Iceland and Vitamin D - many studies
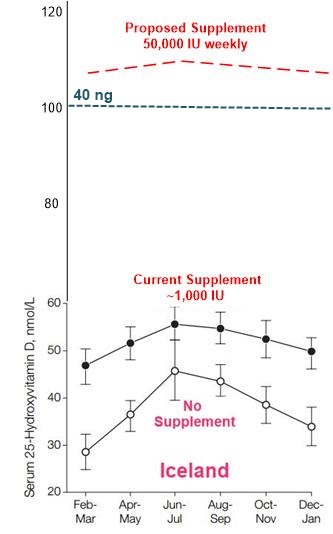
Iceland discussion of weekly 50,000 IU of vitamin D - March 2023
Health can be greatly improved by weekly 50,000 IU of Vitamin D - video Lahore - March 2023
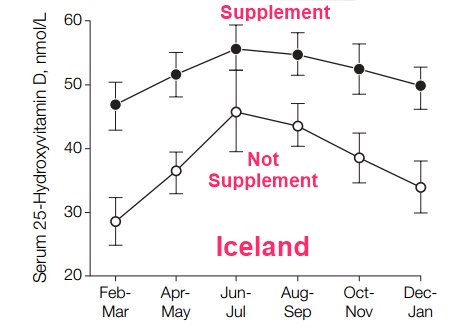
Iceland Vitamin D level 46 nmol (18 ng) - 2005
Relationship between serum parathyroid hormone levels, vitamin D sufficiency, and calcium intake.
JAMA 294:2336-2341 URL: http://www.ncbi.nlm.nih.gov/pubmed/16278362
Steingrimsdottir L et al
Details: Age: 30-85
Gender: Men and Women
Vitamin D Levels (nmol/L): 46.1
Number of participants: 944
📄 Download the PDF from VitaminDWiki
Icelanders supplementing had 19 nmol higher levels in the winter (~1,000 IU)
Minimum anticipated response to 50,000 IU weekly
Anticipate even bigger response by giving
more D to Obese, Asthmatic, smoker, MS, HIV, Diabetic, no gallbladder, stomach by-passed, Depression, poor health, Seniors, etc
Gut-Friendly Vitamin D to those with poor guts
Magnesium to everyone
See also: Depression in Icelandic men 2.5 X more likely if vitamin D deficient – Nov 2015
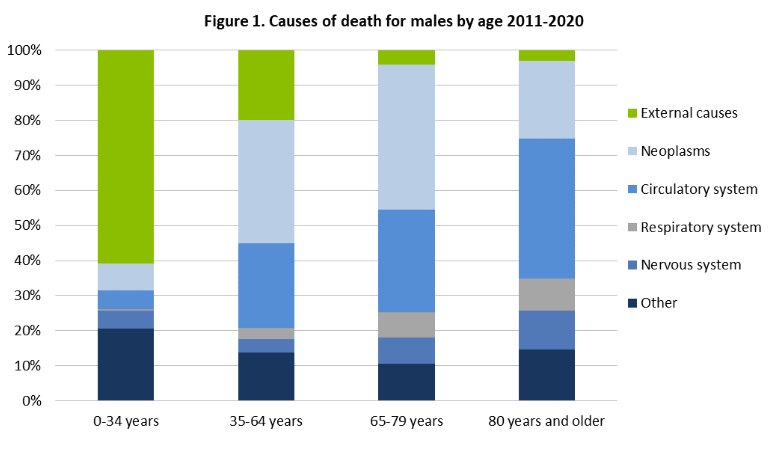
Cancer is a leading cause of Icelandic adult death (Note: vit D prevents many cancers)
Some Vitamin D and Cancer in VitaminDWiki
Cancer risk reduced 65 percent by vitamin D levels greater than 40 nanograms – April 2016
Vitamin D fortification could eliminate 1 in 10 Cancer deaths in the EU – May 2022
100-year history of Vitamin D: from discovery thru COVID - in Icelandic with English Translation
1 page Editorial bjorngu@landspitali.is
📄 Download the Icelandic from VitaminDWiki
📄 Download the English translation from VitaminDWiki
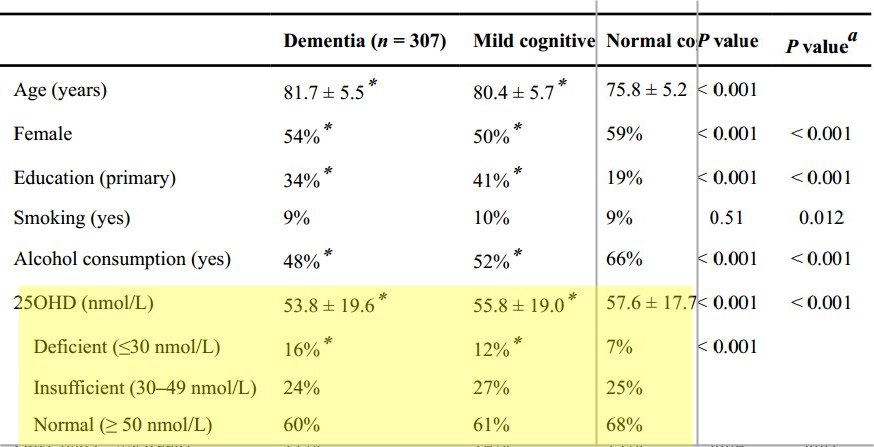
Icelanders (like others) with dementia have low levels of vitamin D - April 2020
Lifestyle and 25-hydroxy-vitamin D among community-dwelling old adults with dementia, mild cognitive impairment, or normal cognitive function
Aging Clinical and Experimental Research vol32, pg 2649–2656 https://doi.org/10.1007/s40520-020-01531-1
Hrafnhildur Eymundsdottir, M. Chang, O. G. Geirsdottir, L. S. Gudmundsson, P. V. Jonsson, V. Gudnason, L. Launer, M. K. Jonsdottir & A. Ramel
Background
Several studies have indicated that older adults with cognitive impairment have a poorer lifestyle than their healthy peers including lower 25-hydroxy-vitamin D levels (25OHD).
Aim: To investigate the associations between lifestyle and 25OHD depending on cognitive status among old adults.
Methods
Community-dwelling old adults (65–96 years) participated in this cross-sectional study based on the Age-Gene/Environment-Susceptibility-Reykjavik-Study. The analytical sample included 5162 subjects who were stratified by cognitive status, i.e., dementia (n = 307), mild cognitive impairment (MCI, n = 492), and normal cognitive status (NCS, n = 4363). Lifestyle variables were assessed and 25OHD was measured. The associations between lifestyle and 25OHD were calculated using linear models correcting for potential confounders.
Results
According to linear regression models, 25OHD was significantly lower in older people with dementia (53.8 ± 19.6 nmol/L) than in NCS participants (57.6 ± 17.7 nmol/L). Cod liver oil (7.1–9.2 nmol/L, P < 0.001) and dietary supplements (4.4–11.5 nmol/L, P < 0.001) were associated with higher 25OHD in all three groups. However, physical activity ≥ 3 h/week (2.82 nmol/L, P < 0.001), BMI < 30 kg/m2 (5.2 nmol/L, P < 0.001), non-smoking (4.8 nmol/L, P < 0.001), alcohol consumption (2.7 nmol/L, P < 0.001), and fatty fish consumption ≥ 3x/week (2.6 nmol/L, P < 0.001) were related to higher 25OHD in NCS only, but not in participants with dementia or MCI.
Discussion
Older people living in Iceland with dementia are at higher risk for 25OHD deficiency when compared to healthy individuals. Physical activity reported among participants with dementia, and MCI is low and is not significantly associated with 25OHD.
Conclusions
Lifestyle factors among NCS participants are associated with 25OHD levels. Importantly, healthy lifestyle should be promoted among individuals with MCI and dementia.
📄 Download the PDF from VitaminDWiki
See in VitaminDWiki Dementia is associated with low vitamin D - many studies
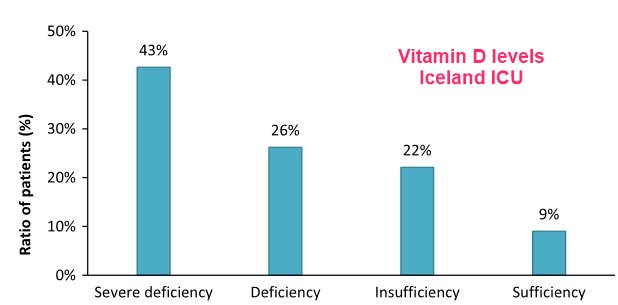
Fewer than 9% of Icelandic ICU patients had more than 30 ng of Vitamin D - June 2016
Severe vitamin D deficiency is common in critically ill patients at a high northern latitude
https://doi.org/10.1111/aas.12748
R. B. Kvaran, M. I. Sigurdsson, S. J. Skarphedinsdottir, G. H. Sigurdsson
Background
Critically ill patients at southern latitudes have been shown to have low vitamin D levels that were associated with prolonged hospital stay. To our knowledge no studies have been conducted on vitamin D status amongst critically ill patients at high northern latitudes. Despite the Icelandic population traditionally taking vitamin D supplements, we hypothesized that the majority of critically ill patients in Reykjavik, Iceland have low vitamin D levels.
Methods
This was a prospective observational study on 122 patients admitted to Landspitali University Hospital intensive care unit. Serum vitamin D (25(OH)D) was measured in all patients on two occasions (first and second day). The prevalence of vitamin D deficiency and its effect on hospital stay was calculated.
Results
Only 9% of patients had vitamin D levels recommended for good health (>75 nmol/l) and 69% were deficient (25(OH)D < 50 nmol/l). The average difference between the first and second vitamin D samples was 2.8 nmol/l. Forty-three percent of the severely vitamin D deficient stayed in the ICU for more than 4 days compared to 19% of patients with better status (P = 0.196).
Discussion
Vitamin D deficiency is very common in critically ill patients at high northern latitudes and patients with severely deficient vitamin D levels had trend towards longer intensive care unit stay. Furthermore, 43% of the patients had vitamin D levels under 25 nmol/l that is associated with osteomalacia. It appears that a single vitamin D measurement gives a reasonable clue about the vitamin D status in critically ill patients.
📄 Download the PDF from Sci-Hub via VitaminDWiki
Vitamin-D homeostasis amongst adult Icelandic population - 2004 (46 nmol average)
Laeknabladid. 90(1):29-36 [Article in Icelandic] PMID: 16819011
Oervar Gunnarsson 1 , Olafur Skúli Indriðason, Leifur Franzson, Edda Halldórsdóttir, Gunnar Sigurðsson
1 Division of endocrinology and metabolism, Iceland University Hospital, Fossvogi, 108 Reykjavík, Iceland. gunnars@landspitali.is.
Background: The purpose of this study was to examine the effect of vitamin D intake and production in skin on vitamin D homeostasis in adult Icelanders.
Methods: Participants were 30-85 years old, randomly selected from the registry of the Reykjavik area (64 degrees N) and answered a thorough questionnaire on diet and vitamin supplements. Concentrations of 25(OH)-vitamin D [25(OH)D] in peripheral blood were examined based on season during the study period February 2001-January 2003, vitamin D intake and age (age groups 30-45, 50-65, and 70-85 years old). We defined vitamin D deficiency as either [25(OH)D] <25 nmol/l or as [25(OH)D] where the inverse relationship between serum iPTH and [25(OH)D] became statistically significant.
Results: Of 2310 invited, 1630 subjects participated (70,6% participation) but 21 individuals were excluded due to primary hyperparathyroidism. Mean [25(OH)D] was 46.5-/+20 nmol/l but varied by season, age and vitamin D intake, highest in June-July, 52.1-/+19.8 and lowest in February-March, 42.0-/+20.5 (p<0.001). [25(OH)D] was highest in the oldest age group, 50.8-/+19.7, but lowest in the youngest, 42.5-/+20 as was the intake 16.6-/+10 microg/day compared to 9.9-/+9 microg/day in the youngest. The correlation between vitamin D intake and [25(OH)D] was highest for the oldest group, r=0.41, p<0.001 but lowest in the youngest, r=0.24, p<0.001. [25(OH)D] was significantly higher among users of vitamin supplements (45.4-/+19.7) or fish oil (53.0-/+18.4) than among non-users (38.0-/+18.9). Vitamin D insufficiency was seen among 14.5% of those participating according to traditional definition, but 50% were below [25(OH)D] of 45 nmol/l where negative correlation between [25(OH)D] and PTH became statistically significant.
Conclusions: The serum concentration of 25(OH)D at which vitamin D deficiency becomes biochemically significant is higher than traditionally thought. A daily intake of 15-20 microg/day during wintertime would be required to maintain normal homeostasis in Icelandic adults, which is considerably higher than present recommendations of 7-10 microg/day for adults. Further research is needed to define the limit for vitamin-D sufficiency.
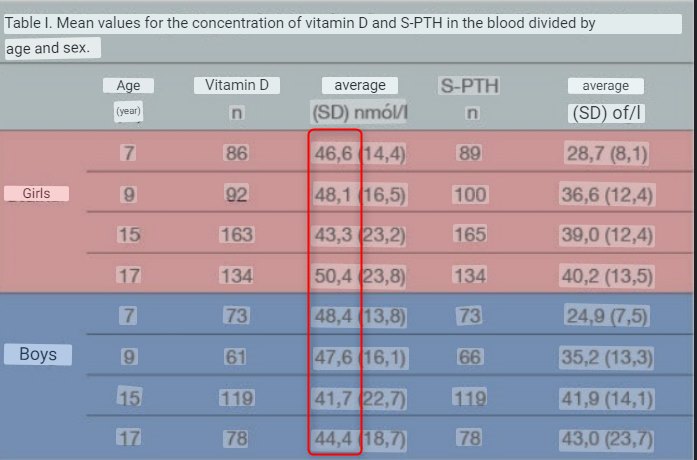
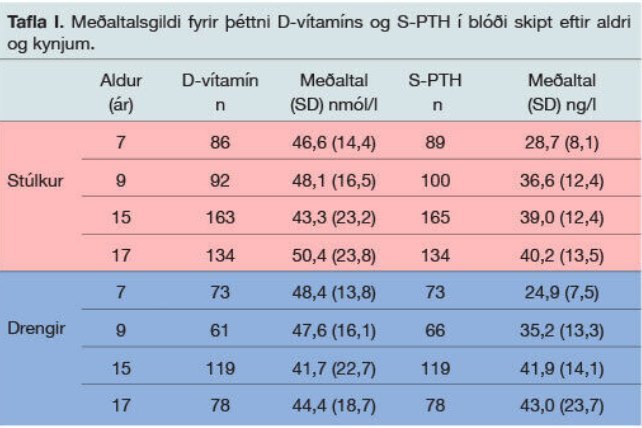
48 nmol = Vitamin D levels of Children in Iceland - 2020
Vitamin D status of Icelandic children and youth: A long-term study
Original in Icelandic
Only 13% of Icelandic children had repeated Vitamin D tests > 50 nmol May 2020
[Vitamin D status of Icelandic children and youngsters: Longitudinal study].
Gunnarsdottir B 1, Hrafnkelsson H 2, Johannsson E 3, Sigurðsson EL 4
Laeknabladid, 01 May 2020, 106(5):235-240Language:ice https://doi.org/10.17992/lbl.2020.05.579
Vitamin D plays a key role for children's growth and physical development, not only by promoting bone health but also by its influence on extraskeletal systems. The Icelandic Directorate of Health recommends a vitamin D concentration in blood of at least 50 nmol/l. The object of this study was to evaluate the vitamin D status of Icelandic children and youngsters at four different ages, and furthermore to evaluate changes in vitamin D concentrations over time and connection to parathyroid hormone status (S-PTH).
Material and methods
The subjects were students from six elementary schools in Reykjavík, born in 1999. Blood tests were taken four times, in 2006, 2008, 2015 og 2017. Some of the subjects took part in all four tests, but more students joined in 2015 and 2017.
Results
In all the tests, around 60% of the subjects had lower vitamin D concentrations than recommended by The Icelandic Directorate of Health. Only 13% met the recommended criteria of a concentration over 50 nmol/l in repeated tests and 38.9% of the subjects had lower concentrations than recommended in at least two tests. There was no significant difference between sexes except that 17 year old girls had significantly higher Vitamin D concentrations than boys (p=0.04). S-PTH was negatively correlated to vitamin D concentrations at ages 7, 15 and 17 but there was not a significant correlation at age 9. S-PTH values were lowest at age 7 and then increased with age.
Conclusion
The majority of Icelandic children and youngsters have vitamin D concentrations under the values recommended by The Icelandic Directorate of Health. In many cases, the concentrations are repeatedly too low. It is clear that there is a need for increased vitamin D intake within this group if the goal regarding recommended concentrations is to be achieved. However, the influence of vitamin D deficiency on public health is not fully known.
📄 Download the Icelandic PDF from VitaminDWiki
--
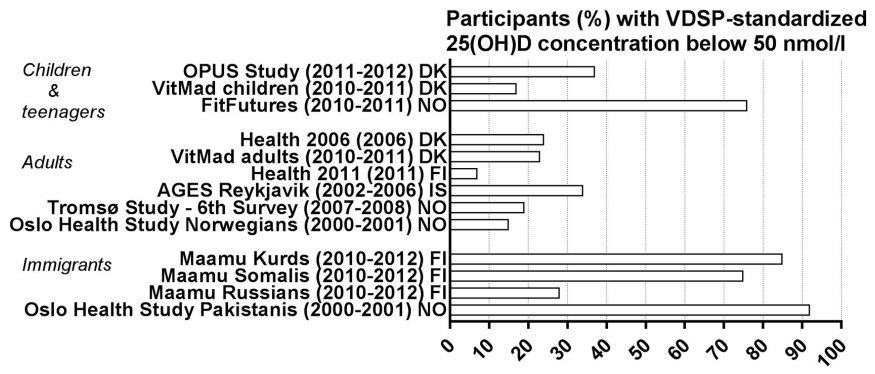
Vitamin D status and current policies to achieve adequate vitamin D intake in the Nordic countries
Volume 49, Issue 6 https://doi.org/10.1177/1403494819896878
Suvi T. Itkonen https://orcid.org/0000-0003-1635-8229 suvi.itkonen@helsinki.fi, Rikke Andersen, […], Anne K. Björk, Åsa Brugård Konde, Hanna Eneroth, Maijaliisa Erkkola, Kristin Holvik https://orcid.org/0000-0003-3132-2822, Ahmed A. Madar, Haakon E. Meyer, Inge Tetens, Jóhanna E. Torfadóttir, Birna Thórisdóttir, and Christel J.E. Lamberg-Allardt, +10 -10View all authors and affiliations
Aims: Nordic countries share fairly similar food culture and geographical location as well as common nutrition recommendations. The aim of this paper was to review the latest data on vitamin D status and intake and to describe the national supplementation and food fortification policies to achieve adequate vitamin D intake in the Nordic countries.
Methods: The data are based on results derived from a literature search presented in a workshop held in Helsinki in November 2018 and completed by recent studies.
Results: Vitamin D policies and the implementation of the recommendations differ among the Nordic countries. Vitamin D fortification policies can be mandatory or voluntary and widespread, moderate or non-existent. Vitamin D supplementation recommendations differ, ranging from all age groups being advised to take supplements to only infants. In the general adult population of the Nordic countries, vitamin D status and intake are better than in the risk groups that are not consuming vitamin D supplements or foods containing vitamin D. Non-Western immigrant populations in all Nordic countries share the problem of vitamin D insufficiency and deficiency.
Conclusions: Despite the common nutrition recommendations, there are differences between the Nordic countries in the implementation of the recommendations and policies to achieve adequate vitamin D intake and status. There is a need for wider Nordic collaboration studies as well as strategies to improve vitamin D status, especially in risk groups.
📄 Download the PDF from VitaminDWiki
Icelandic Mental Health Survey - Jan 2023
Mental health and sociodemographic characteristics among Icelanders, data from a cross-sectional study in Iceland
📄 Download the PDF from VitaminDWiki
"Participants with the most considerable financial difficulties had the highest risk of high scores on
depression RRR 11.19 (95% CI 5.8—21.57),
anxiety RRR 12.35 (95% CI 5.62—27.14) and
stress RRR 11.55 (95% CI 4.75—28.04) "
"We found that young Icelanders show more mental health problems than older Icelanders/"
Vitamin D in northern latitudes: Intake and status in Icelandic children - thesis - 2018
Title: Vitamin D in northern latitudes: Intake and status in Icelandic children
Alternative Title: D-vítamín á norðlægum slóðum: Inntaka og búskapur íslenskra barna.
Author: Þórisdóttir, Birna University/Institute: Háskóli Íslands
University of Iceland, School: Heilbrigðisvísindasvið (HÍ), School of Health Sciences (UI)
Department: Matvæla- og næringarfræðideild (HÍ), Faculty of Food Science and Nutrition (UI)
URI: https://hdl.handle.net/20.500.11815/919
Background: Adequate nutrition in childhood is essential for growth, development and health. Vitamin D supplement use is recommended in Iceland, starting in infancy. Little information exists on the vitamin D status of Icelandic infants and children. Vitamin D has been suggested to affect the development of sensitization to food allergens and food allergy. Aim: To study adherence to dietary guidelines among 6-year-old children (paper I), their vitamin D intake and vitamin D status at 12 months and 6 years (papers II and III) and compare vitamin D and feeding in infancy between 6-year-old children IgE-sensitized to food allergens and non-sensitized children (paper IV).
Methods: The study population is a nationally representative Icelandic cohort of infants born in 2005, followed up at 6 years of age. Three-day weighed food records were kept at 9 months (n=196), 12 months (n=170) and 6 years (n=162). Total vitamin D intake was calculated from both diet and supplements. Further infant nutrition data was collected by dietary history from birth to 5 months and by monthly 1-day food records at 5-8 and 10-11 months of age. Serum 25-hydroxyvitamin D (25(OH)D) was measured at 12 months (n=76) and 6 years (n=139) and serum-specific IgE-antibodies against food at 6 years (n=144). Cut-off values for vitamin D deficiency, insufficiency, sufficiency and possibly adversely high levels were set at 25(OH)D <30 nmol/L, 30-50 nmol/L, >50 nmol/L and >125 nmol/L, respectively. The cut-off value for sensitization was set at specific IgE ≥0.35 kUA/L.
Results: Adherence to dietary guidelines varied among 6-year-old children but was poor in general. A quarter, or less, of the children followed the guidelines for fruit and vegetables, fish, wholegrain bread and other fiber-rich cereals and vitamin D supplements. The food intake was mirrored in a non-optimal distribution of macronutrients, fiber and salt intake. Vitamin and mineral density of the diet seemed however adequate, except for vitamin D. Supplements (fish liver oil or liquid infant drops during the first months) were the main sources of vitamin D. Total vitamin D intake was higher at 9-12 months than at 6 years (the median intakes were 8.7 μg/d vs. 4.9 μg/d, respectively, p<0.01). The mean±SD concentration of 25(OH)D at 12 months was 98±32 nmol/L, with 92% of infants defined as having sufficient vitamin D status and none deficient. Vitamin D intake at 9-12 months, either from use of vitamin D supplements or consumption of fortified foods in significant amounts (e.g., 200 ml/d of formula), or both, was the main observed determinant for vitamin D status 12 months. Breastfeeding and season were not associated with vitamin D status at 12 months. Taking vitamin D supplements increased the risk of serum 25(OH)D at possibly adversely high levels, observed in a quarter of 12-month-old infants. At 6 years, vitamin D status was lower than in infancy (57±18 nmol/L), 30% of children were insufficient and 6% deficient. Higher total vitamin D intake at 6 years, blood samples collected in summer and higher serum 25(OH)D measured at 12 months, were associated with higher likelihood of vitamin D sufficiency at 6 years. The vitamin D status decreased during autumn in children not using vitamin D supplements. Fourteen 6-year-old children (10%) were sensitized to food allergens. Higher vitamin D intake at 12 months (OR=0.8, 95% CI=0.7-0.99) and vitamin D supplement use at 6 years (OR=0.2, 95% CI=0.1-0.98) were associated with lower risk of sensitization. Introduction of solid foods prior to four months was associated with increased risk of sensitization (OR=4.9, 95% CI=1.4-17). More weight gain and head circumference growth from 0-2 months and higher prevalence of overweight at 6 years was observed among sensitized than non-sensitized children.
Conclusions: The results indicate that a public health effort among Icelandic children is needed to increase adherence to dietary guidelines, including vitamin D supplement use. Healthy Icelandic infants and children receiving the recommended 10 µg/d vitamin D are likely to be vitamin D sufficient. Vitamin D insufficiency and deficiency may, however, be prevalent among 6-year-old children due to insufficient intake. Monitoring of diet and vitamin D status among Icelandic infants and children is important, looking both at low and high vitamin D levels. Further studies are needed on the associations of vitamin D and diet with food sensitization and allergy.
📄 Download the PDF from VitaminDWiki
Note: Thesis includes several of the author's publications
Vitamin D levels crash in Icelandic children by age 6 - Feb 2016
Vitamin D Intake and Status in 6-Year-Old Icelandic Children Followed up from Infancy
Nutrients 2016, 8(2), 75; https://doi.org/10.3390/nu8020075
by Birna Thorisdottir 1,*,Ingibjorg Gunnarsdottir 1,Laufey Steingrimsdottir 1,Gestur I. Palsson 2,Bryndis E. Birgisdottir 1 andInga Thorsdottir 1
1 Unit for Nutrition Research, Faculty of Food Science and Nutrition, School of Health Sciences, University of Iceland and Landspitali University Hospital, Reykjavik 101, Iceland
2 Children’s Hospital, Landspitali University Hospital, Reykjavik 101, Iceland
5X fewer children with > 30 ng at age 6:
Possible reasons: 1) Only give 400 IU independent of weight; 2) Cease giving Vitamin D after age 1
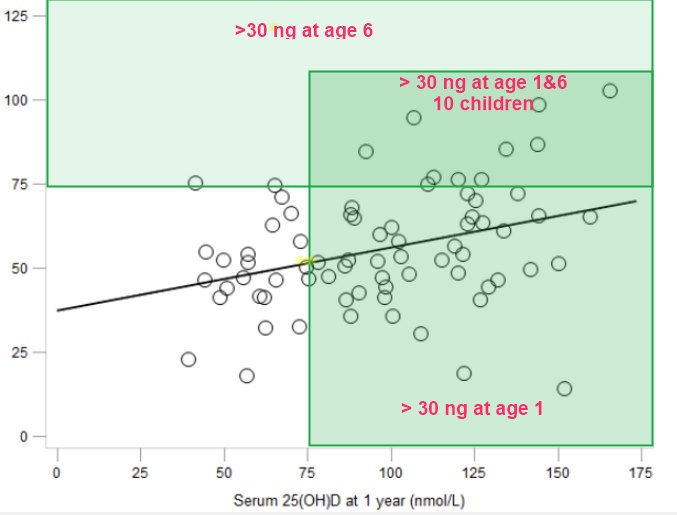
High serum 25-hydroxyvitamin D (25(OH)D) levels have been observed in infants in Nordic countries, likely due to vitamin D supplement use. Internationally, little is known about tracking vitamin D status from infancy to childhood. Following up 1-year-old infants in our national longitudinal cohort, our aims were to study vitamin D intake and status in healthy 6-year-old Icelandic children (n = 139) and to track vitamin D status from one year of age. At six years, the mean 25(OH)D level was 56.5 nmol/L (SD 17.9) and 64% of children were vitamin D sufficient (25(OH)D ≥ 50 nmol/L). A logistic regression model adjusted for gender and breastfeeding showed that higher total vitamin D intake (Odds ratio (OR) = 1.27, 95% confidence interval (CI) = 1.08–1.49), blood samples collected in summer (OR = 8.88, 95% CI = 1.83–43.23) or autumn (OR = 5.64, 95% CI = 1.16–27.32) compared to winter/spring, and 25(OH)D at age one (OR = 1.02, 95% CI = 1.002–1.04) were independently associated with vitamin D sufficiency at age six. The correlation between 25(OH)D at age one and six was 0.34 (p = 0.003). Our findings suggest that vitamin D status in infancy, current vitamin D intake and season are predictors of vitamin D status in early school-age children. Our finding of vitamin D status tracking from infancy to childhood provides motivation for further studies on tracking and its clinical significance.
📄 Download the PDF from VitaminDWiki
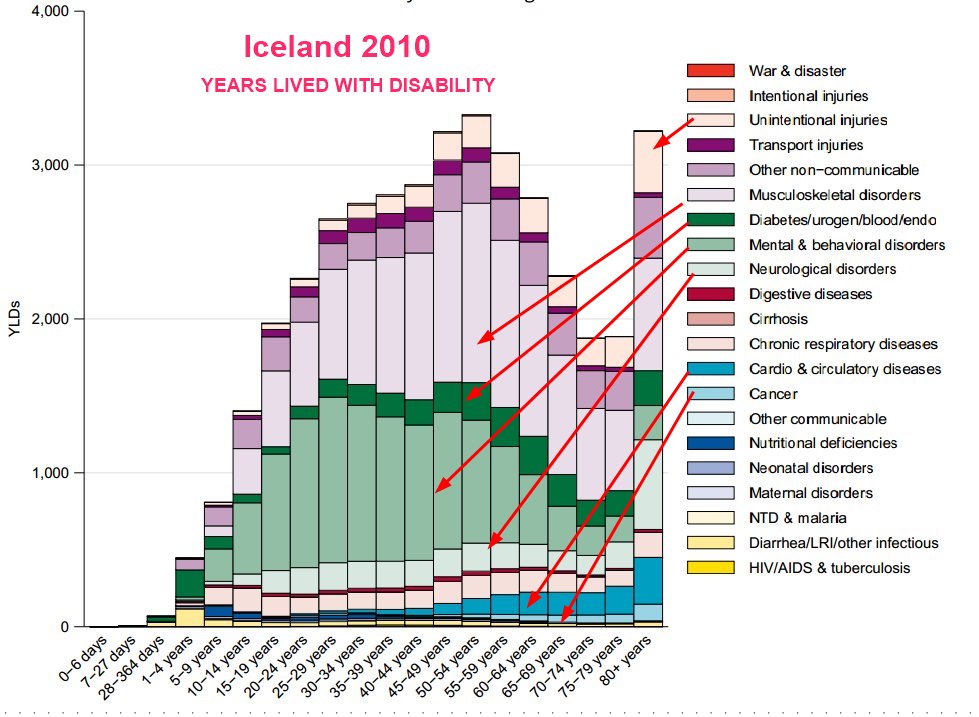
Top Icelandic disease concerns (Global Burden of Disease) - 2010
Top Icelandic disease concerns - Global Burden of Disease 2010
Top 10 causes of death in Iceland
Vitamin D intake from cod = ~400 IU daily average - not nearly enough for aduls
100 IU of vitamin D per ounce of cod
assume 50 kg of cod consumed per year (Icelanders consume 92 kg of fish/year
Daily consumption of cod = 140 grams/day = 140 grams/day * 1 ounce/30 grams = 4 ounces/day
Omega-3 intake from cod = ~300 mg/day
Cod contains 221 milligrams of omega-3 fatty acids per 100 grams,
Assume 50 kg of cod consumed per year (Icelanders consume 92 kg of fish/year
Omega-3 Reduces risk of Breast Cancer - many studies sometimes reduced by a larger amount than by Vitamin D
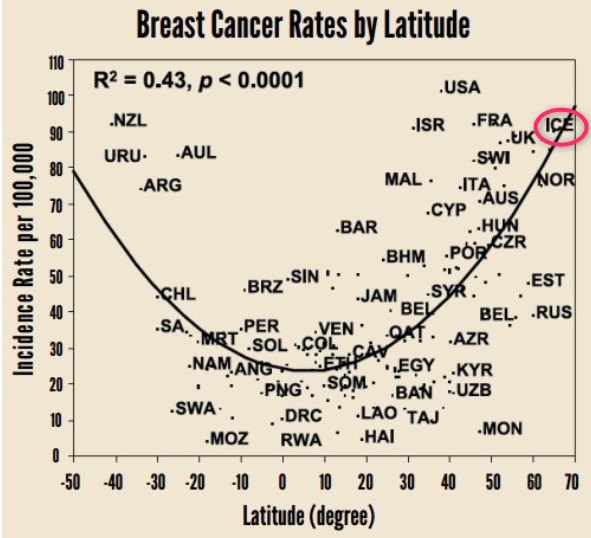
VitaminDWiki - Many diseases increase with latitude (low UV, Vitamin D) charts with Iceland
Breast Cancer
Lung Cancer
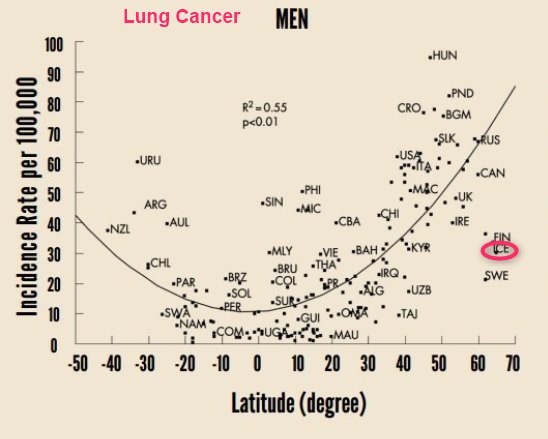
See also VitaminDWiki
Sun holidays are an important, but expensive, source of vitamin D in Sweden - Sept 2013
Eating Fish – 17 health benefits (Omega-3 and perhaps Vitamin D) – umbrella review Feb 2023
Many autoimmune diseases associated with latitude and vitamin D receptor – March 2016
Shift work associated with lower Vitamin D in 12 of 13 studies – meta-analysis July 2022
Employers should give night shift workers free vitamin D – GMB Union June 2019
Increased incidence of 7 cancers if live far from equator (if not take vitamin D) – March 2019
Does Less Sun mean More Disease 5 minute video
Vitamin D levels in Alaska are decreasing – does less fish mean less health – Aug 2017
One pill every two weeks gives you all the vitamin D most adults need
32 publications with (vitamin D keyword or Reykjavik) by Icelandic authors as of Oct 2023
Changes in vitamin D metabolites at the time of critical illness and 6 months later-A prospective observational study - Aug 2022 https://doi.org/10.1111/aas.14137 Reykjavik
Vitamin D status and its correlation to depression - Aug 2022 https://doi.org/10.1186/s12991-022-00406-1 FREE PDF
[Centenary of vitamin-D] July 2022 https://doi.org/10.17992/lbl.2022.0708.697 FREE PDF in Icelandic
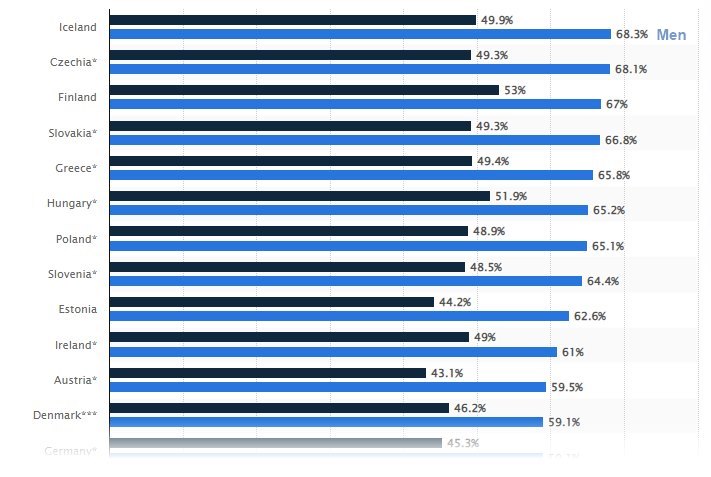
2 out of 3 Icelandic men are overweight or obese (highest rate in Europe)
Statistica 2022
Overview Obesity and Vitamin D contains the following summary
{include}
{include}
10,200 Iceland and Vitamin D articles in Google Scholar as of Sept 2023
Characteristics of hip fractures cases among community-dwelling Icelandic older adults - June 2022 https://hdl.handle.net/20.500.11815/3294 FREE PDF
Serum Vitamin D and Parathyroid Hormone in Relation to Cardiac Structure and Function: The ICELAND-MI Substudy of AGES-Reykjavik - June 2013 https://doi.org/10.1210/jc.2012-4252 FREE PDF
Vitamin D deficiency and nutritional status in elderly hospitalized subjects in Iceland - July 2009 https://doi.org/10.1017/S1368980008004527 FREE PDF
[Vitamin-D homeostasis amongst adult Icelandic population.]. Jan 2004,in Icelandic
Chronic pain in Iceland
Multidisciplinary Pain Rehabilitation Programs in Iceland: An Exploration and Description of the Short-term and Long-term Effects - Feb 2022
📄 Download the Nursing PHD from VitaminDWiki
A population based study of the prevalence of pain in Iceland - 2010
Prevalence estimates of pain differ depending on how it is defined and measured and on the populations studied. It has been estimated that on a given day, as many as 30–44% of the general population experience some kind of pain. Information about the prevalence of pain in Iceland is not available.
The aims of this study were to evaluate the prevalence of pain of various origins among the general population of Iceland, to test hypotheses regarding relationships between pain, quality of life (QOL) and demographic variables, to evaluate participants’ beliefs about causes of their pain, and to evaluate how those who experience pain manage it. A random sample of 1286 adults was drawn from a national registry holding information about all citizens of Iceland. Data were collected with a postal-survey. Pain was evaluated with the Brief Pain Inventory (BPI), with instructions modified to evaluate pain in the past week as opposed to the past 24 h. Of 1286 invited, 599 (46.6%) participated, of which, 232 had experienced pain in the past week (40.3%). Participants had a mean (SD) age of 44.94 (17.12) years and 56% were women. Those who had pain perceived their health to be worse than those who had not [B = −0.91, SE = 0.15, Wald = 38.75, p = 0.00], but did not differ on other variables. Of 232 individuals reporting pain, 183 (79.6%) or 30.6% of the total sample had experienced pain for more than three months. On a scale from 0 “no pain” to 10 “pain as bad as I can imagine” the mean (SD) pain severity score (composite of four pain severity scores) for the 232 participants reporting pain was 3.21 (1.73) and pain interference with life activities 2.59 (1.98), also on a 0–10 scale. Pain severity predicted pain interference [B = 0.71; F = 126.14; df = 1,206; p = 0.00], which mediated the effects of pain severity on mood and QOL. Between Pain Interference with Life and Positive Affect [B = −0.06; F = 4.53; df = 1,196; p = 0.04], between Pain Interference and Negative Affect [B = 0.15; F = 23.21; df = 1,196; p = 0.00], and between Pain Interference and Global Quality of Life [B = −0.18; F = 29.11; df = 1,196; p = 0.00].
Most frequent causes for pain were
strain injuries (n = 79),
resulting from work or sports activity, arthritis (n = 39),
mechanical problems (e.g. due to birth defects, curvature, slipped discs, etc.) (n = 37),
various diseases (n = 31) and accidents (n = 30).
Nineteen participants did not know what caused their pain. Treatments for pain varied, but most had used medications alone (n = 76) or in combination with other treatments (n = 61). The prevalence of pain in the general population of Icelandic adults is similar to what has been reported. Estimates of chronic pain are towards the higher end when compared to data from other European counties, yet comparable to countries such as Norway. This raises questions about possible explanations to be looked for in genetics or cultural point of view. This population-based study provides valuable information about the prevalence of pain in Iceland and also supports findings previously reported about pain in the neighboring countries.
📄 Download the PHD from VitaminDWiki
Whether the weather influences pain: High prevalence of chronic pain in Iceland and Norway: Common genes? Or lack of sunshine and vitamin D? - 2010
Prevalence chronic pain 31% in Iceland vs 12% in Spain
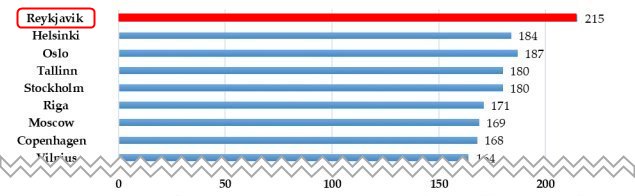
Does less sun mean more disease? 215 days of winter in Iceland (No vitamin D from the sun)
Does Less Sun mean More Disease 5 minute video
COVID and Iceland
Vaccine could have tripled Iceland’s Covid death rate - Nov 2023
Seems to ignore Excess deaths
NOW that the numbers are in, the Icelandic Chief Medical Officer (CMO) claims vaccination against Covid-19 reduced the probability of death from the disease by half, compared with no vaccination. But the actual figures tell a very different story, and the method used to arrive at this conclusion is questionable to say the least. The actual reduction in deaths is negligible at best, and the most worrying result is how those fully vaccinated (two doses) were almost three times more likely to die from the disease than the unvaccinated.
In summary,
only 20 lives were potentially saved in Iceland by Covid-19 vaccination,
while 60-70 may have been lost to the disease in the vaccinated.
When we take into account the number of deaths reported following vaccination, the overall result of the experiment is likely to be negative.
📄 Download the English PDF from VitaminDWiki
📄 Download the Icelandic translated PDF from VitaminDWiki
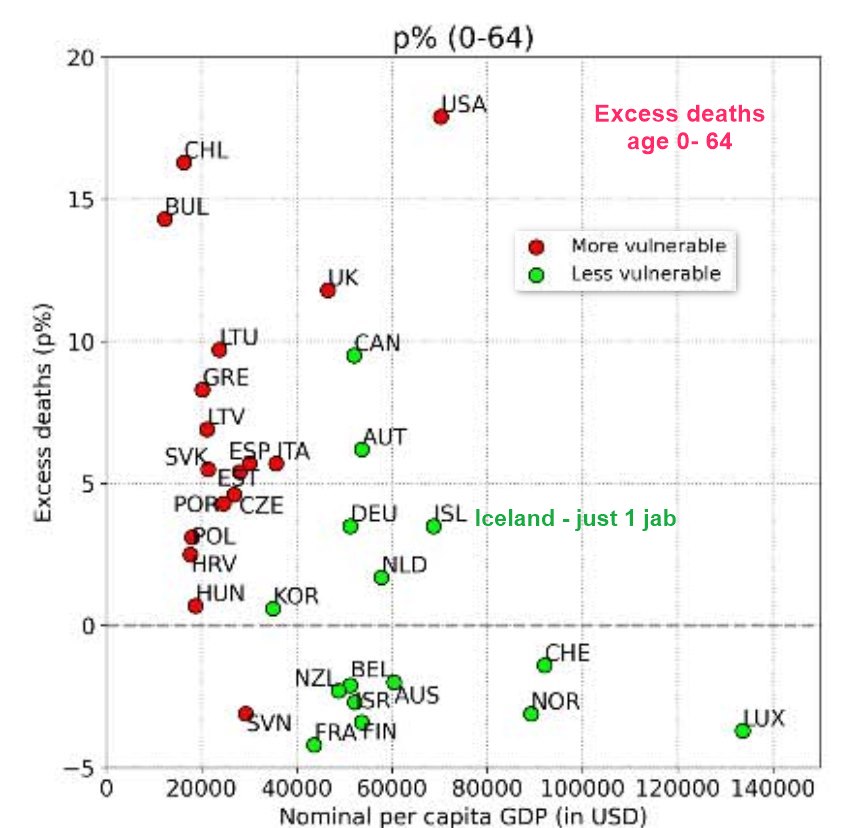
4% Excess deaths in Iceland for ages 0-64 (due to COVID vaccine) - Aug 2023
Excess deaths in 34 countries (probably due to COVID vaccination) – preprint Aug 2023
There have been visits to this page
SHORT URL = https://is.gd/vitdice