Vitamin D loading dose of 300,000 IU for children – 3 weeks with capsules, biscuits, injection – RCT
Stoss therapy using fortified biscuit for vitamin D-deficient children: a novel treatment
Pediatric Research (2018) 10.1038/s41390-018-0135-4
Leila Moslemi, Mohammadreza Esmaeili dooki, Ali Akbar Moghadamnia, Morteza Alijanpour Aghamaleki, Mohammad Pornasrollah, Hassan Ashrafianamiri, Haji-Ghorban Nooreddini, Sohrab Kazemi, Mahdi Pouramir & Ali Bijani
2/week 3 weeks | Capsule
2/week 3 weeks | Injection
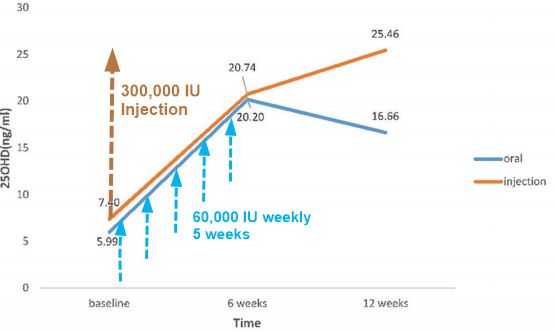
1 time | | Measured at 3 weeks | 42 ng | 50 ng | 63 ng | | VitaminDWiki guess at 10 weeks | 35 ng | 40 ng | 80 ng | 1. Overview Loading of vitamin D contains the following {include} --- Injection category listing has items along with related searches Infant-Child category listing has items along with related searches Fortification with Vitamin D category listing has items along with related searches * Vitamin D injection lasts longer and has bigger response than weekly oral – Jan 2017 has the following *
PDF is available free at Sci-Hub 10.1038/s41390-018-0135-4
Background: To evaluate the efficacy of stoss therapy using fortified biscuit for vitamin D-deficient children.
Methods
A total of 108 children aged 30–72 months with vitamin D deficiency were studied in a randomized single-blind clinical trial. The deficient children were assigned to three groups, namely, vitamin D-fortified biscuit (BG), capsule vitamin D (CG), and ampoule vitamin D (AG). Capsules and biscuits containing 50,000 IU of cholecalciferol were consumed twice per week for 3 consecutive weeks. Ampoules with 300,000 IU of cholecalciferol were injected intramuscularly in a single dose. Three weeks after treatment, serum 25(OH)D concentrations were measured, and the three groups were compared.
Results
Each method of treatment could increase the mean serum 25(OH)D concentration to optimal level. Serum 25(OH)D concentrations ≥100 ng/mL were observed in six children, including four from AG and two from CG (P = 0.09). The comparison of the mean serum 25(OH)D concentrations after treatment showed between ampoule and capsule (P = 0.3) and capsule and biscuit (P = 0.62) were insignificant; however, the ampoule and biscuit groups differed significantly (P = 0.012).
Conclusion
Stoss therapy using fortified biscuit may be an effective way to improve compliance in children who cannot take capsules without adverse effects and may also be recommended for prevention purposes.