Mortality increased with highest levels of vitamin D – article and 4 letters
A Reverse J-Shaped Association of All-Cause Mortality with Serum 25-Hydroxyvitamin D in General Practice: The CopD Study
The Journal of Clinical Endocrinology & Metabolism August 1, 2012 vol. 97 no. 8 2644-2652
D. Durup, H. L. Jørgensen, J. Christensen, P. Schwarz, A. M. Heegaard and B. Lind
Department of Drug Design and Pharmacology (D.D., A.M.H.), Faculty of Health and Medical Sciences, University of Copenhagen, 2100 Copenhagen, Denmark; Department of Clinical Biochemistry (H.L.J.), Bispebjerg Hospital, 2400 Copenhagen, Denmark; Department of Statistics and Epidemiology (J.C.), the Danish Cancer Society, 2100 Copenhagen Denmark; Research Center of Aging and Osteoporosis (P.S.), Department of Medicine, Glostrup University Hospital and Faculty of Health and Medical Sciences, University of Copenhagen, 2200 Copenhagen, Denmark; and Copenhagen General Practitioners Laboratory (B.L.), 1112 Copenhagen, Denmark
Address all correspondence and requests for reprints to: Anne-Marie Heegaard, Department of Drug Design and Pharmacology, Faculty of Health and Medical Sciences, University of Copenhagen. 2100 Universitetsparken 2, Copenhagen, Denmark. E-mail: amhe@farma.ku.dk.
Context: Optimal levels of vitamin D have been a topic of heavy debate, and the correlation between 25-hydroxyvitamin D [25(OH)D] levels and mortality still remains to be established.
Objective: The aim of the study was to determine the association between all-cause mortality and serum levels of 25(OH)D, calcium, and PTH.
Design and Setting: We conducted a retrospective, observational cohort study, the CopD Study, in a single laboratory center in Copenhagen, Denmark.
Participants: Serum 25(OH)D was analyzed from 247,574 subjects from the Copenhagen general practice sector. In addition, serum levels of calcium, albumin-adjusted calcium, PTH, and creatinine were measured in 111,536; 20,512; 34,996; and 189,496 of the subjects, respectively.
Main Outcome Measures: Multivariate Cox regression analysis was used to compute hazard ratios for all-cause mortality.
Results: During follow-up (median, 3.07 yr), 15,198 (6.1%) subjects died. A reverse J-shaped association between serum level of 25(OH)D and mortality was observed. A serum 25(OH)D level of 50–60 nmol/liter was associated with the lowest mortality risk. Compared to 50 nmol/liter, the hazard ratios (95% confidence intervals) of all-cause mortality at very low (10 nmol/liter) and high (140 nmol/liter) serum levels of 25(OH)D were 2.13 (2.02–2.24) and 1.42 (1.31–1.53), respectively. Similarly, both high and low levels of albumin-adjusted serum calcium and serum PTH were associated with an increased mortality, and secondary hyperparathyroidism was associated with higher mortality (P < 0.0001).
Conclusion: In this study from the general practice sector, a reverse J-shaped relation between the serum level of 25(OH)D and all-cause mortality was observed, indicating not only a lower limit but also an upper limit. The lowest mortality risk was at 50–60 nmol/liter. The study did not allow inference of causality, and further studies are needed to elucidate a possible causal relationship between 25(OH)D levels, especially higher levels, and mortality.
Received January 23, 2012, Accepted April 18, 2012, Copyright © 2012 by The Endocrine Society
Published again in March 2015 - cardio mortality instead of all cause mortality, with 3 more authors
📄 Download the PDF from VitaminDWiki
Wonder if Danes get a lot of Vitamin A in cod liver oil
Vitamin A interferes with vitamin D and may be the cause of U shaped relationships – April 2014
Vitamin A is #6 in the following
Is too much vitamin D bad – possible causes and cures
Note: Vitamin A can block the Vitamin D receptor
Comparing the abstracts we find the following to be strange:
Exact same number of people in the database: 247,574
High level of Calcium increased all-cause mortality, but was not mentioned in cardio mortality
Vitamin D Council notes that only Nordic countries find this association - May 2012
High and low vitamin D levels cause mortality?
". . .Cochrane review, the preformed vitamin A, as in cod liver oil, is associated with excess mortality"
The Findings May Be Due To Late-Life Vitamin D Supplementation by Women
William B. Grant, Researcher David A. McCarthy
Sunlight, Nutrition and Health Research Center
The recent paper by Durup and colleagues found a J-shaped relation between serum 25-hydroxyvitamin D [25(OH)D] concentrations and all-cause mortality rates (1). While not unprecedented, this result is nonetheless surprising given the benefits of vitamin D in reducing the risk of many types of cancer, cardiovascular disease, infectious diseases, and other diseases associated with large numbers of deaths in Denmark (2).
One reason for this finding may be that women, who comprise 71.2-73.7% of those with serum 25(OH)D concentrations above 75 nmol/liter, are more likely than men to be diagnosed with low bone mass density and instructed by their physician to take supplemental vitamin D. Since many of the vitamin D-sensitive diseases are long-latency diseases, these diseases could be progressing due to low serum 25(OH)D concentrations earlier in life. Some of the effects, such as calcification of the arteries, may not be reversed through increasing serum 25(OH)D concentrations. This hypothesis is supported by two studies of the association of serum 25(OH)D concentrations with frailty status in the United States. For men, there was a monotonic decrease in frailty status with increasing serum 25(OH)D concentrations (3), while for women, there was a minimum in frailty status near 57 nmol/liter, with much higher frailty status near 12 nmol/liter and 150 nmol/liter (4). Ensrud et al. (4) considered the possibility that "fail women might be preferentially prescribed vitamin D supplements and thus have higher levels". This possibility could not be ruled out. Thus, it would be interesting to see the analyses in (1) repeated separately for men and women.
Regarding the discussion in Durup et al. (1) of U-shaped 25(OH)D-all-cause mortality rate findings, a recent meta-analysis of 11 such studies found an apparent minimum mortality rate near 80 nmol/liter (5). However, the upper 95% confidence interval of the relation at 80 nmol/liter in Figure 4 was higher than the regression fit at 115 nmol/liter. Thus, in general, these 11 all-cause mortality rate studies do not find a significant U-shaped 25(OH)D-all-cause mortality rate relation.
A concern with the Copenhagen study is that in clinical practice, when patients are found to have low have 25(OH)D concentrations, they are usually placed on vitamin D supplements to improve their status. Patients who have 25(OH)D levels in the sufficient range are much less likely to go on supplemental vitamin D. It is likely that the 2-3 year mortality in the group with low 25(OH)D is significantly underestimated as they would have had 2-3 years benefit of being on additional vitamin D, while the group with the better 25(OH)D concentrations is more likely appropriately represented in the study data as they are much less likely to have been placed on the supplement. Since the study was retrospective and the patients along with their providers were aware of the findings, the low range patients would have been managed upward potentially reducing their mortality range in the near term. If true, this would mean that the curve would be much higher in the low range and about the same in the upper range.
References
Durup D, Jorgensen HL, Christensen J, Schwarz P, Heegaard AM, Lind B. 2012 A reverse J-shaped association of all-cause mortality with serum 25-hydroxyvitamin D in general practice, the CopD Study. J Clin Endocrinol Metab. 2012 May 9. [Epub ahead of print]
Grant WB 2011 An estimate of the global reduction in mortality rates through doubling vitamin D levels. Eur J Clin Nutr 65:1016-1026
Ensrud KE, Blackwell TL, Cauley JA, Cummings SR, Barrett-Connor E, Dam TT, Hoffman AR, Shikany JM, Lane NE, Stefanick ML, Orwoll ES, Cawthon PM; Osteoporotic Fractures in Men Study Group 2011 Circulating 25- hydroxyvitamin D levels and frailty in older men: the osteoporotic fractures in men study. J Am Geriatr Soc 59:101-106
Ensrud KE, Ewing SK, Fredman L, Hochberg MC, Cauley JA, Hillier TA, Cummings SR, Yaffe K, Cawthon PM; Study of Osteoporotic Fractures Research Group 2010 Circulating 25-hydroxyvitamin D levels and frailty status in older women. J Clin Endocrinol Metab 95:5266-5273.
Zittermann A, Iodice S, Pilz S, Grant WB, Bagnardi V, Gandini S 2012 Vitamin D deficiency and mortality risk in the general population: A meta- analysis of prospective cohort studies. Am J Clin Nutr 95:91-100.
Conflict of Interest: WBG receives funding from the UV Foundation (McLean, VA), Bio-Tech Pharmacal (Fayetteville, AR), the Vitamin D Council (San Luis Obispo, CA), and the Vitamin D Society (Canada). DAM is a clinician who does not receive any outside funding and has no conflicts of interest to report.
Response to Grant Letter
Darshana Durup H. L. Jørgensen, J. Christensen, P. Schwarz, A. M. Heegaard and B. Lind
University of Copenhagen
We appreciate the thoughtful comments from Dr. Grant regarding the reverse J-shaped association between vitamin D and mortality risk. Our study showed an increased morality risk with serum 25-hydroxyvitamin D [25(OH)D] levels below 50 nmol/liter (1).
Additionally, we observed an increased mortality risk with higher serum levels of 25(OH)D. Not many studies have found a U- or reverse J-shape in comparable studies, but our approach of analyzing the data is different from that in most of these other studies. The design of many studies does not allow for analyzing the very low and very high levels of 25(OH)D, because they compare reference values with 1 to 4 categories. To see the real shape of the curve, we believe that the data need to be analyzed either by a cubic spline analysis or by dividing the 25(OH)D levels into categories where the extreme values are apparent, since the association between vitamin D status and mortality might be driven by individuals in the very low and high levels of 25(OH)D as we state in our paper. However, this may not always be possible, since it may require a large sample size, with sufficient observations at the extremes.
Finally, the hypotheses applied by Dr. Grant are interesting, but at this point we cannot confirm or refute any of the speculations . We sincerely hope that we and other research groups could bring more answers to the table in near future.
Reference
1 Durup D, Jorgensen HL, Christensen J, Schwarz P, Heegaard AM, Lind B. 2012 A reverse J-shaped association of all-cause mortality with serum 25-hydroxyvitamin D in general practice, the CopD Study. J Clin Endocrinol Metab. 2012 May 9.
Cautious Interpretation of the Reverse J-shaped Association between Circulating 25-Hydroxyvitamin D and Total Mortality is Necessary
Armin Zittermann, Head of Study Center
Clinic for Thoracic and Cardiovascular Surgery, Heart & Diabetes Center NRW, Ruhr University Bochum,
The study by Durup et al. (1) adds to the growing evidence of an inverse J-shaped association between circulating 25-hydroxyvitamin D and total mortality. However, almost all of these studies fell short of measuring the active vitamin D metabolite 1,25-dihydroxyvitamin D. In a former study in patients of a specialist heart center (2), we demonstrated a consistent decline in 1-year mortality with higher 1,25- dihydroxyvitamin D levels, but only a non-significant trend toward an association between 25-hydroxyvitamin D quintile and 1-year mortality.
A re-analysis of these earlier data according to 25-hydroxyvitamin D cut-off values used by Durup et al. (<25, 25-50, 50-75, 75-100,100-125, >125 nmol/liter) also indicates an inverse J-shaped association between circulating 25-hydroxyvitamin D category and 1-year mortality incidence (
category 1 [n = 178]: 25.3%;
category 2 [n = 177]: 13.0%;
category 3 [n = 70]: 11.4%;
category 4 [n = 33]: 9.1%;
category 5 [n = 23]: 0.0%;
category 6 [n = 29]: 10.3% , respectively).
Mean [SD] circulating 1,25-dihydroxyvitamin D levels in the aforementioned 25-hydroxyvitmin D categories were as follows (in pmol/l): (category 1: 67.1[40.1]; category 2: 74.2 [36.9]; category 3: 87.1[48.6]; category 4: 104.5[67.6]; category 5: 101.4[47.1]; category 6: 87.8[41.1], respectively), indicating that very high 25-hydroxyvitamin D levels may sometimes reflect low availability of the active vitamin D hormone. This assumption is in line with experimental data (3) demonstrating that high circulating 25-hydroxyvitamin D levels can be the result of low renal 1?-hydroxylase activity. Moreover, it has recently been shown that compared to younger cardiac surgical patients, older patients do not only have reduced 1,25-dihydroxyvitamin D levels but also have significantly higher circulating 25-hydroxyvitamin D levels (4).
Potential health benefits of vitamin D are currently hotly debated. Our data demonstrate that it is absolutely necessary to measure both , 25-hydroxyvitamin D and 1,25-dihydroxyvitamin D, before any conclusions from epidemiological studies about harmful vitamin D effects can be drawn.
References
Durup D, Jorgensen HL, Christensen J, Schwarz P, Heegaard AM, Lind B 2012 A Reverse J-Shaped Association of All-Cause Mortality with Serum 25 -Hydroxyvitamin D in General Practice, the CopD Study J Clin Endocrinol Metab doi:10.1210/jc.2012-1176
Zittermann A, Schleithoff SS, Frisch S, Gotting C, Kuhn J, Koertke H, Kleesiek K, Tenderich G, Koerfer R 2009 Circulating calcitriol concentrations and total mortality. Clin Chem 55: 1163-1170
Vieth R, Fraser D, Kooh SW 1987 Low dietary calcium reduces 25-hydroxycholecalciferol in plasma of rats. J Nutr 117: 914-918
Borgermann J, Lazouski K, Kuhn J, Dreier J, Schmidt M, Gilis-Januszewski T, Knabbe C, Gummert JF, Zittermann A 2012 1,25- Dihydroxyvitamin D Fluctuations in Cardiac Surgery Are Related to Age and Clinical Outcome. Crit Care Med 40, in press
Conflict of Interest: I have received speaker honoraria from DiaSorin, Germany, and Abbott, Germany.
Response to Zitterman Letter
Darshana Durup H. L. Jørgensen, J. Christensen, P. Schwarz, A. M. Heegaard and B. Lind
University of Copenhagen
We thank Dr. Zitterman and colleagues for taking the time to re-analyze their data according to the cut-off values used in our study. It is very interesting that they found indications of reverse J-shaped association after doing this. This confirms the importance of how these studies are analyzed, since the association between vitamin D status and mortality might be driven by values in the very low and high levels of 25-hydroxyvitamin D [25(OH)D] as we state in our paper (1).
In a recent comprehensive study by Saliba et al. (2) on vitamin D and mortality risk, the 50-75 nmol/liter category was associated with the lowest mortality risk but not the upper category (?75nmol). Unfortunately, the lower and upper categories were predefined to 25(OH)D <30 nmol/liter and ?75nmol, respectively, leaving no information on the effects at the extreme levels.
References
Durup D, Jorgensen HL, Christensen J, Schwarz P, Heegaard AM, Lind B. A reverse J-shaped association of all-cause mortality with serum 25-hydroxyvitamin D in general practice, the CopD Study. J Clin Endocrinol Metab.
Saliba W, Barnett O, Rennert HS, Rennert G. The risk of all-cause mortality is inversely related to serum 25(OH)D levels. J Clin Endocrinol Metab.
See also VitaminDWiki
Vitamin A interferes with vitamin D and may be the cause of U shaped relationships – April 2014
Vitamin D3 but not D2 reduces mortality – meta-analysis July 2011
- wonder if the current study included results from use of Vitamin D2
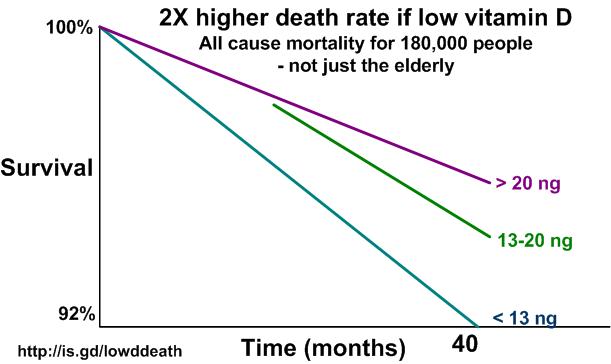
Mortality and vitamin D – great chart which follows

- Death rate 2X higher if low vitamin D - 180,000 adults, not just elderly – May 2012 which has the following chart