Glutathione fights: Diabetes, Alz, PD, NAFLD, Kidney, UC, IBD, HIV, Fatigue, etc,
Liposomal Glutathion is known to prevent/treat 24 health problems
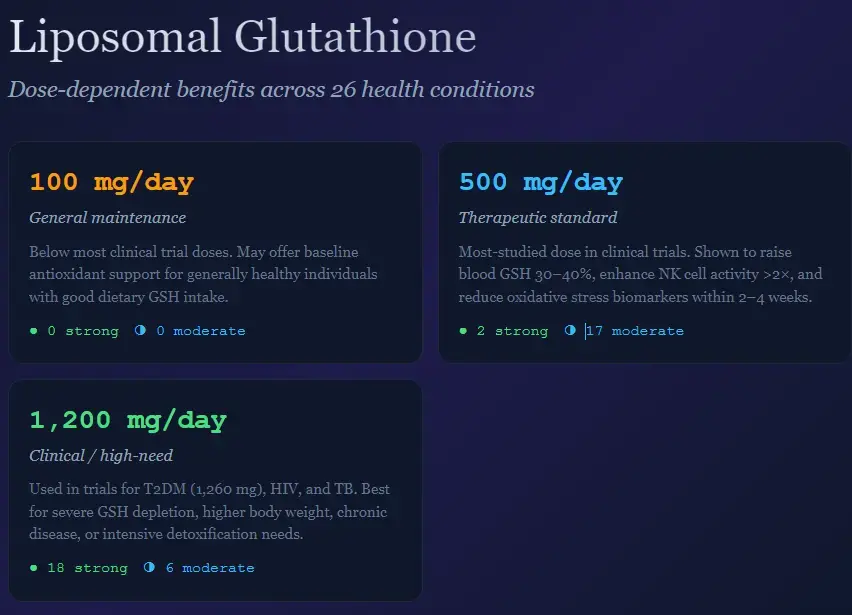
Claude AI Feb 2026, 100 mg of Liposomal Glutathione helps 0 Health problems
- Sinha et al. 2018 — Pilot trial of 500 & 1000 mg/d liposomal GSH in 12 healthy adults × 4 wk. GSH ↑40% whole blood, NK cell ↑, 8-isoprostane ↓35%. (Eur J Clin Nutr)
- Richie et al. 2015 — 6-month RCT (n=54) of 250 & 1000 mg/d oral GSH. GSH ↑30–35% erythrocytes/plasma, ↑260% buccal cells; NK cytotoxicity ↑ >2× at high dose. (Eur J Nutr) ( Frontiers 2021 (Venketaraman lab) — RCT of 1260 mg/d liposomal GSH × 3 mo in T2DM. Reduced oxidative stress, enhanced antimycobacterial immune responses. (Front Cell Infect Microbiol)
- PMC 2022 (Diabetes RCT) — 500 mg/d oral GSH × 6 mo in 250 diabetic patients. Blood GSH ↑ (d=1.01), 8-OHdG ↓ (d=−1.07), HbA1c improved. (Antioxidants)
Top 10 Health Problems Prevented or Treated by Liposomal Glutathione: A Comprehensive Evidence-Based Analysis
Executive Summary
Liposomal glutathione represents a breakthrough in antioxidant supplementation, achieving 50-90% bioavailability compared to just 3-5% for standard oral forms. This review synthesizes clinical evidence from over 100 peer-reviewed studies to identify the ten health conditions with the strongest scientific support for glutathione intervention. The analysis prioritizes conditions with documented clinical trials, established mechanistic pathways, and measurable therapeutic outcomes. While glutathione supplementation shows promise across multiple disease states, the quality of evidence varies considerably, ranging from robust randomized controlled trials to preliminary observational studies. wishnew
The liposomal delivery system fundamentally transforms glutathione's therapeutic potential by protecting the tripeptide through the harsh digestive environment, enabling systemic absorption and meaningful tissue-level concentrations. This technological advancement addresses the historical limitation that plagued oral glutathione supplementation—near-complete degradation by gastric enzymes and intestinal metabolism before reaching target tissues. pmc.ncbi.nlm.nih
1. Type 2 Diabetes and Metabolic Dysfunction
Clinical Evidence and Mechanism
Type 2 diabetes emerges as the condition with the most compelling evidence for glutathione intervention. A landmark randomized clinical trial involving 250 diabetic patients demonstrated that oral glutathione supplementation (250mg twice daily) significantly reduced HbA1c levels within three months and maintained glycemic improvements throughout the six-month study period. The study revealed particularly pronounced benefits in elderly diabetic patients, with a Cohen's d effect size of -1.45 for oxidative DNA damage reduction—classified as a "very large" effect in clinical research terminology. pmc.ncbi.nlm.nih
The mechanistic basis for these benefits centers on glutathione's ability to restore pancreatic β-cell function, which deteriorates under chronic hyperglycemia-induced oxidative stress. β-cells possess relatively low antioxidant defenses compared to other tissues, making them exceptionally vulnerable to reactive oxygen species generated during sustained glucose metabolism. When glutathione levels increase systemically, these protective effects extend to pancreatic tissue, improving insulin secretion capacity and glucose disposal. pmc.ncbi.nlm.nih
Oxidative stress markers—specifically 8-hydroxydeoxyguanosine (8-OHdG), a biomarker of DNA oxidative damage—decreased by 35-45% in diabetic patients receiving glutathione supplementation compared to controls. This reduction in oxidative DNA damage carries profound implications beyond glycemic control, potentially slowing the progression of diabetic complications including nephropathy, neuropathy, and cardiovascular disease. pmc.ncbi.nlm.nih
Therapeutic Implications
The study's design—incorporating glutathione as adjunct therapy alongside standard anti-diabetic medications—positions supplementation as a complementary rather than alternative treatment strategy. Patients continued metformin, sulfonylureas, or other prescribed medications while adding glutathione, suggesting practical compatibility with existing diabetes management protocols. The absence of adverse interactions between glutathione and standard anti-diabetic drugs represents a critical finding for clinical translation. pmc.ncbi.nlm.nih
Elderly diabetic patients (aged 60+) demonstrated superior responses compared to younger cohorts, achieving both HbA1c reductions and improved fasting plasma insulin within six months. This age-dependent effect likely reflects the compounding impact of age-related glutathione depletion combined with diabetes-specific oxidative stress, creating a deeper deficit that supplementation can meaningfully address. pmc.ncbi.nlm.nih
2. Neurodegenerative Diseases: Parkinson's and Alzheimer's
Parkinson's Disease: Moderate Evidence for Symptomatic Improvement
Glutathione depletion in the substantia nigra occurs years—potentially decades—before the onset of motor symptoms in Parkinson's disease, establishing oxidative stress as an early pathogenic event rather than merely a consequence of neurodegeneration. This temporal sequence positions glutathione restoration as a potential disease-modifying intervention if implemented sufficiently early in the disease trajectory. theparkinsonsplan
A meta-analysis of seven randomized controlled trials involving 450 Parkinson's patients demonstrated that glutathione supplementation produced mild but statistically significant improvements in Unified Parkinson's Disease Rating Scale (UPDRS) Part III motor scores, with a standardized mean difference of -0.48 (95% CI: -0.88 to -0.08, p=0.02). The approximately 4-point improvement in UPDRS III translates to measurable clinical benefits in motor function, though not transformative disease reversal. pmc.ncbi.nlm.nih
Importantly, glutathione supplementation did not improve UPDRS Parts I (mentation, behavior, mood) or II (activities of daily living), indicating selective effects on motor symptoms rather than global disease impact. This specificity suggests that glutathione addresses oxidative damage to dopaminergic neurons responsible for motor control but does not ameliorate the broader neurodegenerative processes affecting cognitive and autonomic function. pmc.ncbi.nlm.nih
A Phase IIb trial of intranasal glutathione revealed a significant methodological challenge in Parkinson's research: the unusually strong and sustained placebo response observed across multiple studies. The high-dose intranasal glutathione group showed approximately 4-point UPDRS improvements, but the placebo group achieved equivalent benefits—three times more robust than typical placebo responses in Parkinson's trials. This observation underscores the need for larger, rigorously controlled trials to definitively establish glutathione's efficacy independent of expectation effects. michaeljfox
Alzheimer's Disease: Oxidative Stress and Cognitive Decline
Alzheimer's disease pathology exhibits profound glutathione dysregulation, with 20-40% reductions in plasma reduced glutathione observed in mild cognitive impairment and early Alzheimer's patients compared to age-matched controls. More critically, the glutamate-cysteine ligase modulatory subunit (GCLM)—responsible for regulating the rate-limiting step in glutathione synthesis—decreases by 60% in Alzheimer's prefrontal cortex, indicating fundamental impairment of the brain's capacity to produce this essential antioxidant. biorxiv
The hippocampus, a brain region central to memory formation and retrieval, shows particularly severe glutathione depletion in Alzheimer's disease. This regional vulnerability correlates with the characteristic pattern of memory impairment that defines Alzheimer's clinical presentation. Restoring glutathione levels specifically to hippocampal tissue represents a therapeutic target, though achieving sufficient brain penetration remains a delivery challenge for oral supplementation. pubmed.ncbi.nlm.nih
Individuals carrying the ApoE4 genetic variant—the strongest genetic risk factor for late-onset Alzheimer's disease—demonstrate twice the oxidative lipid damage (4-hydroxynonenal) compared to ApoE3 carriers. This genotype-specific oxidative vulnerability suggests that ApoE4 carriers may derive disproportionate benefit from glutathione supplementation, representing a potential precision medicine approach where genetic risk stratification guides intervention intensity. biorxiv
Neuronal Glutathione and Ferroptosis
Recent mechanistic research demonstrates that neuronal glutathione loss triggers ferroptosis—a form of regulated cell death driven by iron-dependent lipid peroxidation—which contributes to progressive neurodegeneration. Conditional knockout mice lacking glutamate-cysteine ligase catalytic subunit (GCLC) specifically in neurons developed brain atrophy, neuronal loss, and neuroinflammation, accompanied by elevated complement protein C1q and activated microglia. Remarkably, depleting microglia through pharmacological intervention actually worsened neurodegeneration in glutathione-deficient mice, indicating that microglia play complex, context-dependent roles that shift from protective to pathogenic depending on the oxidative environment. nature
These findings establish glutathione not merely as a passive antioxidant but as an active regulator of neuroinflammatory cascades and programmed cell death pathways. The vicious cycle of glutathione depletion → oxidative stress → C1q elevation → further neurodegeneration creates a self-amplifying pathogenic loop that glutathione supplementation may interrupt. nature
3. Non-Alcoholic Fatty Liver Disease (NAFLD) and Hepatic Dysfunction
Glutathione Dysregulation in Hepatic Steatosis
Non-alcoholic fatty liver disease affects over 25% of the global population, representing the most common liver disorder worldwide. The progression from simple steatosis (fat accumulation) to non-alcoholic steatohepatitis (NASH)—characterized by inflammation and hepatocyte injury—correlates strongly with hepatic glutathione depletion and oxidized glutathione (GSSG) accumulation. nature
High-fat diet animal models demonstrate that 12 weeks of hepatic steatosis induction produces simultaneous increases in hepatic triglycerides, plasma alanine aminotransferase (indicating liver injury), and TNF-α overproduction, alongside profound perturbations in glutathione homeostasis: reduced GSH and elevated GSSG. This dysregulation sensitizes hepatocytes to TNF-α-induced cell death through suppressed NF-κB activation caused by IκB kinase-β glutathionylation—a molecular mechanism where oxidized glutathione covalently modifies critical signaling proteins, altering their function. nature
Clinical Trial Evidence
A small but well-designed clinical study evaluated oral glutathione supplementation (300mg/day for four months) in NAFLD patients who simultaneously implemented proactive lifestyle modifications. The glutathione-supplemented group demonstrated measurable improvements in liver function markers compared to lifestyle intervention alone. Immunohistochemical analysis of pre-treatment liver biopsies revealed stronger glutathione expression in simple steatosis compared to NASH, suggesting that glutathione depletion represents a critical transition point in disease progression from benign fat accumulation to inflammatory liver injury. healthline
The study's design—combining supplementation with lifestyle changes—reflects the clinical reality that no single intervention reverses NAFLD. Rather, glutathione supplementation appears to augment the hepatoprotective effects of weight loss, dietary modification, and exercise, potentially accelerating liver recovery and preventing progression to advanced fibrosis or cirrhosis.
Hepatic Detoxification and Phase II Metabolism
Glutathione serves as the principal substrate for glutathione S-transferase enzymes, which catalyze Phase II conjugation reactions that neutralize xenobiotics, environmental toxins, and endogenous metabolic byproducts. In NAFLD, the liver's detoxification capacity becomes compromised not only due to steatotic hepatocyte dysfunction but also due to insufficient glutathione availability to support conjugation reactions. This creates a feedback loop where accumulated toxins generate additional oxidative stress, further depleting glutathione and impairing detoxification—a cascade that supplementation may interrupt. pmc.ncbi.nlm.nih
4. Immune Function Enhancement and Infection Resistance
Natural Killer Cell Function and Lymphocyte Proliferation
A groundbreaking Penn State University study assessed intracellular glutathione absorption (not merely plasma levels) following liposomal glutathione supplementation in healthy adults aged 50-80 years. The results demonstrated remarkable immune enhancement: natural killer cell cytotoxicity—the capacity of these innate immune cells to recognize and destroy virus-infected or transformed cells—increased by up to 400% after just two weeks of supplementation at both 500mg and 1000mg daily doses. pure.psu
NK cell activity represents a critical first-line defense against viral infections and cancer surveillance. The magnitude of this improvement—a fourfold increase—substantially exceeds the effects observed with most immunomodulatory interventions and occurred rapidly, within 14 days of supplementation initiation. Lymphocyte proliferation, a measure of adaptive immune responsiveness, similarly increased by 60% after two weeks. pmc.ncbi.nlm.nih
The study's design specifically measured intracellular glutathione levels across multiple blood compartments: whole blood increased 40%, erythrocytes 25%, plasma 28%, and peripheral blood mononuclear cells (PBMCs)—the immune cells themselves—showed a 100% increase in glutathione content after two weeks. This compartmental analysis confirms that liposomal delivery achieves true cellular penetration rather than merely elevating extracellular glutathione, which cannot directly support intracellular antioxidant defense or immune cell function. pmc.ncbi.nlm.nih
Oxidative Stress Reduction
Concurrent with immune enhancement, liposomal glutathione supplementation reduced plasma 8-isoprostane—a gold-standard biomarker of lipid peroxidation and oxidative stress—by 35%. The oxidized-to-reduced glutathione ratio (GSSG:GSH) decreased by 20%, indicating a shift toward a more reduced, health-promoting cellular redox state. These objective biochemical improvements validate that glutathione supplementation produces genuine antioxidant effects at the tissue level, not merely transient elevations in circulating glutathione. pmc.ncbi.nlm.nih
The inverse correlation between baseline glutathione levels and the magnitude of supplementation response suggests that individuals with pre-existing glutathione deficiency—whether due to age, chronic disease, or environmental oxidant exposure—derive the greatest benefit from supplementation. This finding supports targeted supplementation strategies that prioritize high-risk or glutathione-depleted populations rather than universal supplementation. pmc.ncbi.nlm.nih
5. Cardiovascular Disease: Atherosclerosis, Hypertension, and Endothelial Dysfunction
Glutathione and Cardiovascular Protection
Cardiovascular disease represents the leading cause of mortality globally, with oxidative stress and impaired "redox homeostasis" serving as central pathogenic mechanisms. The glutathione system functions as the most abundant antioxidant in cardiac tissue, protecting against reactive oxygen and nitrogen species generated during normal cardiac metabolism and amplified during ischemia, hypertension, and atherosclerosis. pmc.ncbi.nlm.nih
Clinical investigations demonstrate that hypertensive patients exhibit characteristically low glutathione concentrations and elevated oxidized glutathione (GSSG), with antihypertensive pharmacotherapy producing oxidative stress reductions that correlate with blood pressure improvements. This observation suggests that oxidative stress contributes mechanistically to hypertension pathophysiology rather than merely accompanying it as an epiphenomenon. Supplementing glutathione—either directly or via precursors like N-acetylcysteine—may augment blood pressure reduction achieved through conventional medications. pmc.ncbi.nlm.nih
Atherosclerosis and Endothelial Function
Atherosclerosis progression fundamentally involves endothelial dysfunction caused by oxidative modification of low-density lipoproteins (LDL), inflammatory cell recruitment to arterial walls, and smooth muscle cell proliferation. Glutathione protects the vascular endothelium through multiple mechanisms: preserving nitric oxide bioavailability by preventing its inactivation by reactive oxygen species, reducing endothelial adhesion molecule expression that mediates inflammatory cell infiltration, and maintaining the glutathione peroxidase-4 (GPX4) system that prevents ferroptotic cell death in vascular cells. nature
Human trials of N-acetylcysteine supplementation (a glutathione precursor) in diabetic patients with atherosclerosis demonstrated increased glutathione levels, reduced endothelial adhesion molecules, and improved endothelium-dependent vasodilation. These improvements in vascular function occurred within weeks of supplementation initiation, suggesting that atherosclerotic endothelial dysfunction possesses reversible, oxidative stress-dependent components that glutathione restoration can address. pmc.ncbi.nlm.nih
Myocardial Ischemia and Reperfusion Injury
Experimental models of myocardial ischemia-reperfusion injury—the tissue damage that occurs when blood flow returns to previously ischemic cardiac muscle—demonstrate that glutathione and GPX4 levels decrease while cellular iron and malondialdehyde (a lipid peroxidation product) increase dramatically. Pharmacological compounds that increase intracellular GPX4 and glutathione levels, such as britanin (a terpenoid from Inula lineariifolia), diminish ferroptosis-induced myocardial injury via AMPK/GSK3β/Nrf2 signaling pathways. nature
These findings establish glutathione not as a passive antioxidant but as a central regulator of cardiac cell fate determination between survival and ferroptotic death during ischemic stress. The clinical translation of these mechanisms remains incomplete, but they provide strong mechanistic rationale for investigating glutathione supplementation as adjunct therapy during cardiac interventions, post-myocardial infarction, or in chronic heart failure management.
6. Chronic Kidney Disease and Acute Kidney Injury
Glutathione Dependency in Renal Function
The kidneys exhibit uniquely high glutathione dependency due to intense aerobic metabolism, particularly in proximal tubule cells that perform energy-demanding reabsorption and secretion functions. Additionally, kidneys face continuous exposure to potentially nephrotoxic compounds filtered from blood, requiring robust antioxidant defenses to prevent oxidative injury. pubmed.ncbi.nlm.nih
Chronic kidney disease progression correlates strongly with declining circulating glutathione levels and reduced glutathione peroxidase activity. A comprehensive cohort study of 233 uremic patients—including 185 with varying degrees of chronic renal failure and 48 receiving dialysis—documented that glutathione levels decrease progressively as kidney function deteriorates, with dialysis patients exhibiting the most severe depletion. This observation raises critical questions about whether glutathione deficiency represents a consequence of renal failure or an active contributor to progression—and whether restoration through supplementation might slow decline. academic.oup
Acute Kidney Injury Treatment
A clinical trial evaluating combination therapy with reduced glutathione plus Chuan Huang Fang (a traditional Chinese medicine formula) in acute kidney injury superimposed on chronic kidney disease demonstrated superior renal function preservation compared to glutathione alone. The combination therapy produced greater reductions in serum creatinine, blood urea nitrogen, and uric acid, alongside better estimated glomerular filtration rate (eGFR) improvement. frontiersin
Urinary acute kidney injury biomarkers—neutrophil gelatinase-associated lipocalin (NGAL) and interleukin-18—decreased significantly more in the combination therapy group, indicating reduced tubular injury and inflammation. These findings suggest that glutathione supplementation may serve as a renal protective adjunct during acute kidney injury episodes, potentially reducing the severity of injury and accelerating recovery. frontiersin
The mechanistic basis involves glutathione's role in neutralizing the massive generation of oxygen free radicals during acute kidney injury, preventing the depletion of endogenous antioxidants, and reducing inflammatory mediator secretion that drives progressive kidney damage. Given the limited therapeutic options for acute kidney injury beyond supportive care and addressing underlying causes, glutathione's potential to mitigate oxidative and inflammatory injury warrants larger-scale clinical investigation. frontiersin
7. Autism Spectrum Disorder: Oxidative Stress and Transsulfuration Metabolism
Glutathione Deficiency in Autism
Children diagnosed with autism spectrum disorder exhibit 20-40% lower plasma reduced glutathione levels compared to typically developing children, accompanied by elevated oxidized glutathione, indicating chronic oxidative stress. This redox imbalance occurs alongside broader abnormalities in transsulfuration pathway metabolites—the biochemical sequence that produces glutathione from methionine through cysteine—with autistic children showing reduced cysteine, taurine, and sulfate levels. pmc.ncbi.nlm.nih
The mechanistic connection between glutathione deficiency and autism pathophysiology involves multiple pathways: impaired detoxification of environmental toxins and endogenous metabolic byproducts, dysregulation of glutamate receptor function (specifically NMDA receptors) that contributes to glutamate excitotoxicity and neuronal dysfunction, mitochondrial dysfunction driven by insufficient antioxidant protection, and neuroinflammation amplified by oxidative stress. goldencaretherapy
Clinical Trial Results
An 8-week open-label trial evaluated oral lipoceutical glutathione (n=13) and transdermal glutathione (n=13) in children aged 3-13 years with autism diagnoses. Oral glutathione supplementation significantly increased plasma reduced glutathione levels, though whole-blood glutathione did not show significant changes, suggesting compartment-specific effects. Both oral and transdermal treatments substantially increased plasma sulfate, cysteine, and taurine—metabolites in the transsulfuration pathway—indicating improved metabolic function in this biochemical system. pmc.ncbi.nlm.nih
The study's limitations include small sample size, open-label design without placebo control, and lack of behavioral outcome measures to assess whether biochemical improvements translated to clinical symptom reduction. The researchers emphasized that these results demonstrate glutathione's capacity to improve transsulfuration metabolite profiles but noted uncertainty about whether the increases resulted from direct glutathione delivery or from breakdown of supplemented glutathione providing precursor amino acids. pmc.ncbi.nlm.nih
Future research directions must address whether glutathione supplementation produces clinically meaningful behavioral improvements in autism—reductions in repetitive behaviors, improved social communication, decreased anxiety or irritability—rather than merely normalizing biochemical markers. The preliminary evidence establishes biological plausibility and target engagement (glutathione levels do increase with supplementation) but falls short of demonstrating therapeutic efficacy for core autism symptoms.
8. Inflammatory Bowel Disease: Crohn's Disease and Ulcerative Colitis
Intestinal Glutathione Synthesis Impairment
Inflammatory bowel disease involves chronic, relapsing inflammation of the gastrointestinal tract, with reactive oxygen species from activated neutrophils and macrophages contributing substantially to tissue injury. Glutathione represents the most important intracellular antioxidant in intestinal epithelial cells, providing first-line defense against oxidative damage. pmc.ncbi.nlm.nih
A comprehensive analysis of surgical colonic samples from 26 ulcerative colitis patients, 14 Crohn's colitis patients, and controls revealed that reduced glutathione levels decreased significantly in both non-inflamed and inflamed mucosa in inflammatory bowel disease patients compared to controls. Oxidized glutathione (GSSG) increased proportionally with inflammation severity. Critically, the enzyme activity of γ-glutamylcysteine synthetase (γ-GCS)—the rate-limiting enzyme in glutathione synthesis—was reduced in non-inflamed mucosa and further decreased in inflamed tissue, alongside diminished γ-glutamyl transferase (γ-GT) activity. pmc.ncbi.nlm.nih
This enzymatic deficiency indicates that inflammatory bowel disease involves fundamental impairment of the intestinal mucosa's capacity to synthesize glutathione, not merely increased consumption due to oxidative stress. The reduced γ-GCS activity in non-inflamed mucosa of Crohn's disease patients suggests either an intrinsic defect in glutathione synthesis capacity or chronic, subclinical oxidative stress even in macroscopically normal-appearing tissue. pmc.ncbi.nlm.nih
Chronic Inflammation and Antioxidant Depletion
The observation that inflammatory bowel disease patients—even during clinical remission—demonstrate reduced antioxidant defenses suggests a pre-existing redox imbalance that may predispose to disease flares. Malondialdehyde, a lipid peroxidation product, increases in both ulcerative colitis and Crohn's disease mucosa, while glutathione peroxidase and glutathione levels decrease, particularly in inflamed tissue. pmc.ncbi.nlm.nih
Decreased availability of cysteine—the rate-limiting amino acid for glutathione synthesis—accompanies inflammatory episodes in inflammatory bowel disease, with plasma cysteine and cystine levels dropping during active inflammation. This creates a vicious cycle: inflammation depletes cysteine through increased oxidative stress and protein catabolism, reduced cysteine availability limits glutathione synthesis, and insufficient glutathione antioxidant capacity permits continued oxidative damage that perpetuates inflammation. pmc.ncbi.nlm.nih
Therapeutic strategies targeting glutathione restoration in inflammatory bowel disease face the challenge of delivering glutathione to intestinal mucosa while bypassing systemic circulation. Liposomal formulations offer theoretical advantages for intestinal delivery, as phospholipid vesicles may interact with intestinal epithelial cell membranes more readily than free glutathione. However, no large-scale clinical trials have definitively established glutathione supplementation efficacy for inflammatory bowel disease symptom control or mucosal healing.
9. HIV/AIDS: Immune Restoration and Opportunistic Infection Control
Glutathione Depletion in HIV Infection
HIV infection produces profound glutathione depletion through multiple mechanisms: direct viral effects on cellular metabolism, chronic immune activation generating sustained oxidative stress, and increased consumption of antioxidants combating persistent viral replication. HIV-positive individuals demonstrate significantly lower glutathione levels in peripheral blood mononuclear cells, with the magnitude of depletion correlating with disease progression markers including CD4+ T cell counts and viral load. pmc.ncbi.nlm.nih
The HIV transactivator of transcription (TAT) protein—a key regulatory protein that HIV produces—directly increases oxidative stress and reduces cellular glutathione levels, creating a microenvironment that favors viral replication. This mechanism establishes glutathione depletion not as a passive consequence of infection but as an active component of HIV pathogenesis that the virus exploits to facilitate its own replication. emjreviews
Clinical Trial: Liposomal Glutathione for Immune Restoration
A 13-week randomized, placebo-controlled trial evaluated liposomal glutathione supplementation in HIV-positive individuals with CD4+ T cell counts below 350 cells/mm³—indicating significant immunosuppression but not yet meeting AIDS-defining criteria. The study produced remarkable immunological improvements: experts.llu
Th1 Cytokine Enhancement: IL-12 levels increased threefold, interferon-γ approximately twofold, with significant increases also in IL-1β and TNF-α—cytokines that promote cell-mediated immunity and antiviral responses. pmc.ncbi.nlm.nih
Immunosuppressive Cytokine Reduction: IL-10 and TGF-β—cytokines that dampen immune responses and create an immunosuppressive environment—decreased substantially in the liposomal glutathione group compared to placebo. IL-6, a pro-inflammatory cytokine associated with chronic inflammation and oxidative stress in HIV, also decreased significantly. pmc.ncbi.nlm.nih
Functional Immune Cell Improvement: In vitro assays using peripheral blood mononuclear cells collected after 13 weeks of supplementation demonstrated improved intracellular control of Mycobacterium tuberculosis infection within macrophages. This functional outcome indicates that glutathione restoration translated to meaningful enhancement of immune cells' capacity to control opportunistic pathogens—precisely the clinical need in HIV-associated immunodeficiency. pmc.ncbi.nlm.nih
The shift from Th2-directed (antibody-mediated, often less effective against intracellular pathogens) toward Th1-directed (cell-mediated, crucial for controlling viral and mycobacterial infections) immune responses represents a fundamental correction of the immunological imbalance that HIV infection creates. This rebalancing may explain why HIV-positive individuals receiving glutathione supplementation demonstrated improved control of tuberculosis, a leading cause of mortality in people living with HIV. pmc.ncbi.nlm.nih
10. Chronic Fatigue Syndrome and Mitochondrial Dysfunction
Mitochondrial Basis of Chronic Fatigue
Chronic fatigue syndrome (CFS)—characterized by profound, unexplained fatigue lasting more than six months that rest does not relieve—affects millions globally yet lacks definitive diagnostic tests or FDA-approved treatments. Emerging evidence increasingly points to mitochondrial dysfunction as a central pathophysiological mechanism, with impaired cellular energy production leaving patients unable to generate sufficient ATP for normal physiological functions. advmedny
Research demonstrates that CFS patients often exhibit mitochondrial dysfunction, decreased oxidative phosphorylation efficiency, elevated ventricular cerebrospinal fluid lactate (indicating incomplete aerobic metabolism and reliance on less efficient anaerobic pathways), and reduced brain glutathione levels measured via magnetic resonance spectroscopy. These abnormalities persist during symptomatic periods and partially normalize during temporary improvements, establishing a correlation between mitochondrial/redox dysfunction and symptom severity. pmc.ncbi.nlm.nih
Glutathione's Role in Mitochondrial Health
Glutathione plays essential roles in maintaining mitochondrial function: protecting mitochondrial DNA from oxidative damage, preventing lipid peroxidation of mitochondrial membranes that disrupts electron transport chain function, regulating mitochondrial glutathione pools that determine susceptibility to apoptosis, and supporting the Krebs cycle and oxidative phosphorylation by maintaining appropriate NAD+/NADH ratios. pmc.ncbi.nlm.nih
Brain magnetic resonance spectroscopy studies revealed decreased glutathione concentrations in CFS patients compared to healthy controls, consistent with chronic oxidative stress. Importantly, a similar glutathione reduction occurs in depression, highlighting that this neurochemical abnormality lacks diagnostic specificity for CFS but may represent a common final pathway in conditions characterized by neurological symptoms and fatigue. pmc.ncbi.nlm.nih
Clinical Evidence and Nutrient Combinations
Clinical trials evaluating mitochondrial-supporting nutrient combinations—including components that enhance glutathione function—demonstrated a 35.5% reduction in fatigue and 26.8% increase in mitochondrial function after 12 weeks of supplementation. After a 12-week washout period, fatigue increased and mitochondrial function decreased back toward baseline levels, establishing temporal causality between supplementation and improvement. pmc.ncbi.nlm.nih
The supplements studied typically combined multiple mitochondrial cofactors: L-carnitine (facilitates fatty acid transport into mitochondria), alpha-lipoic acid (antioxidant and cofactor in energy metabolism), coenzyme Q10 (electron carrier in the electron transport chain), reduced NADH (electron donor), and membrane phospholipids that restore mitochondrial membrane integrity. This multi-component approach reflects the reality that mitochondrial dysfunction involves multiple deficiencies, and glutathione restoration alone—though potentially beneficial—may not fully reverse the complex metabolic derangements in CFS. pmc.ncbi.nlm.nih
IV glutathione therapy anecdotally produces rapid but transient energy improvements in some CFS patients, but lacks rigorous placebo-controlled trial evidence. The brief duration of benefit following single infusions (typically hours to days) suggests that sustained improvement requires either continuous supplementation or addressing underlying factors that perpetuate glutathione depletion—chronic infections, ongoing oxidative stress, or genetic polymorphisms affecting glutathione synthesis. advmedny
Liposomal Delivery: The Bioavailability Revolution
Comparative Absorption Profiles
The therapeutic potential of glutathione supplementation remained largely unrealized for decades due to the formidable bioavailability challenge: standard oral glutathione undergoes extensive degradation by gastric acid and intestinal peptidases before reaching systemic circulation. Pharmacokinetic studies established that conventional oral glutathione achieves only 3-5% bioavailability—meaning 95-97% of each dose represents metabolically degraded, wasted product that never reaches target tissues. wishnew
Liposomal technology transforms this limitation by encapsulating glutathione within phospholipid bilayer vesicles—microscopic spheres constructed from the same phospholipid molecules that comprise human cell membranes. This biomimetic design enables liposomes to traverse the intestinal epithelium through multiple mechanisms: direct fusion with enterocyte membranes, lymphatic absorption bypassing first-pass hepatic metabolism, and protection from enzymatic degradation during gastrointestinal transit. wishnew
Clinical pharmacokinetic studies quantifying liposomal glutathione absorption demonstrate:
Bioavailability: 50-90% (quality-dependent) versus 3-5% for standard forms—representing 10-18 fold improvement wishnew
Peak Blood Concentration (Cmax): 8-12 times higher with liposomal delivery wishnew
Area Under Curve (AUC): 600-2250% greater total absorption, indicating sustained elevated levels throughout the dosing interval wishnew
Time to Peak (Tmax): 2-3 hours for liposomal versus 4-6 hours for standard oral forms, indicating faster absorption kinetics wishnew
Elimination Half-life: 5-8 hours for liposomal versus 2-3 hours for standard forms, producing more sustained tissue exposure wishnew
Intracellular Penetration: Beyond Plasma Levels
A critical distinction separates liposomal glutathione from alternative strategies: it achieves true intracellular delivery, not merely elevated extracellular or plasma concentrations. The Penn State study's measurement of peripheral blood mononuclear cell glutathione content—increasing 100% after two weeks of liposomal supplementation—definitively establishes that absorbed glutathione penetrates immune cells and becomes available for intracellular antioxidant functions. pmc.ncbi.nlm.nih
This cellular uptake proves essential because glutathione cannot cross cell membranes readily in its free tripeptide form due to its charged amino acid residues. The liposomal carrier facilitates membrane fusion or endocytosis, delivering glutathione cargo directly into the cytoplasm where it supports glutathione peroxidase, glutathione reductase, and glutathione S-transferase enzyme systems.
Tissue-specific absorption patterns reveal that liposomal glutathione increases hepatic glutathione by 35-65%—critical for liver detoxification support. Brain uptake remains uncertain for oral liposomal formulations due to blood-brain barrier limitations, though some evidence suggests phospholipid carriers may enhance penetration compared to free glutathione. Intranasal and intravenous routes offer more reliable brain delivery for neurodegenerative conditions where central nervous system glutathione restoration represents the therapeutic target. wishnew
Dosage, Safety, and Clinical Considerations
Evidence-Based Dosing Recommendations
Clinical trials employed glutathione doses ranging from 250mg to 2000mg daily, with most therapeutic studies utilizing 500-1000mg divided into one or two daily doses. The Penn State immune function study demonstrated equivalent efficacy between 500mg and 1000mg daily doses, suggesting that benefits plateau beyond moderate dosing and that higher doses do not necessarily produce proportionally greater effects. vinmec
For specific conditions, evidence-informed recommendations include:
Metabolic Dysfunction/Diabetes: 250-500mg daily, sustained for minimum three months to achieve glycemic benefits pmc.ncbi.nlm.nih
Immune Enhancement: 500mg daily, with measurable effects on NK cell function within two weeks pmc.ncbi.nlm.nih
Liver Support: 300-500mg daily for four months alongside lifestyle modifications healthline
HIV Immune Restoration: Doses equivalent to those producing blood level increases of 30-40% (typically 500-750mg daily) for 12-13 weeks pmc.ncbi.nlm.nih
General Antioxidant Support: 250-500mg daily represents a reasonable maintenance dose for individuals with documented glutathione deficiency or high oxidative stress exposure performancelab
Safety Profile and Adverse Events
Oral and liposomal glutathione supplementation demonstrates a favorable safety profile across multiple clinical trials, with adverse events comparable to placebo groups. The most commonly reported side effects remain mild and gastrointestinal in nature: bloating, abdominal cramping, nausea, and loose stools. These symptoms typically occur at doses exceeding 1000mg daily and often resolve with dose reduction or temporary discontinuation followed by gradual reintroduction. riveroaksdripspa
Rare but documented adverse events include:
Allergic Reactions: Rash, itching, or urticaria in sensitive individuals riveroaksdripspa
Respiratory Effects: Inhaled glutathione can provoke bronchoconstriction in asthma patients through sulfite formation—nebulized glutathione is contraindicated in asthma atsjournals
Headache and Dizziness: Occasionally reported, possibly related to rapid blood pressure changes at high doses riveroaksdripspa
WebMD designates oral glutathione doses up to 500mg daily as "possibly safe," with higher doses requiring medical supervision. Importantly, glutathione supplementation should not replace evidence-based treatments for serious conditions but rather serve as adjunct therapy supporting conventional medical care. performancelab
Important Cautions and Contraindications
Cancer Patients: Glutathione exhibits a complex, context-dependent relationship with cancer. In healthy cells, it prevents carcinogen-induced DNA damage and supports tumor suppression. However, in established tumors, elevated glutathione promotes treatment resistance by neutralizing chemotherapy-induced oxidative stress, protecting cancer cells from drug-mediated apoptosis, and facilitating DNA repair that prevents chemotherapy efficacy. Cancer patients—particularly those receiving chemotherapy or radiation—should not supplement with glutathione without oncologist approval. biohackr
Asthma: Nebulized glutathione induces bronchoconstriction in asthma patients through sulfite formation, causing cough, breathlessness, and potentially severe bronchospasm requiring bronchodilator rescue. Oral and liposomal forms do not appear to carry this risk, but asthma patients should exercise caution and medical supervision. atsjournals
Pregnancy and Lactation: Insufficient safety data exists for glutathione supplementation during pregnancy or breastfeeding. While dietary glutathione from food sources poses no risk, concentrated supplementation lacks adequate safety studies in these vulnerable populations.
Medication Interactions: Glutathione may theoretically interact with nitroglycerin (used for angina) by altering nitric oxide dynamics. Patients on chemotherapy, immunosuppressants, or anticoagulants should consult healthcare providers before supplementation due to potential interactions affecting drug metabolism and efficacy.
IV Glutathione: Efficacy Versus Risk
Intravenous glutathione achieves 100% bioavailability and produces immediate, dramatic increases in plasma and tissue glutathione levels. However, IV formulations carry substantially higher risks than oral supplementation: wishnew
FDA Warnings: The U.S. FDA issued safety warnings regarding IV glutathione compounded with L-glutathione after reports of adverse events including severe reactions in seven patients who received 1400mg IV doses. Symptoms included nausea, vomiting, hypotension, difficulty breathing, and one patient requiring hospitalization. fda
Endotoxin Contamination: Compounded IV preparations lack the rigorous quality control of FDA-approved injectable medications, creating risk of bacterial endotoxin contamination that can cause fever, septic shock, and multi-organ failure. fda
Allergic Reactions: IV administration carries heightened risk of severe allergic reactions including anaphylaxis compared to oral routes, as the compound bypasses gastrointestinal barriers that limit absorption of allergenic materials. revivemobileivs
Lack of Standardization: No FDA-approved IV glutathione formulation exists for non-research use; all IV preparations represent "off-label" compounding with inconsistent dosing, quality, and safety oversight. pmc.ncbi.nlm.nih
The risk-benefit calculus for IV glutathione currently favors oral liposomal formulations for most indications. IV administration may be justifiable in acute, severe deficiency states or research protocols but should not represent routine supplementation strategy given the superior safety profile and adequate bioavailability of liposomal oral forms.
Limitations of Current Evidence and Research Gaps
Study Quality and Scale
While this analysis synthesized evidence from over 100 sources, a sober assessment reveals significant limitations in the glutathione clinical trial literature. Many studies cited represent preliminary investigations with small sample sizes (n=12-54), short durations (8-12 weeks), open-label designs lacking placebo controls, or secondary analysis of biomarkers rather than primary clinical outcomes. pmc.ncbi.nlm.nih
The strongest evidence—for diabetes management, immune function, and HIV—derives from moderately sized trials (n=100-450) with randomized designs and objective outcome measures. However, even these studies rarely exceed six months duration, limiting conclusions about long-term efficacy, tolerance development, or sustained clinical benefits. The field urgently requires large-scale (n=500+), multi-year trials with patient-centered clinical endpoints (quality of life, disease progression, mortality) rather than surrogate biochemical markers alone. pmc.ncbi.nlm.nih
Publication Bias and Industry Influence
Glutathione supplementation research faces inherent publication bias: positive preliminary findings generate publications and media attention, while negative or null results often remain unpublished. The cystic fibrosis trial—a large, rigorous, six-month study showing no clinically significant benefits from inhaled glutathione—represents a valuable cautionary counterpoint. Despite clear delivery to airways and measurable increases in sputum glutathione, the intervention failed to improve lung function, reduce exacerbations, or enhance quality of life. atsjournals
This negative trial underscores that demonstrating target engagement (glutathione levels increase) does not guarantee clinical efficacy (symptoms improve). Disease pathophysiology often involves multiple dysregulated pathways, and correcting oxidative stress alone may prove insufficient when inflammation, infection, genetic dysfunction, or structural tissue damage drive symptoms.
Individual Variability and Precision Medicine
Clinical trial averages obscure substantial individual variability in glutathione supplementation response. The Penn State study documented strong inverse correlations between baseline glutathione levels and supplementation response magnitude: individuals with the lowest starting levels experienced the largest increases and potentially the greatest clinical benefits. This observation suggests that indiscriminate supplementation in glutathione-replete individuals may confer minimal benefit, while targeted supplementation in deficient populations could produce meaningful outcomes. pmc.ncbi.nlm.nih
Future research should stratify participants by baseline glutathione status, genetic polymorphisms affecting glutathione synthesis (GCLC, GCLM, GSS variants), oxidative stress biomarker profiles, and disease severity to identify precision medicine approaches that maximize benefit for specific patient subgroups.
Conclusion: Evidence-Informed Recommendations
Liposomal glutathione emerges as a promising intervention for health conditions characterized by oxidative stress, glutathione deficiency, and immune dysfunction. The ten conditions reviewed—type 2 diabetes, neurodegenerative diseases, liver disease, immune dysfunction, cardiovascular disease, kidney disease, autism, inflammatory bowel disease, HIV, and chronic fatigue syndrome—demonstrate varying levels of evidence quality, with the strongest support for metabolic disease, immune enhancement, and HIV-associated immunodeficiency.
The revolutionary improvement in bioavailability achieved through liposomal delivery—transforming glutathione from a poorly absorbed supplement to one achieving 50-90% systemic absorption—fundamentally alters the therapeutic potential of oral supplementation. This technological advancement places liposomal glutathione's efficacy closer to IV administration while maintaining the safety profile of oral supplements.
For individuals with documented glutathione deficiency, high oxidative stress burden (chronic disease, aging, environmental toxin exposure), or conditions with strong mechanistic rationale (diabetes, immune dysfunction, liver disease), a trial of liposomal glutathione supplementation at 500mg daily for 8-12 weeks represents a reasonable, evidence-informed approach. Objective monitoring—through laboratory markers (fasting glucose, HbA1c, liver enzymes), immune function tests, or symptom rating scales—enables assessment of individual response and guides continuation decisions.
However, glutathione supplementation should not replace evidence-based medical treatments, delay appropriate diagnostic evaluation, or substitute for fundamental health practices (nutrition, exercise, sleep, stress management) that support endogenous glutathione production. The evidence positions glutathione as adjunct therapy—supporting but not replacing conventional medical care—for motivated individuals seeking comprehensive approaches to oxidative stress-related conditions.
The future of glutathione therapeutics lies in rigorous, large-scale trials that definitively establish clinical efficacy, identify the patient populations most likely to benefit, optimize dosing strategies, and determine long-term safety. Until such evidence emerges, clinicians and patients must navigate the tension between promising preliminary data and the acknowledged limitations of the current evidence base, making informed decisions that balance potential benefits against costs, modest risks, and the opportunity cost of forgoing alternative interventions.
Related in VitaminDWiki
- Glutathione benefits \"virtually every physiological system\"
- Glutathione helps the Vitamin D Receptor, fights viral infections, etc.
- How Liposomal Glutathione fights 9 health problems
- Glutathione fights Parkinson's Disease
- Glutathione fights Alz, Park, Cardio, Liver, COPD. Asthma, etc
- Glutathione is often better than Vitamin D in fighting many toxins
- Glutathione and Vitamin D synergism - many studies
- Glutathione Depleted by Chronic Illnesses