Pregnancy helped by Magnesium - many studies
800 mg of Magnesium early in 3rd trimester significantly increased brain activity in preterm infants – RCT May 2024
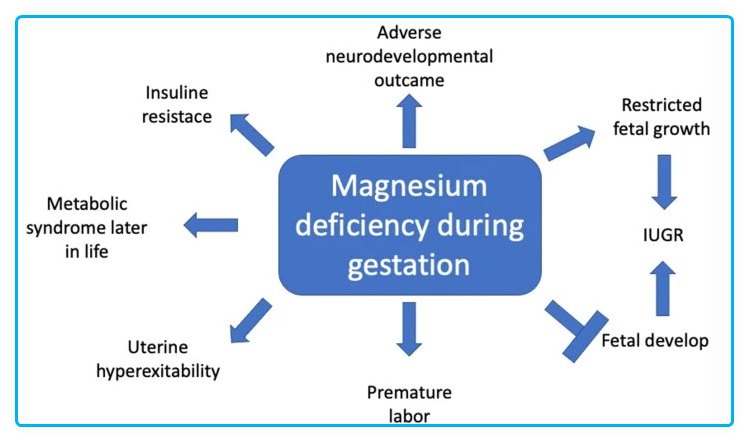
The Role of Magnesium in Pregnancy and in Fetal Programming of Adult Diseases - 2020
Helped a lot 📄 PDF
Effect of Magnesium Supplement on Pregnancy Outcomes: RCT - 2017
Helped a lot 📄 PDF
800 mg of Magnesium early in 3rd trimester significantly increased brain activity in preterm infants – RCT May 2024
Preterm labor 1.8X more likely if low Magnesium - 2014
A Study on the Association between Low Maternal Serum Magnesium Level and Preterm Labour
Advances in Medicine, Volume 2014 (2014), Article ID 704875, 6 pages, http://dx.doi.org/10.1155/2014/704875
Kehinde S. Okunade, Ayodeji A. Oluwole, and Maymunah A. Adegbesan-Omilabu
Department of Obstetrics & Gynaecology, Lagos University Teaching Hospital, Lagos, Nigeria
Objectives. The study was aimed to assess the association between low maternal serum magnesium levels and preterm labour. Methods. It is a cross-sectional case-control study in which eligible participants were pregnant women admitted in labour within the labour ward complex of a Lagos tertiary hospital. Relevant data were extracted from the case records of these women and blood samples were obtained from all participants and serum magnesium levels measured.
Results. The study showed that 36% of the study patients had varying degrees of hypomagnesaemia.
The relative risk indicates that preterm labour is 1.83 times higher among the patients with low serum magnesium (less than 1.6 mg/dL). The mean difference in serum magnesium levels in both groups was statistically significant ().
Conclusion. We can infer that low serum magnesium (hypomagnesaemia) is associated with preterm onset of labour. We can, also from this finding, formulate a proposition that would help in preventing preterm labour and birth with the use of prophylactic oral magnesium supplementation among patients with higher risk for development of preterm labour.
📄 Download the PDF from VitaminDWiki
Importance of Magnesium in Pregnancy – Sept 2016
Magnesium in pregnancy
Nutr Rev. 2016 Sep;74(9):549-57. doi: 10.1093/nutrit/nuw018. Epub 2016 Jul 21.
Dalton LM1, Ní Fhloinn DM1, Gaydadzhieva GT1, Mazurkiewicz OM1, Leeson H1, Wright CP2.
Magnesium deficiency is prevalent in women of childbearing age in both developing and developed countries. The need for magnesium increases during pregnancy, and the majority of pregnant women likely do not meet this increased need. Magnesium deficiency or insufficiency during pregnancy may pose a health risk for both the mother and the newborn, with implications that may extend into adulthood of the offspring. The measurement of serum magnesium is the most widely used method for determining magnesium levels, but it has significant limitations that have both hindered the assessment of deficiency and affected the reliability of studies in pregnant women. Thus far, limited studies have suggested links between magnesium inadequacy and certain conditions in pregnancy associated with high mortality and morbidity, such as
gestational diabetes,
preterm labor,
preeclampsia, and
small for gestational age or
intrauterine growth restriction.
This review provides recommendations for further study and improved testing using measurement of red cell magnesium. Pregnant women should be counseled to increase their intake of magnesium-rich foods such as nuts, seeds, beans, and leafy greens and/or to supplement with magnesium at a safe level.
📄 Download the PDF from Sci-Hub.tw via VitaminDWiki
Pre-eclampsia inversely proportional to serum Magnesium – Oct 2014
Cochrane review of a variety of Magnesium compounds during pregnancy found some benefit - 2014
Magnesium supplementation in pregnancy.
Cochrane Database Syst Rev. 2014 Apr 3;4:CD000937. doi: 10.1002/14651858.CD000937.pub2.
Makrides M1, Crosby DD, Bain E, Crowther CA.
Healthy Mothers, Babies and Children, South Australian Health and Medical Research Institute, C/- WCHRI, 72 King William Road, North Adelaide, SA, Australia, 5006.
BACKGROUND:
Magnesium is an essential mineral required for regulation of body temperature, nucleic acid and protein synthesis and in maintaining nerve and muscle cell electrical potentials. Many women, especially those from disadvantaged backgrounds, have low intakes of magnesium. Magnesium supplementation during pregnancy may be able to reduce fetal growth restriction and pre-eclampsia, and increase birthweight.
OBJECTIVES:
To assess the effects of magnesium supplementation during pregnancy on maternal, neonatal/infant and paediatric outcomes.
SEARCH METHODS:
We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (31 March 2013).
SELECTION CRITERIA:
Randomised and quasi-randomised trials assessing the effects of dietary magnesium supplementation during pregnancy were included. The primary outcomes were perinatal mortality (including stillbirth and neonatal death prior to hospital discharge), small-for-gestational age, maternal mortality and pre-eclampsia.
DATA COLLECTION AND ANALYSIS:
Two review authors independently assessed study eligibility, extracted data and assessed the risk of bias of included studies.
MAIN RESULTS:
Ten trials involving 9090 women and their babies were included; one trial had a cluster design (with randomisation by study centre).
All 10 trials randomly allocated women to either an oral magnesium supplement or a control group; in eight trials a placebo was used, and in two trials no treatment was given to the control group. In the 10 included trials, the compositions of the magnesium supplements, gestational ages at commencement, and doses administered varied, including:
magnesium oxide, 1000 mg daily from ≤ four months post-conception (one trial);
magnesium citrate, 365 mg daily from ≤ 18 weeks until hospitalisation after 38 weeks (one trial), and 340 mg daily from nine to 27 weeks' gestation (one trial);
magnesium gluconate, 2 to 3 g from 28 weeks' gestation until birth (one trial), and 4 g daily from 23 weeks' gestation (one trial);
magnesium aspartate, 15 mmol daily (three trials, commencing from either six to 21 weeks' gestation until birth, ≤ 16 weeks' gestation until birth, or < 12 weeks until birth), or 365 mg daily from 13 to 24 weeks until birth (one trial); and
magnesium stearate, 128 mg elemental magnesium from 10 to 35 weeks until birth (one trial).
In the analysis of all trials, oral magnesium supplementation compared to no magnesium was associated with no significant difference in perinatal mortality (stillbirth and neonatal death prior to discharge) (risk ratio (RR) 1.10; 95% confidence interval (CI) 0.72 to 1.67; five trials, 5903 infants),
small-for-gestational age (RR 0.76; 95% CI 0.54 to 1.07; three trials, 1291 infants), or
pre-eclampsia (RR 0.87; 95% CI 0.58 to 1.32; three trials, 1042 women).
None of the included trials reported on maternal mortality.Considering secondary outcomes, while no increased risk of stillbirth was observed, a possible increased risk of neonatal death prior to hospital discharge was shown for infants born to mothers who had received magnesium (RR 2.21; 95% CI 1.02 to 4.75; four trials, 5373 infants). One trial contributed over 70% of the participants to the analysis for this outcome; the trial authors suggested that the large number of severe congenital anomalies in the supplemented group (unlikely attributable to magnesium) and the deaths of two sets of twins (with birthweights < 750 g) in the supplemented group likely accounted for the increased risk of death observed, and thus this result should be interpreted with caution. Furthermore, when the deaths due to severe congenital abnormalities in this trial were excluded from the meta-analysis, no increased risk of neonatal death was seen for the magnesium supplemented group.
Magnesium supplementation was associated with significantly fewer babies with an
Apgar score less than seven at five minutes ( RR 0.34 ; 95% CI 0.15 to 0.80; four trials, 1083 infants), with meconium-stained liquor (RR 0.79; 95% CI 0.63 to 0.99; one trial, 4082 infants),
late fetal heart decelerations (RR 0.68; 95% CI 0.53 to 0.88; one trial, 4082 infants), and
mild hypoxic-ischaemic encephalopathy (RR 0.38; 95% CI 0.15 to 0.98; one trial, 4082 infants).
Women receiving magnesium were significantly less likely to require hospitalisation during pregnancy (RR 0.65 , 95% CI 0.48 to 0.86; three trials, 1158 women).
Of the 10 trials included in the review, only two were judged to be of high quality overall. When an analysis was restricted to these two trials none of the review's primary outcomes (perinatal mortality, small-for-gestational age, pre-eclampsia) were significantly different between the magnesium supplemented and control groups.
AUTHORS' CONCLUSIONS: There is not enough high-quality evidence to show that dietary magnesium supplementation during pregnancy is beneficial.
PMID: 24696187 📄 Download the PDF from VitaminDWiki
studies in both of the VitaminDWiki categories Pregnancy and Magnesium
This list is automatically updated
{category}
Google Sites has the following
(Use original to access the links)
Low magnesium associated with miscarriage
Compared with controls, a significant decrease in magnesium, with increase of the calcium/magnesium ratio, was found in miscarriage.
Low magnesium, phosphorus found in threatened miscarriage
The study showed symptoms of threatened miscarriage are related to decreased concentrations of inorganic phosphorus, magnesium, total protein and albumin and reduced activity of total alkaline phosphatase activity (alkaline phosphatases are most effective in an alkaline environment). Women who did not undergo miscarriage showed significantly higher inorganic phosphorus concentration compared to those who lost pregnancy, what might be of prognostic value. Phosphorus and Miscarriage (link)
100% of previously infertile women gave birth after normalizing magnesium levels
After a further two months of 200 micrograms daily oral selenium as selenomethionine and oral magnesium supplements, all six women normalized their RBC-Mg (P < 0.0001) and RBC-GSH-Px (P < 0.0001) levels. All 12 previously infertile women have produced normal healthy babies all conceiving within eight months of normalizing their red blood cell magnesium levels (600 mg/day magnesium). Selenium supplementation (200mcg) was necessary for 6 of the women to normalize their red blood cell magnesium levels. Selenium and miscarriage (link)
Magnesium deficiency linked to miscarriage and birth defects
Some studies suggest that magnesium deficiency may play a role in miscarriage of diabetic women, in fetal malformations and in the pathogenesis of neonatal hypocalcemia of the infants of diabetic mothers.
Magnesium prevents preterm labor
Magnesium supplementation during pregnancy seems necessary because it improves maternal health and fetal outcome.
Magnesium supplementation reduces the incidence of preterm labour and vaginal haemorrhage.
Premature delivery is significantly reduced from 8.2 to 2.8%.
Intravenous magnesium application in pharmacological doses is still the therapeutic basis in pre-eclampsia and eclampsia.
(Note by VitaminDWiki - Intravenous Magnesium delays delivery by a few days to a week. Wonder about having adequate Mg during pregnancy)
Magnesium deficiency during pregnancy associated with fetal death in animals
Magnesium deficiency during gestation significantly increased neonatal mortality and morbidity. Such increases were associated with a reduced free magnesium concentration in both maternal and offspring blood and an increased incidence of periventricular hemorrhage and edema in newborn pups as observed by magnetic resonance imaging and histology. Animals fed a magnesium-deficient diet before mating but given magnesium supplementation during gestation did not demonstrate a significant change in neonatal mortality and morbidity when compared to control animals. The significant improvement in fetal outcome with dietary magnesium supports the concept of magnesium supplementation during pregnancy.
Low calcium, iron, zinc and magnesium associated with higher rate of miscarriage
Female rats received a control or a 50% mineral-restricted diet for 12 weeks, by which time mineral-restricted rats had lower plasma iron, zinc, magnesium and calcium concentrations. Following mating with control males, a third of the mineral-restricted dams were shifted to the control diet from parturition. RESULTS: Pregnant mineral-restricted dams had a higher miscarriage rate, and body weights of their pups at birth and weaning were lower.
http://www.ncbi.nlm.nih.gov/pubmed/15296486
Magnesium deficiency leads to insulin resistance
Insulin secretion requires magnesium: magnesium deficiency results in impaired insulin secretion while magnesium replacement restores insulin secretion. Furthermore, experimental magnesium deficiency reduces the tissues sensitivity to insulin.
Insulin Resistance and Miscarriage (link)
Low magnesium associated with premenstrual tension
Magnesium deficiency has been implicated as a possible causative factor in premenstrual tension (PMT). We have assessed serum and red cell magnesium concentration in nine normal premenopausal women and 26 PMT patients, using atomic absorption spectrometry. Mean red cell magnesium level was significantly lower in PMT patients. Red cell magnesium determinations should be included in the evaluation of PMT.
http://www.ajcn.org/cgi/content/abstract/34/11/2364
See also PubMed
Preterm birth and the role of neuroprotection.- Jan 2015
BMJ. 2015 Jan 20;350:g6661. doi: 10.1136/bmj.g6661.
Chang E1.
1Department of Obstetrics and Gynecology, Medical University of South Carolina, Charleston, SC 29492, USA changey@musc.edu.
Preterm birth remains a common complication of pregnancy and causes substantial neonatal morbidity and mortality. As improvements in the care of preterm neonates have outpaced efforts to prevent preterm birth, the numbers of survivors with neurologic sequelae that affect quality of life have increased. The main strategies to reduce the impact of neurologic complications of prematurity include prevention of preterm birth and protection of the developing fetal brain through antenatal administration of drugs. These strategies rely on a basic understanding of the intertwined pathophysiology of spontaneous preterm labor and perinatal brain injury, which will be reviewed here. The review will outline current methods for the prevention of prematurity and neuroprotection. The use of magnesium sulfate as a neuroprotective compound will be discussed, including concerns over its association with increased pediatric mortality and abnormalities in bone density.
PMID: 25646630
The use of intravenous magnesium in non-preeclamptic pregnant women: fetal/neonatal neuroprotection. - May 2015
Arch Gynecol Obstet. 2015 May;291(5):969-75. doi: 10.1007/s00404-014-3581-1. Epub 2014 Dec 12.
Jacquemyn Y1, Zecic A, Van Laere D, Roelens K.
PURPOSE: To review the effect of intravenous magnesium in obstetrics on fetal/neonatal neuroprotection.
METHODS: A systematic review of published studies.
RESULTS: Five randomized trials and 4 meta-analyses have shown a significant 32% reduction of cerebral palsy when administering magnesium sulfate in case of preterm delivery. The pathophysiologic mechanism is not fully unraveled: modulation of the inflammatory process, both in the mother and the fetus, and downregulation of neuronal stimulation seem to be involved. After long-term high-dose intravenous administration of magnesium , maternal and neonatal adverse effects such as maternal and neonatal hypotonia and osteoporosis and specific fetal/neonatal cerebral lesions have been described. In case of administration for less than 48 h at 1 g/h and a loading dose of 4 g, these toxic amounts are not achieved.
American, Canadian and Australian guidelines recommend the use of intravenous magnesium in any threatening delivery at less than 32 weeks .
The "number needed to treat" to avoid 1 cerebral palsy is between 15 and 35.
CONCLUSIONS: Intravenous magnesium significantly reduces the risk for cerebral palsy in preterm birth. Open questions remain the optimal dosing schedule, whether or not repeating when delivery has been successfully postponed and a new episode of preterm labor occurs. Some concern has been raised on a too optimistic value for random error which might have led to over-optimistic conclusions in classic meta-analysis. Randomized trials comparing different doses and individual patient data meta-analysis might resolve these issues.
PMID: 25501980
[Magnesium and pregnancy]. [Article in Japanese] - Aug 2012
Clin Calcium. 2012 Aug;22(8):1205-10. doi: CliCa120812051210.
Yamasaki M1.
Blood levels of total Mg, ionized Mg and intracellular ionized Mg of platelet were lowered in the 2nd trimester of gestation and thereafter. Urinary excretion of Mg does not change during the whole period of pregnancy. According to our results of animal experiments, intestinal absorption of Mg does not increase during pregnancy compared with non-pregnant state. These data suggest pregnant women tend to become magnesium deficiency . This is reflected in the fact that Mg metabolic parameters of pregnant women with preeclampsia are relatively reduced compared with those of healthy gravidae. In the obstetrical practice Mg has other significance, because magnesium sulfate is frequently used as a drug of choice in the therapy of threatened premature delivery and eclampsia . Mg plays important roles in physiology and pharmacology during gestation.
Magnesium sulphate for preventing preterm birth in threatened preterm labour
Cochraine Aug 2014, 37 included trials
"Magnesium sulphate is ineffective at delaying birth or preventing preterm birth"
". . . (in contrast to its use in appropriate groups of women for maternal, fetal, neonatal and infant neuroprotection where beneficial effects have been demonstrated)."
See also web
Benefits of Magnesium during pregnancy - May 2015
Magnesium While Pregnant: Is it Safe or Dangerous? May 2015
Clips follow
A magnesium deficiency may lead to premature birth
Magnesium naturally works to relax muscles.
Proper magnesium levels may prevent the uterus from contracting prematurely.
Magnesium helps repair tissue.
- This is extremely valuable at a time when your body’s tissue is being pushed to the limits.
Magnesium also helps regulate blood sugar. This can reduce or eliminate those dramatic mood swings.
Magnesium also helps stop leg cramps.
- One heck of a bonus when everything hurts.
Magnesium can also curb nausea which is great for those of us suffering from morning sickness.
Physical and emotional stress associated with pregnancy can deplete magnesium levels in your body.
- Healthy growth of the fetus requires a steady supply of nutrients from the mother.
If a stressful pregnancy is depleting magnesium it’s logical to replace them.
Magnesium acts to optimize your blood pressure.
- This will come in handy when it’s time for delivery.
- Not to mention, there are studies that show magnesium can increase your pain threshold.
Magnesium Sulfate slows or stops preterm labor - 2014
Magnesium Sulfate in Preterm Labor
Updated March 2014 clips follow
"Magnesium sulfate, or mag for short, has been used in pregnancy for over 60 years. Mag was originally used solely to prevent seizures due to worsening preeclampsia, and it is still used for that reason. In modern days, magnesium sulfate is also used to slow or stop preterm labor, and to prevent injuries to the baby's brain."
"Although mag infusions can have a lot of benefits for moms and babies, they aren't fun."
"Magnesium sulfate is commonly used on obstetrical floors, and for good reason. It's a well-studied drug, so doctors know very well how it affects moms and babies. It's also a useful medication, and can be used for these three main reasons:"
Allow time to give steroids
Prevent seizures from eclampsia
Protect the preterm baby's brain
Magnesium Sulfate reduced cerebral palsy in premies - Dec 2013
Magnesium (Sulfate) reduces risk of cerebral palsy for those at risk of pre-term births – Dec 2013
More Magneiusm, half as many pregnancy leg cramps - RCT Aug 2012
Oral magnesium for relief in pregnancy-induced leg cramps: a randomised controlled trial
Chayanis Supakatisant andVorapong Phupong*
Maternal & Child Nutrition, Volume 11, Issue 2, pages 139–145, April 2015
Read at DeepDyve
Leg cramps are common in pregnant women. Currently, there is no standard treatment for pregnancy-induced leg cramps. The objective of this study was to evaluate the therapeutic efficacy of oral magnesium in pregnant women with leg cramps. This double-blinded, randomised, placebo-controlled trial included 86 healthy pregnant women, 14–34 weeks of gestation who had leg cramps at least twice per week. The study period was 4 weeks. Eighty women completed the study. Forty-one women were assigned to magnesium bisglycinate chelate (300 mg per day) and 39 women to placebo. Details of leg cramps were recorded before beginning the treatment and the fourth week of study. Outcome measure was the reduction of cramp frequency after treatment and cramp intensity measured by 100-mm visual analogue scale.
Fifty per cent reduction of cramp frequency was significantly higher in the magnesium group than the placebo group (86.0% vs. 60.5% , P = 0.007). The 50% reduction of cramp intensity was also significantly higher in the treatment group than in the placebo group (69.8% vs. 48.8%, P = 0.048). There were no significant differences between the two groups in terms of side effects such as nausea and diarrhoea. These results demonstrated that oral magnesium supplement can improve the frequency and intensity of pregnancy-induced leg cramps. Therefore, oral magnesium may be a treatment option for women suffering from pregnancy-induced leg cramps.
Magnesium appears to decrease morning sickness
Can You Prevent Morning Sickness? March 2014
Magnesium on my skin has cured me???? 4th HG pregnancy!
- Hyperemesis Gravidarum Support and Research Forums
- Pregnancy Advice Dr Marilyn Glenville
- "Magnesium is a mineral that your body needs to form bone, protein and fatty acids. It relaxes your muscles and helps your blood to clot appropriately. This is a useful mineral if you suffer from leg cramps. Studies show that magnesium levels are lower in women who have had a premature labour."
- "Furthermore, because it has a good effect on muscles, it can help to prevent premature contractions by relaxing the muscles of the womb. Scientists have investigated the effect of giving magnesium during pregnancy and found that women taking magnesium supplements had less chance of having low birthweight and premature babies, and their babies had better Apgar score.Magnesium is known as ‘nature’s tranquilliser’, so it can be invaluable if you are suffering from tension and/or stress. It’s also a good basic treatment for insomnia. Take it as a separate supplement (apart from what is contained in your multivitamin and mineral tablet) for best effect. A total of 200mg per day is the optimum dosage. If you need help with sleeping, take it about an hour before going to bed."
- http://www.babycenter.com/0magnesium-in-your-pregnancy-diet659.bc
- "Signs of a magnesium deficiency include nausea, vomiting, loss of appetite, fatigue, insomnia, muscle twitching, poor memory, irregular heartbeat, and weakness."
- 1 way is Magnesium - click on image for details