5,000 IU daily or 50,000 IU Vitamin D weekly repleted many dark skinned adolescents – RCT
Treatment of Vitamin D Deficiency in Predominantly Hispanic and Black Adolescents: A Randomized Clinical Trial
Journal of Pediatrics – online first
Hina J. Talib, MDcorrespondenceemail, Tulasi Ponnapakkam, PhD, Robert Gensure, MD, PhD, Hillel W. Cohen, DrPH, MPH, Susan M. Coupey, MD
📄 Download the PDF from VitaminDWiki
Objectives
To compare 3 different treatment regimens for vitamin D deficiency in minority adolescents and to explore factors that impact treatment efficacy.
Study design
We conducted an 8-week, prospective, open-label, randomized clinical trial in an urban, academic, children's hospital.
A total of 183 vitamin D-deficient adolescents,
mean 25-hydroxyvitamin D or 25(OH)D 13.7 ± 3.9 ng/mL;
mean age 16.6 ± 2.2 years,
were randomized into 3 vitamin D3 (cholecalciferol) treatment arms: 50 000 IU/wk; 5000 IU/d; and 1000 IU/d. Serum 25(OH)D and vitamin D binding protein (VDBP) levels were measured pre-and posttreatment; 122 (67%) participants completed posttreatment measures. Complete-case and multiple-imputation, intention-to-treat analyses were performed.
Results
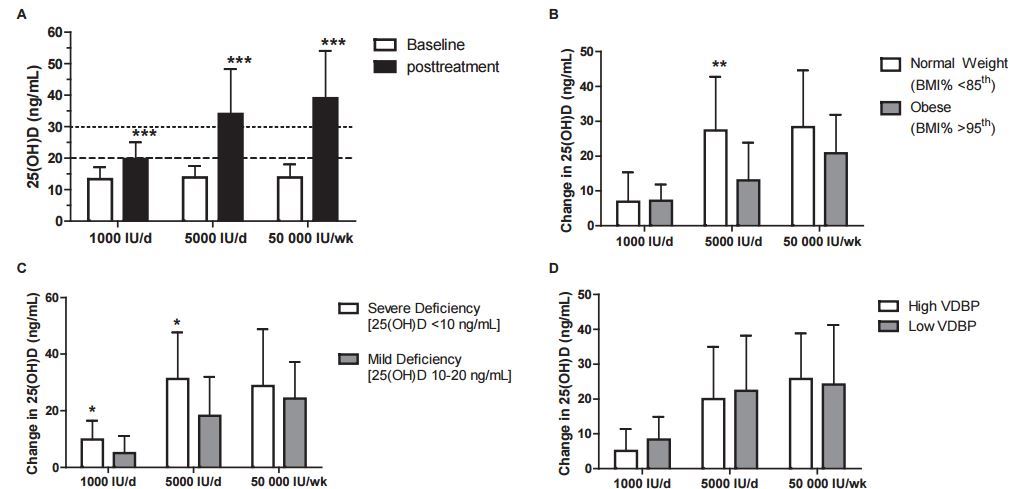
Mean change in 25(OH)D level posttreatment was significantly different among the 3 arms, 24.9 ± 15.1 vs 21.0 ± 15.2 vs 6.2 ± 6.5 ng/mL, for 50 000 IU, 5000 IU, and 1000 IU doses, respectively, P < .001. Both high-dose treatments were effective in increasing the 25(OH)D level out of deficiency range (≥20 ng/mL) in more than 80% of participants, and 60% remained deficient after low-dose treatment. Only 72%, 56%, and 2% achieved vitamin D sufficiency (>30 ng/mL) with 50 000 IU, 5000 IU, and 1000 IU doses, respectively, P < .001.
Obese participants had substantially less mean change in 25(OH)D level after treatment than normal-weight participants, 13.7 ± 10.7 vs 21.9 ± 16.9 ng/mL, P < .001.
Mean baseline VDBP level was almost twice as high in Hispanic compared with black participants (P < .001) and did not alter treatment response or change with treatment.
Conclusions
Adult-sized adolescents require 8 weeks of high-dose cholecalciferol, at least 5000 IU/d, to correct deficiency. Obese adolescents have poorer response to treatment and may need higher doses than nonobese youth. Hispanic and black adolescents have different VDBP levels but similar treatment responses.
Trial registration: ClinicalTrials.gov: NCT01784029.