a dose-response relationship between vitamin D status and respiratory hospitalization risk. Participants with severe vitamin D deficiency (<15 nmol/L) demonstrated a 33% higher hazard ratio for RTI-related hospital admission compared to those with optimal levels (≥75 nmol/L) after adjusting for age, sex, and season (HR: 1.33, 95% CI: 1.05-1.67). This magnitude of increased risk is clinically significant and comparable to other established risk factors for respiratory infections. medicalxpress
Notably, intermediate vitamin D categories (15-24 nmol/L, 25-49 nmol/L, and 50-74 nmol/L) did not reach statistical significance compared to the reference group, suggesting that the elevated risk is concentrated among those with the most profound deficiency. This threshold effect indicates that severe vitamin D deficiency represents a critical biological tipping point for immune vulnerability. medicalnewstoday
Linear Dose-Response Relationship
Analyzing vitamin D as a continuous variable revealed a consistent linear relationship: each 10 nmol/L increase in serum 25(OH)D was associated with a 4% reduction in RTI hospitalization risk (HR: 0.96, 95% CI: 0.94-0.99). This finding demonstrates that vitamin D's protective effect operates across a spectrum rather than representing a simple threshold phenomenon. The consistency of this association throughout the vitamin D concentration range suggests a fundamental biological relationship between vitamin D status and respiratory infection susceptibility. epocrates
Universal Risk Across Ethnic Groups
A critical aspect of the analysis examined whether the vitamin D-RTI association differed by ethnicity. The inclusion of an interaction term for 25(OH)D × ethnicity in the survival models revealed no statistically significant interaction. This finding indicates that the elevated risk associated with low vitamin D applies consistently across White, Asian, Black, mixed, and other ethnic populations. Given the dramatically higher prevalence of vitamin D deficiency in ethnic minority communities, this universal risk pattern underscores the urgent need for targeted public health interventions in these populations. unmc
Mechanistic Understanding: How Vitamin D Protects Against Respiratory Infections
Innate Immunity and Antimicrobial Peptides
Vitamin D's protective role against respiratory infections operates through multiple immunological pathways, with antimicrobial peptide induction representing a primary mechanism. When immune cells encounter pathogens through toll-like receptors (TLRs), they upregulate both vitamin D receptor (VDR) expression and the enzyme CYP27B1, which converts inactive 25-hydroxyvitamin D into the active form, 1,25-dihydroxyvitamin D (1,25[OH]₂D). academic.oup
The active vitamin D metabolite directly stimulates transcription of the cathelicidin antimicrobial peptide (CAMP) gene, which produces the antimicrobial peptide LL-37. This regulation is human-specific and involves a classical vitamin D response element (VDRE) in the CAMP gene promoter located approximately 615 base pairs upstream from the transcriptional start site. Cathelicidin disrupts bacterial cell membranes, neutralizes viruses, and additionally functions as a signaling molecule to activate broader immune responses. pmc.ncbi.nlm.nih
Research demonstrates that TLR2/1 activation by bacterial lipopeptides (such as those from Mycobacterium tuberculosis) enhances antimicrobial capacity of monocytes through a vitamin D-dependent pathway, inducing both cathelicidin expression and its antimicrobial protein product. Beyond cathelicidin, vitamin D also influences β-defensin antimicrobial peptides, though this regulation is more complex and typically requires additional cofactors beyond vitamin D alone. sciencedirect
Macrophage Function and Phagocytosis
Recent research reveals that 1,25(OH)₂D promotes development of macrophages expressing elevated levels of complement receptor immunoglobulin (CRIg), a unique complement receptor critical for phagocytosis and bacterial clearance. Macrophages differentiated in the presence of 1,25(OH)₂D demonstrate significantly enhanced phagocytic activity against both bacterial (Staphylococcus aureus) and fungal (Candida albicans) pathogens. This enhanced phagocytosis translates directly to improved pathogen clearance capacity. nature
Furthermore, vitamin D facilitates local production of active 1,25(OH)₂D by macrophages themselves following TLR1/2 engagement, creating an autocrine amplification loop that enhances innate immune responses. In highly inflammatory conditions, M1 macrophages can produce sufficient levels of 1,25(OH)₂D to modify T cell responses and regulate inflammation through a vitamin D-mediated negative feedback mechanism. pmc.ncbi.nlm.nih
Autophagy Enhancement
Vitamin D robustly enhances autophagy, a cellular process critical for combating intracellular pathogens such as Mycobacterium tuberculosis and various viral infections. The active vitamin D metabolite has been documented to inhibit mammalian target of rapamycin (mTOR), a protein kinase that suppresses autophagy when active. By inhibiting mTOR, vitamin D effectively releases the brake on autophagic pathways, enabling cells to degrade intracellular pathogens more efficiently. The vitamin D receptor has even been identified as a master transcriptional regulator of autophagy genes in certain cell types. pmc.ncbi.nlm.nih
Immunomodulation and Inflammation Regulation
Beyond enhancing pathogen killing, vitamin D exerts sophisticated immunomodulatory effects that balance protective immunity with inflammation control. Active vitamin D influences dendritic cell maturation, promoting tolerogenic dendritic cells that suppress excessive inflammatory responses. This effect includes dose-dependent reduction in transcription of pro-inflammatory Th1 cytokines (IL-2, GM-CSF, interferon-γ) and increased expression of anti-inflammatory Th2 cytokines (IL-4, IL-5, IL-10). pmc.ncbi.nlm.nih
Vitamin D also inhibits production of pro-inflammatory cytokines including IL-12, TNF-α, and IL-17 while promoting regulatory T cell development and recruitment through increased chemokine CCL22 expression. This immunomodulatory capacity appears particularly important for preventing cytokine storms and excessive inflammatory lung damage during severe respiratory infections. The vitamin D-cathelicidin axis additionally activates autophagy and modulates inflammatory pathways simultaneously, providing coordinated antimicrobial and anti-inflammatory effects. pmc.ncbi.nlm.nih
Prevalence and Public Health Burden of Vitamin D Deficiency in the UK
Alarming Deficiency Rates in Ethnic Minority Communities
The UK faces a vitamin D deficiency crisis of startling magnitude, particularly affecting ethnic minority populations. A comprehensive analysis of 440,581 UK Biobank participants found that 57.2% of individuals of Asian ancestry exhibited severe vitamin D deficiency (<25 nmol/L) during winter/spring months, with rates remaining elevated at 50.8% even during summer/autumn. Black African populations demonstrated the second-highest vulnerability, with 38.5% experiencing severe deficiency in winter and 30.8% in summer. Mixed ancestry individuals (36.5% in winter, 22.5% in summer) and Chinese participants (33.1% in winter, 20.7% in summer) also showed elevated deficiency rates. unisa.edu
By comparison, White European populations exhibited considerably lower—though still concerning—severe deficiency prevalence: 17.5% in winter dropping to 5.9% in summer. This stark seasonal variation reflects the population's greater capacity for vitamin D synthesis from sunlight when UVB exposure is adequate. Overall, approximately 55.4% of the UK population has either insufficient (25-50 nmol/L) or deficient (<25 nmol/L) vitamin D status. pmc.ncbi.nlm.nih
The dramatically higher deficiency rates in populations with darker skin result from elevated melanin concentrations, which reduce the skin's capacity to synthesize vitamin D from UVB radiation. This biological vulnerability is compounded by cultural factors including modest dress practices that limit skin exposure, reduced dietary intake of vitamin D-rich foods (particularly oily fish), lower supplement usage rates, and higher proportions living in socioeconomically deprived circumstances. openaccess.sgul.ac
Seasonal and Geographic Variations
Vitamin D deficiency demonstrates pronounced seasonal patterns throughout the UK, with serum 25(OH)D concentrations typically declining by approximately 50% from peak levels in September to a nadir in February. Between October and early March, residents of the UK cannot synthesize adequate vitamin D from sunlight exposure alone due to the sun angle at northern latitudes. During these winter months, even White European populations see deficiency prevalence increase dramatically. medindia
Geographic location within the UK also significantly influences vitamin D status. Nearly one-third of study participants living in Edinburgh and Glasgow recorded low vitamin D levels in winter, substantially higher than rates observed in southern UK residents from comparatively higher socioeconomic regions. Scotland demonstrated significantly higher odds of both vitamin D deficiency and insufficiency compared to other UK regions. This latitude effect reflects reduced UVB radiation intensity at more northern locations. unisa.edu
Populations at Elevated Risk
Beyond ethnic minorities, several population groups face elevated vitamin D deficiency risk requiring year-round supplementation consideration: cios.icb.nhs
Institutionalized individuals: Residents of care homes and other institutions with limited outdoor exposure demonstrate particularly high deficiency rates. nhs
Limited mobility populations: Frail or housebound individuals who rarely venture outdoors cannot maintain adequate vitamin D through sun exposure. medindia
Cultural dress practices: Individuals who habitually wear clothing covering most skin for religious or cultural reasons have limited capacity for cutaneous vitamin D synthesis. nhs
Socioeconomic disadvantage: Lower socioeconomic groups exhibit higher deficiency prevalence across all ethnic categories, likely reflecting reduced supplement usage, lower consumption of vitamin D-rich foods, and less leisure time for outdoor activities. academic.oup
Age-related factors: Both young children and older adults face elevated risk, with children from South Asian (43% deficient) and Black African/Caribbean (28% deficient) backgrounds showing particularly alarming deficiency rates compared to White European children (3% deficient). openaccess.sgul.ac
Clinical and Interventional Evidence: Vitamin D Supplementation for Respiratory Infection Prevention
Meta-Analytic Evidence and Treatment Efficacy
A comprehensive 2021 meta-analysis of 43 randomized controlled trials (RCTs) involving 48,488 participants found that vitamin D supplementation provided modest but significant protection against acute respiratory infections overall (OR 0.92, 95% CI: 0.86-0.99). However, a 2025 update incorporating six additional large trials (total: 49 RCTs, 64,573 participants) found the intervention no longer reached statistical significance for overall ARI risk (OR 0.94, 95% CI: 0.88-1.00, p=0.057). pubmed.ncbi.nlm.nih
Despite the marginal overall effect, critically important subgroup analyses reveal substantial heterogeneity based on baseline vitamin D status and dosing regimen. The protective effect concentrates heavily among individuals with baseline vitamin D deficiency or insufficiency, whereas those already vitamin D sufficient derive minimal additional benefit from supplementation. bmj
Dosing Regimens and Optimal Strategies
Daily low-dose supplementation emerges as the most effective preventive strategy. Meta-analyses consistently demonstrate that daily doses between 400-1200 IU during autumn, winter, or spring provide modest protection against ARIs. A meta-analysis of pediatric populations found that daily doses ≤1000 IU were associated with significant reductions in ARI incidence, whereas higher doses conferred no benefit. This dose-response pattern suggests an optimal therapeutic window exists for respiratory protection. pubmed.ncbi.nlm.nih
High monthly bolus dosing demonstrates mixed results. A randomized clinical trial in long-term care residents (mean age 84 years) found that monthly high-dose vitamin D (100,000 IU monthly, averaging 3,300-4,300 IU daily) reduced acute respiratory illnesses by 40% compared to standard low-dose supplementation (400-1,000 IU daily). However, the high-dose group experienced more than twice the incidence of falls, highlighting important safety trade-offs. Other studies examining intermittent bolus regimens (weekly or less frequent) have generally shown inferior efficacy compared to daily dosing. news.cuanschutz
Population-specific effects: Military conscripts in Finland with insufficient baseline vitamin D levels exhibited significantly more ARIs compared to those with sufficient levels (OR 2.11, 95% CI: 1.19-3.74), with vitamin D insufficiency inversely associated with cathelicidin concentration (OR 0.49, 95% CI: 0.24-0.99). This finding provides direct mechanistic evidence linking vitamin D status to antimicrobial peptide production and infection risk. infectiousdiseaseadvisor
Influenza-specific protection: Although vitamin D supplementation shows inconsistent effects across all respiratory viruses, several trials document specific protective effects against influenza A. High-dose vitamin D supplementation (versus low-dose) reduced influenza A infection rates by 61% (OR 0.39, 95% CI: 0.26-0.59). A pediatric RCT in Japan found that 1,200 IU/d vitamin D supplementation reduced influenza A incidence but not influenza B incidence. jamanetwork
Economic Evaluations and Cost-Effectiveness
Multiple economic analyses demonstrate that vitamin D supplementation represents a highly cost-effective or cost-saving intervention for preventing ARIs. A Colombian cost-utility analysis of pediatric vitamin D supplementation found the intervention to be cost-dominant, associated with both lower costs (US$1,354 vs US$1,948 per person) and higher quality-adjusted life-years (0.99 vs 0.98 QALYs) compared to no supplementation over six months. The intervention generated savings of US$594 per patient treated. pmc.ncbi.nlm.nih
Probabilistic sensitivity analyses showed vitamin D supplementation had a 96% probability of being cost-effective at willingness-to-pay thresholds as low as US$4,000 per QALY gained. A similar analysis focused on preventing pneumonia recurrence in children found vitamin D supplementation cost-effective from a societal perspective, though results were sensitive to the relative risk magnitude assumed. pmc.ncbi.nlm.nih
These economic evaluations support vitamin D supplementation as a high-value public health intervention that simultaneously reduces healthcare costs while improving population health outcomes. Given the substantial economic burden of respiratory tract infections—which generate high costs due to their frequency—cost-effective preventive strategies merit serious policy consideration. pmc.ncbi.nlm.nih
UK Public Health Recommendations and Policy Landscape
Current Official Guidance
The UK government, based on recommendations from the Scientific Advisory Committee on Nutrition (SACN) following its comprehensive 2016 Vitamin D and Health report, advises that everyone over age 4 should consider taking a daily supplement containing 10 micrograms (400 IU) of vitamin D during autumn and winter months (October through March). This recommendation reflects the reality that UK residents cannot synthesize adequate vitamin D from sunlight during these months due to the sun angle at northern latitudes. bmj
For higher-risk populations—including those who spend little time outdoors, individuals who cover most of their skin when outside, people with darker skin pigmentation, and residents of care facilities—the guidance recommends year-round supplementation with 10 micrograms daily. Pregnant and breastfeeding women are also advised to maintain vitamin D supplementation throughout pregnancy and lactation. cios.icb.nhs
The SACN established the reference nutrient intake (RNI) at 10 micrograms (400 IU) daily based on the amount needed for most of the population to maintain serum 25(OH)D concentrations at or above 25 nmol/L when UVB sunshine exposure is minimal. This target specifically addresses musculoskeletal health protection, though SACN noted in a December 2020 review that this dosage may provide additional benefit in reducing acute respiratory tract infection risk. gov
Fortification Policy and Implementation Gaps
Unlike most other high-latitude Western countries, the UK does not mandate vitamin D fortification of staple foods. Fortification remains entirely voluntary for food producers, with fat spreads (margarines and plant oil-based spreads) and breakfast cereals representing the most commonly fortified items. Margarine was subject to mandatory vitamin D fortification until 2013, when the requirement was removed as part of a government-wide deregulation initiative. gov
In spring 2022, the Department of Health and Social Care launched a comprehensive review to promote vitamin D importance and identify strategies to improve population intake, including potential mandatory fortification. SACN's 2024 rapid review on fortification concluded that evidence from countries with existing vitamin D fortification policies suggests an appropriately designed and well-implemented mandatory fortification program has potential to improve UK population vitamin D status. gov
However, SACN emphasized that an effective fortification policy would require careful modeling to identify suitable foods reaching all population groups (including those consumed by groups at risk of deficiency), assess safe fortification levels accounting for existing fortified foods and supplement usage, and determine appropriate vitamin D forms (D₂ versus D₃). The challenge is particularly acute for South Asian populations, who are more likely to consume millet and rice than wheat, complicating strategies focused on wheat fortification. nutricomms
Healthy Start Scheme and Access Barriers
The UK's Healthy Start scheme provides free vitamin D-containing supplements to eligible pregnant women, women with children under 12 months, and children aged 6 months to 4 years from low-income families. This targeted program aims to address vitamin D deficiency in populations facing both biological vulnerability (pregnancy, infancy) and socioeconomic barriers to supplement access. notts.icb.nhs
Despite these governmental recommendations and the Healthy Start program, substantial proportions of the UK population maintain poor vitamin D status, suggesting that current strategies have had limited impact. Low-cost vitamin D supplements are available from most pharmacies and supermarkets, yet uptake remains suboptimal. General practices in many regions no longer routinely prescribe vitamin D supplements for regular treatment, instead directing patients toward over-the-counter products. notts.icb.nhs
This implementation gap between policy recommendations and population behavior underscores the need for more effective public health interventions, potentially including mandatory fortification, enhanced public awareness campaigns targeting high-risk populations, and reduced financial barriers to supplement access. gov
Respiratory Disease Burden and the Public Health Imperative
Mortality and Morbidity Impact
Respiratory tract infections impose a devastating global health burden, ranking among the leading causes of death worldwide. In 2021, lower respiratory infections remained the world's most deadly communicable disease aside from COVID-19, positioned as the fifth leading cause of death globally. These infections resulted in 2.74 million deaths in 2015, representing 4.8% of all deaths that year. Among low-income countries specifically, lower respiratory infections constituted the leading cause of death in 2021. pmc.ncbi.nlm.nih
The mortality burden concentrates heavily among two vulnerable populations: children under 5 years and adults over 70 years. Lower respiratory tract infections (pneumonia and bronchitis) rank among the top 20 leading causes of mortality globally for individuals aged 50-74 years and in the top 10 for those aged 75 and older. Streptococcus pneumoniae remains the leading bacterial cause of lower respiratory infection deaths (505,268 deaths in 2021), followed by Staphylococcus aureus (423,837 deaths) and Klebsiella pneumoniae. thelancet
Long-term Consequences and Excess Mortality
The impact of respiratory infections extends far beyond the acute illness episode. A landmark eight-decade longitudinal study from the UK found that individuals who experienced a lower respiratory tract infection before age 2 years faced a 93% increased risk of premature death from respiratory disease as adults (by age 73) compared to those without early childhood LRTI. This association remained robust after adjusting for childhood socioeconomic disadvantage and adult smoking status. hcplive
Early childhood LRTI accounted for one in five (20.4%) premature adult deaths from respiratory disease across England and Wales, translating to an estimated 179,188 excess deaths between 1972 and 2019. By comparison, adult smoking—the dominant respiratory risk factor—accounted for three in five (57.7%) of these premature deaths. The magnitude of respiratory disease burden linked to early childhood infection rivals that of major lifestyle risk factors. thelancet
Furthermore, contracting a lower respiratory tract infection in adulthood dramatically elevates mortality risk in subsequent months. Among hospitalized LRTI patients, 30-day mortality risk reached 5.8% and 360-day risk was 18.3%—representing increases of 7.5-fold and 2.6-fold respectively compared to matched comparison patients. Even ambulatory LRTI patients demonstrated 6.5-fold and 2.1-fold elevated mortality risk at 30 and 360 days. cidrap.umn
Healthcare System Strain and Economic Costs
Respiratory tract infections create substantial strain on healthcare systems through emergency department visits, hospital admissions, and intensive care requirements. The economic burden stems not only from direct medical costs but also from productivity losses, long-term disability, and premature mortality. In the UK specifically, respiratory disease mortality has remained higher than in comparable EU15+ countries between 1985 and 2015, with elevated mortality observed for obstructive, interstitial, and infectious respiratory disease subcategories. bmj
Each hospital admission for a respiratory infection represents a preventable healthcare utilization event that could potentially be averted through cost-effective interventions targeting modifiable risk factors. The current UK study's finding that severe vitamin D deficiency increases RTI hospitalization risk by 33% suggests that addressing this widespread nutritional deficiency could reduce admissions, alleviate NHS pressures, and generate substantial healthcare cost savings. surrey.ac
Limitations and Research Considerations
Observational Design and Causality
The UK Biobank study employed an observational case-control design that identifies associations but cannot definitively establish causation. While the 33% increased risk associated with severe vitamin D deficiency is substantial and biologically plausible given known immunological mechanisms, the possibility remains that low vitamin D serves as a marker of poor health or other unmeasured confounding factors rather than a direct causal agent. emjreviews
Reverse causation represents a particular concern: individuals with underlying health conditions that increase infection susceptibility may also have behaviors or physiological states that reduce vitamin D status (reduced outdoor activity, chronic inflammation, etc.). However, the biological mechanisms linking vitamin D to antimicrobial peptide production, macrophage function, and immune modulation provide strong mechanistic support for a causal relationship. ashpublications
Vitamin D Measurement Timing
A substantial proportion (75%) of hospitalized cases had vitamin D measured as an inpatient, while others had measurements taken at variable intervals before admission (median 51 days). Acute illness and hospitalization can themselves affect vitamin D metabolism and measurement, potentially introducing measurement error. However, the study's large sample size and long follow-up period help mitigate concerns about measurement timing affecting overall conclusions. pmc.ncbi.nlm.nih
Generalizability and Population Representativeness
The UK Biobank cohort, while large and ethnically diverse, may not fully represent the broader UK population. Participants are generally healthier and more health-conscious than the general population, potentially underestimating the true magnitude of vitamin D-related respiratory infection risk in more vulnerable communities. Additionally, the median follow-up of 14.8 years means that vitamin D measurements occurred in the mid-2000s to early 2010s, and vitamin D status may have changed substantially during the lengthy follow-up period. medicalnewstoday
Intervention Trial Evidence Gaps
While the observational evidence linking vitamin D deficiency to respiratory infection risk is compelling, randomized controlled trials of vitamin D supplementation show more modest and inconsistent effects on respiratory infection outcomes. The most recent 2025 meta-analysis found that vitamin D supplementation no longer reached statistical significance for overall ARI prevention (p=0.057), though the point estimate still favored a protective effect. pmc.ncbi.nlm.nih
This discrepancy between observational and interventional evidence may reflect several factors: trials often supplement individuals who are not severely deficient at baseline (diluting observed effects), bolus dosing regimens prove less effective than daily administration, trial durations may be insufficient to capture effects, and vitamin D may require longer-term repletion to optimize immune function rather than providing immediate protection. Future trials should specifically target severely deficient populations with daily supplementation regimens to definitively test whether correcting severe deficiency reduces respiratory infection risk. sciencedirect
Conclusions and Public Health Implications
The University of Surrey-led UK Biobank study provides robust epidemiological evidence that severe vitamin D deficiency (<15 nmol/L) substantially elevates the risk of serious respiratory tract infections requiring hospitalization. The 33% increased risk documented in this 36,258-participant cohort, coupled with the consistent 4% risk reduction per 10 nmol/L vitamin D increase, establishes vitamin D status as a significant modifiable risk factor for respiratory infection morbidity. newatlas
This relationship operates consistently across diverse ethnic populations, even as deficiency prevalence varies dramatically—from over 50% in UK Asian communities to approximately 17% in White Europeans during winter months. The mechanistic understanding of vitamin D's role in antimicrobial peptide production, macrophage function, autophagy enhancement, and immune regulation provides biological plausibility supporting a causal interpretation of the observational findings. academic.oup
Given that lower respiratory tract infections rank as the fifth leading cause of death globally and that respiratory disease mortality in the UK exceeds that of comparable European nations, interventions targeting modifiable risk factors carry substantial public health importance. Vitamin D supplementation represents a low-cost, safe, and potentially cost-effective strategy for reducing respiratory infection burden, particularly among severely deficient populations. en.wikipedia
Current UK guidance recommending 10 micrograms (400 IU) daily supplementation during autumn and winter—with year-round supplementation for high-risk groups—aligns with the study findings. However, implementation remains suboptimal, with large proportions of the population failing to achieve adequate vitamin D status despite these recommendations. Enhanced public health strategies warrant serious consideration, including: bhf.org
Targeted outreach to high-risk populations: Intensive public health messaging specifically directed toward Asian, Black African/Caribbean, and other ethnic minority communities experiencing alarmingly high deficiency rates. pmc.ncbi.nlm.nih
Mandatory food fortification: Following models from Finland, Norway, and other countries that have successfully raised population vitamin D status through fortified staple foods. pmc.ncbi.nlm.nih
Reduced financial barriers: Expanding the Healthy Start scheme and ensuring vitamin D supplements remain affordable and accessible, particularly in socioeconomically disadvantaged communities. northyorkshireccg.nhs
Healthcare provider education: Ensuring physicians, pharmacists, and other healthcare professionals actively screen for and counsel about vitamin D deficiency risk factors. unmc
Seasonal supplementation campaigns: Public health campaigns timed to autumn months encouraging population-wide vitamin D supplementation initiation as sunlight exposure declines. theros.org
The convergence of epidemiological evidence, mechanistic understanding, and economic analyses supports vitamin D deficiency as a tractable public health target with potential to reduce respiratory infection morbidity, alleviate healthcare system strain, and improve population health outcomes—particularly during winter months when both deficiency prevalence and respiratory infection incidence peak simultaneously. While definitive proof of causality awaits large-scale randomized trials targeting severely deficient populations with appropriate daily dosing regimens, the existing evidence base justifies immediate action to address the vitamin D deficiency pandemic through comprehensive public health interventions.