Chronic Kidney Disease (stage 3) slowed by 30 ng of Vitamin D and Calcitriol
Effectiveness of Native Vitamin D Therapy in Patients with Chronic Kidney Disease Stage 3 and Hypovitaminosis D in Colombia, South America
International Journal of Nephrology and Renovascular Disease » Volume 12 Pages 241—250, DOI https://doi.org/10.2147/IJNRD.S214194
 Click on chart for details
---
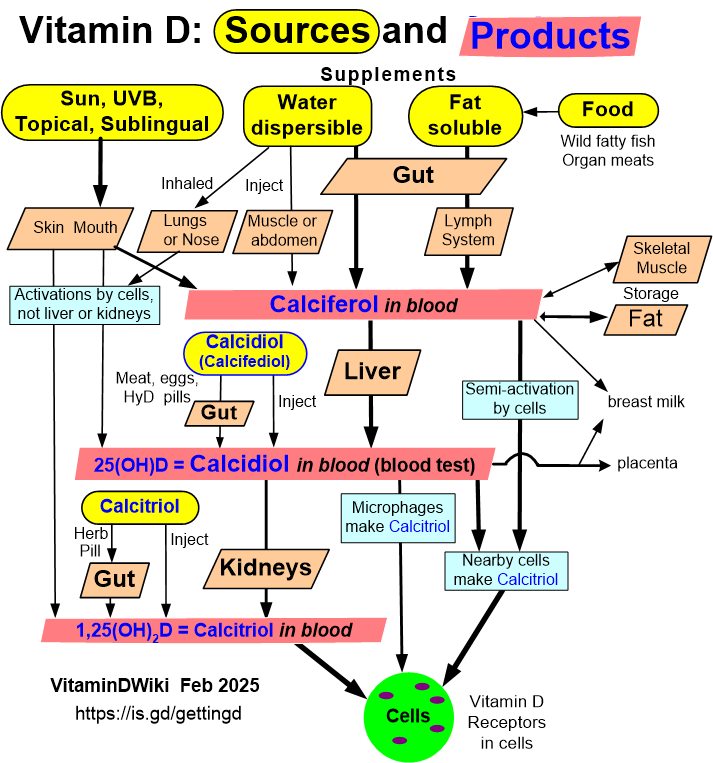
1. Overview Kidney and vitamin D contains the following summary
{include}
Click on chart for details
---
1. Overview Kidney and vitamin D contains the following summary
{include}
📄 Download the PDF from VitaminDWiki
Cesar A Restrepo-Valencia,1 Jose V Aguirre-Arango,2 Carlos G Musso3
1 Professor Titular, Universidad de Caldas, Manizales, Colombia; caugustorv@une.net.co
2 Professor Catedratico, Universidad de Manizales, Manizales, Colombia;
3 Facultad de Ciencias de la Salud, Universidad Simón Bolívar, Barranquilla, Colombia
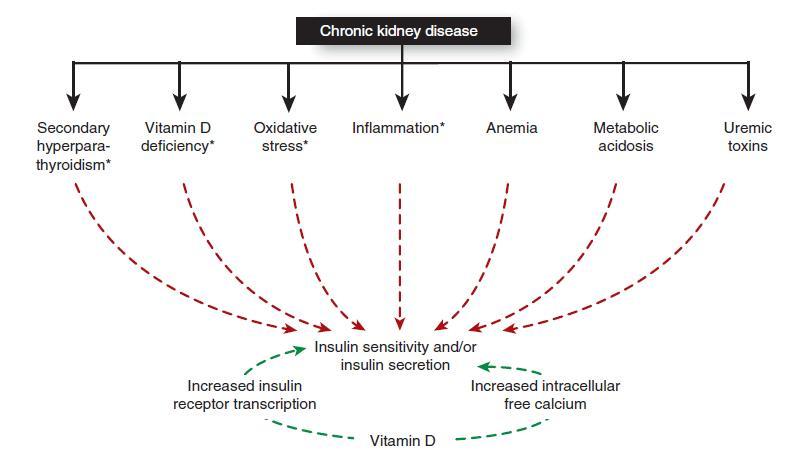
Introduction: In a high percentage of patients with chronic kidney disease (CKD) low levels of vitamin D are detected. The purpose of this study was to evaluate if the native vitamin D therapy (cholecalciferol) in the patients with stage 3 and hypovitaminosis D allows to modify markers of bone and mineral metabolism once normal serum levels have been achieved.
Materials and methods: From an initial base of 297 patients with CKD and hypovitaminosis D, those with normal or high levels of PTH were chosen for therapy with native vitamin D. The initial administered dose was 1000 IU/day, with adjustments every 4 months of 1000 IU (maximum 4000 IU/day, according to RDA and IOM), until achieving serum levels of 25 hydroxyvitamin D greater than 30 ng/mL and lower than 80 ng/mL. The variables calcium, phosphorus, intact parathormone (iPTH), creatinine and glomerular filtration rate (GFR) were also evaluated every 4 months.
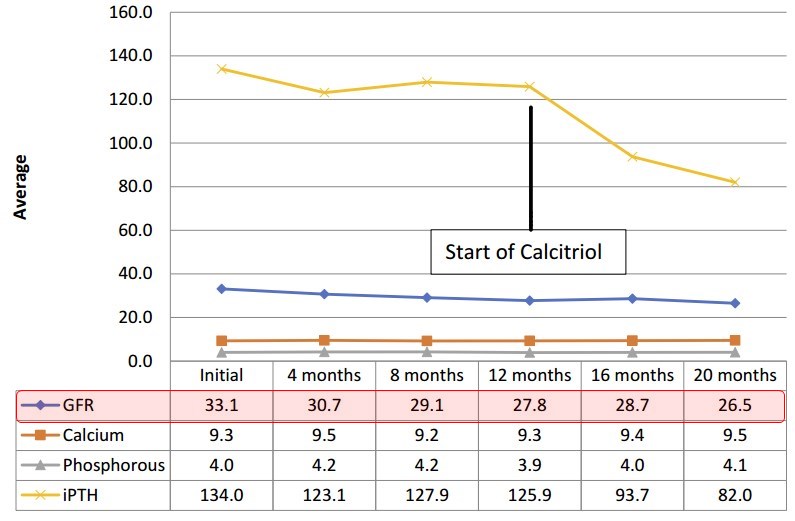
Results: The total number of patients included in this study was 170. Seventy-three patients were excluded along the follow-up: 17 non-responders (never achieved the projected serum levels of vitamin D), and 56 for not completing one year of follow-up. A total of 97 patients were finally included. In 82 patients, follow-up was achieved for 12 months (G1) and in 38 patients for 24 months (G2). In 15 patients despite achieving satisfactory levels of vitamin D at 12 months, it was not possible to obtain adequate levels of iPTH for their GFR according to K/DOQI 2003 guidelines and they were called refractory to therapy (G3). In both groups 1 and 2, a non-significant tendency to increase calcium and serum phosphorus was observed. iPTH decreased significantly at 12 and 24 months follow-up. In group 3, we opted at 12 months for conversion to calcitriol, with a significant reduction in iPTH values. In this group, the initial value of GFR was close to 30 mL/min, and its fall in time more significant than the other two groups to CKD stage 4.
Conclusion: Cholecalciferol with adjustment in its dose, and obtaining normal serum levels is an excellent therapeutic alternative for the treatment of patients with CKD stage 3, and hypovitaminosis D. In the group of patients with GFR close to 30 mL/min, or lower values (stage 4), and with the presence of secondary hyperparathyroidism, the use of active form of vitamin D (calcitriol, paricalcitol) is recommended as the first therapeutic alternative.