Harmonization of serum 25-hydroxycalciferol assay results from high-performance liquid chromatography, enzyme immunoassay, radioimmunoassay, and immunochemiluminescence systems: A multicenter study
Different results by 5 types of testers on 275 blood samples
| Tester | Def <11 ng | Insufficient 11 - 20 ng | Sufficient > 20 ng | Comments |
| HPLC | 36% | 30% | 34% | the standard |
| ECL-Roche | 33% | 30% | 38% | OK if not taking Biotin |
| CLIA-Diasorin | 48% | 33% | 18% | too low |
| EIA-DIAsource | 15% | 41% | 41% | too high |
| RIA-DIAsource | 30% | 26% | 43% | too high |
Roche reads 9 ng too high if take 10 mg of Biotin daily for a week
J Clin Lab Anal. 2017 Nov;31(6). doi: 10.1002/jcla.22117. Epub 2017 Feb 7.
Nikooyeh B1, Samiee SM2, Farzami MR2, Alavimajd H3, Zahedirad M1, Kalayi A1, Shariatzadeh N1, Boroumand N3, Golshekan E2, Gholamian Y2, Neyestani TR1.
Tests for Vitamin D category listing has 160 items
- This problem along with other problems with vitamin D testers have been documented by many studies
- Greatly improved Vitamin D testing repeatability – May 2020
- Problems with Vitamin D Testing – chapter – Aug 2019
- How to compare Vitamin D measurements from multiple studies – July 2021
- Big differences (~10 ng) in vitamin D test results, even when using the same type of tester – Aug 2015
- Huge differences in % deficient (< 30ng) depending on the tester used
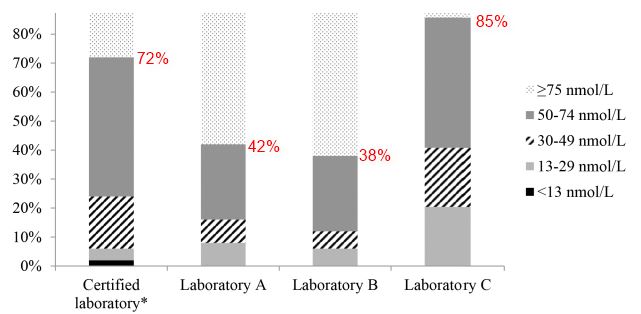
- Note: A, B, and C unable to detect/measure < 13 nmol (5 ng)
- 4 popular vitamin D testers gave very different results (no surprise) – June 2021
- Percent who are Vitamin D Deficient: 6, 9, or 22 – depends on testing system – Oct 2014
- No vitamin D test needed before supplementing (typically) – April 2014
- Vitamin D tester falsely said half of hemodialysis patients had less than 30 ng – Jan 2013
- Vitamin D measurements vary with the same sample of blood – March 2014
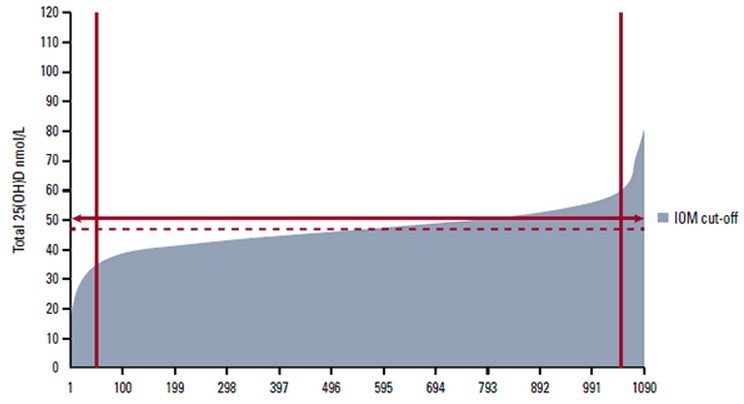
1090 tests of the same blood sample on the same type of tester
BACKGROUND:
Remarkable disagreement among different systems of 25-hydroxy vitamin D 25(OH)D assay makes decision making for both clinical and community interventions very difficult. This study aimed to harmonize the results obtained from different 25(OH)D assay systems.
METHODS:
A total of 275 serum samples were analyzed for 25(OH)D using DIAsource-enzyme immunoassay (EIA), DIAsource-radioimmunoassay (RIA), Roche-electrochemiluminescence (ECL), Diasorin-chemiluminescent immunoassay (CLIA), and high-performance liquid chromatography (HPLC), as the reference method. Serum intact parathyroid hormone (iPTH) was also measured in all samples. Between-system agreement and harmonization were evaluated using Bland-Altman analysis, receiver operating characteristic (ROC), and regression analysis.
RESULTS:
Mean serum 25(OH)D concentrations and frequency distribution of vitamin D status showed a significant difference among the studied systems (P<.001 for both). Serum 25(OH)D assay results from all systems correlated with those from HPLC. As compared with HPLC, ECL showed a positive bias (+3.8 nmol/L), whereas CLIA had a negative bias (-11.9 nmol/L). Both EIA and RIA showed a more or less similar positive bias (8.0 and 8.1 nmol/L, respectively). Using serum iPTH-based 25(OH)D cutoff points, only ECL results became comparable to and without significant difference with HPLC. However, when system-specific cutoffs were defined based on HPLC results using regression equations, mean 25(OH)D and frequency distribution of vitamin D status were more harmonized compared with the other methods.
CONCLUSION:
Our findings showed that with adjustment of circulating 25(OH)D based on HPLC, frequency distribution of vitamin D status, as judged by different methods, can be well harmonized with no statistically significant inter-system difference.
PMID: 28169461 DOI: 10.1002/jcla.22117
4088 visitors, last modified 08 Jul, 2021,
Printer Friendly
Follow this page for updates
- This problem along with other problems with vitamin D testers have been documented by many studies
- Greatly improved Vitamin D testing repeatability – May 2020
- Problems with Vitamin D Testing – chapter – Aug 2019
- How to compare Vitamin D measurements from multiple studies – July 2021
- Big differences (~10 ng) in vitamin D test results, even when using the same type of tester – Aug 2015
- Huge differences in % deficient (< 30ng) depending on the tester used
- Note: A, B, and C unable to detect/measure < 13 nmol (5 ng)
- 4 popular vitamin D testers gave very different results (no surprise) – June 2021
- Percent who are Vitamin D Deficient: 6, 9, or 22 – depends on testing system – Oct 2014
- No vitamin D test needed before supplementing (typically) – April 2014
- Vitamin D tester falsely said half of hemodialysis patients had less than 30 ng – Jan 2013
- Vitamin D measurements vary with the same sample of blood – March 2014
1090 tests of the same blood sample on the same type of tester
BACKGROUND:
Remarkable disagreement among different systems of 25-hydroxy vitamin D 25(OH)D assay makes decision making for both clinical and community interventions very difficult. This study aimed to harmonize the results obtained from different 25(OH)D assay systems.
METHODS:
A total of 275 serum samples were analyzed for 25(OH)D using DIAsource-enzyme immunoassay (EIA), DIAsource-radioimmunoassay (RIA), Roche-electrochemiluminescence (ECL), Diasorin-chemiluminescent immunoassay (CLIA), and high-performance liquid chromatography (HPLC), as the reference method. Serum intact parathyroid hormone (iPTH) was also measured in all samples. Between-system agreement and harmonization were evaluated using Bland-Altman analysis, receiver operating characteristic (ROC), and regression analysis.
RESULTS:
Mean serum 25(OH)D concentrations and frequency distribution of vitamin D status showed a significant difference among the studied systems (P<.001 for both). Serum 25(OH)D assay results from all systems correlated with those from HPLC. As compared with HPLC, ECL showed a positive bias (+3.8 nmol/L), whereas CLIA had a negative bias (-11.9 nmol/L). Both EIA and RIA showed a more or less similar positive bias (8.0 and 8.1 nmol/L, respectively). Using serum iPTH-based 25(OH)D cutoff points, only ECL results became comparable to and without significant difference with HPLC. However, when system-specific cutoffs were defined based on HPLC results using regression equations, mean 25(OH)D and frequency distribution of vitamin D status were more harmonized compared with the other methods.
CONCLUSION:
Our findings showed that with adjustment of circulating 25(OH)D based on HPLC, frequency distribution of vitamin D status, as judged by different methods, can be well harmonized with no statistically significant inter-system difference.
PMID: 28169461 DOI: 10.1002/jcla.22117
| 4088 visitors, last modified 08 Jul, 2021, |