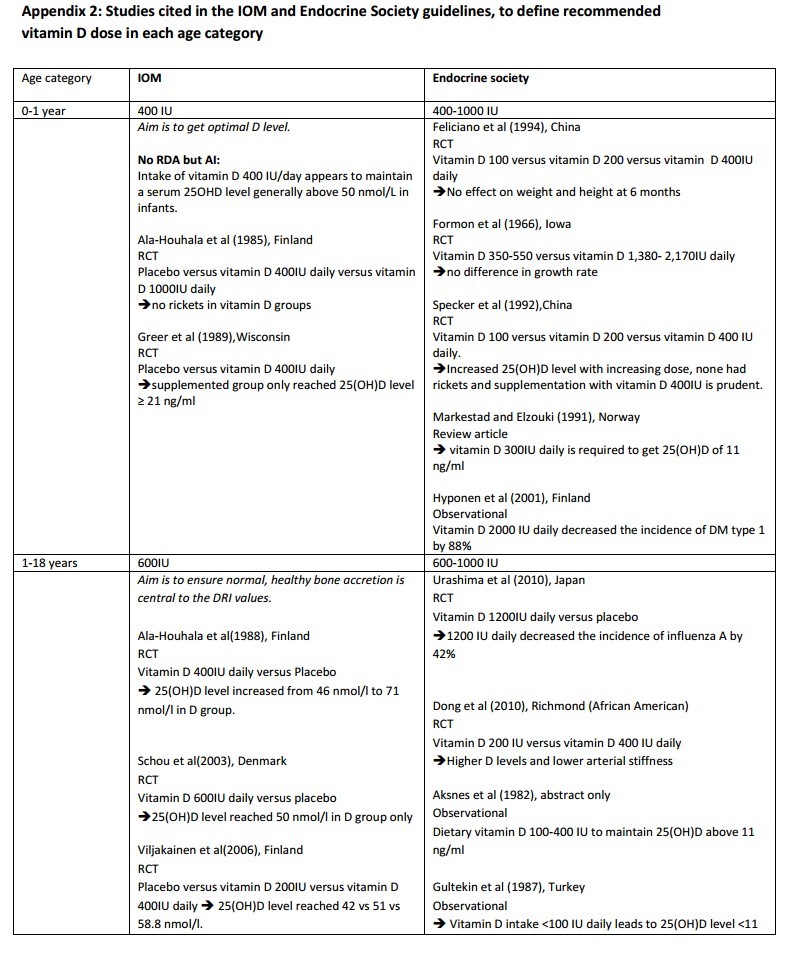
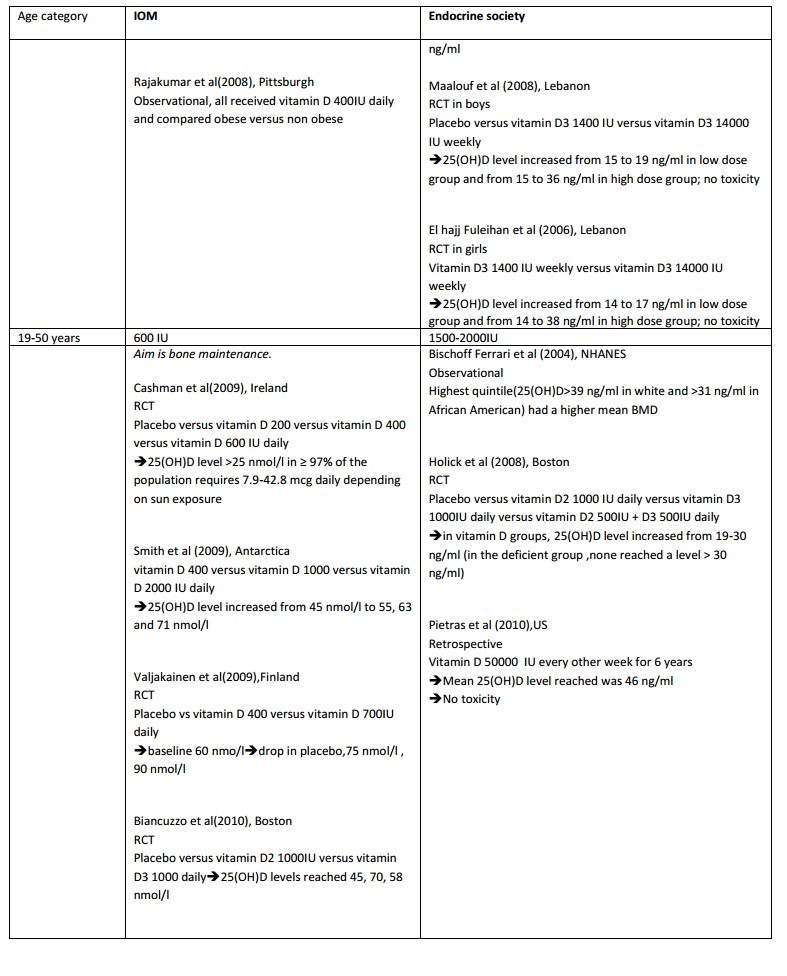
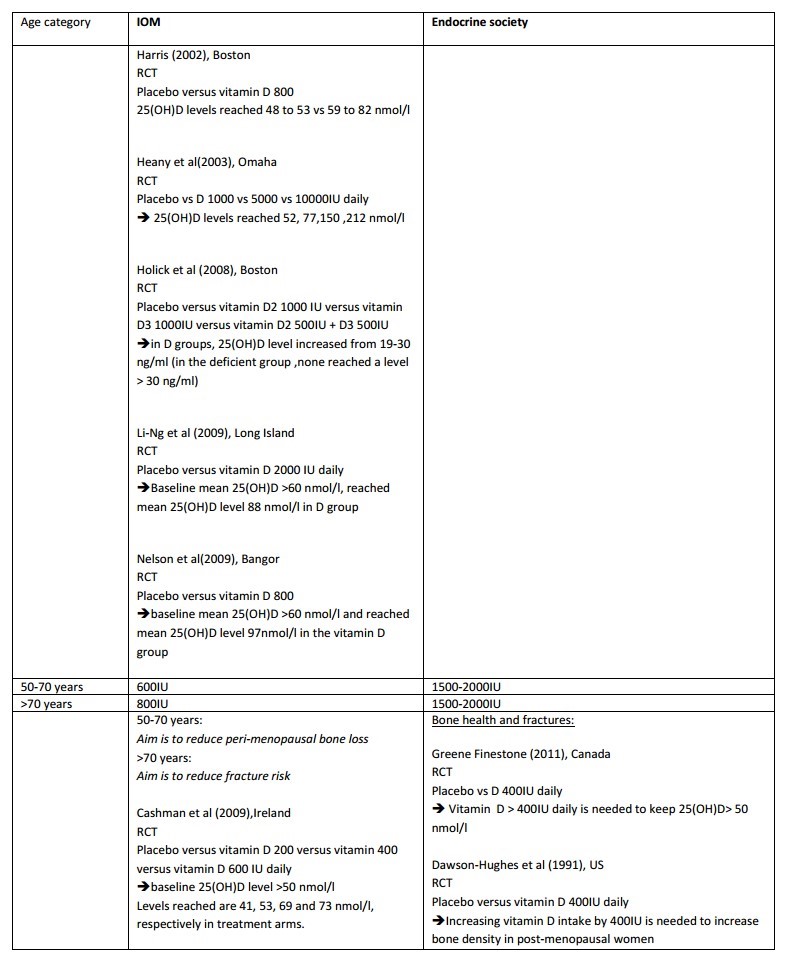
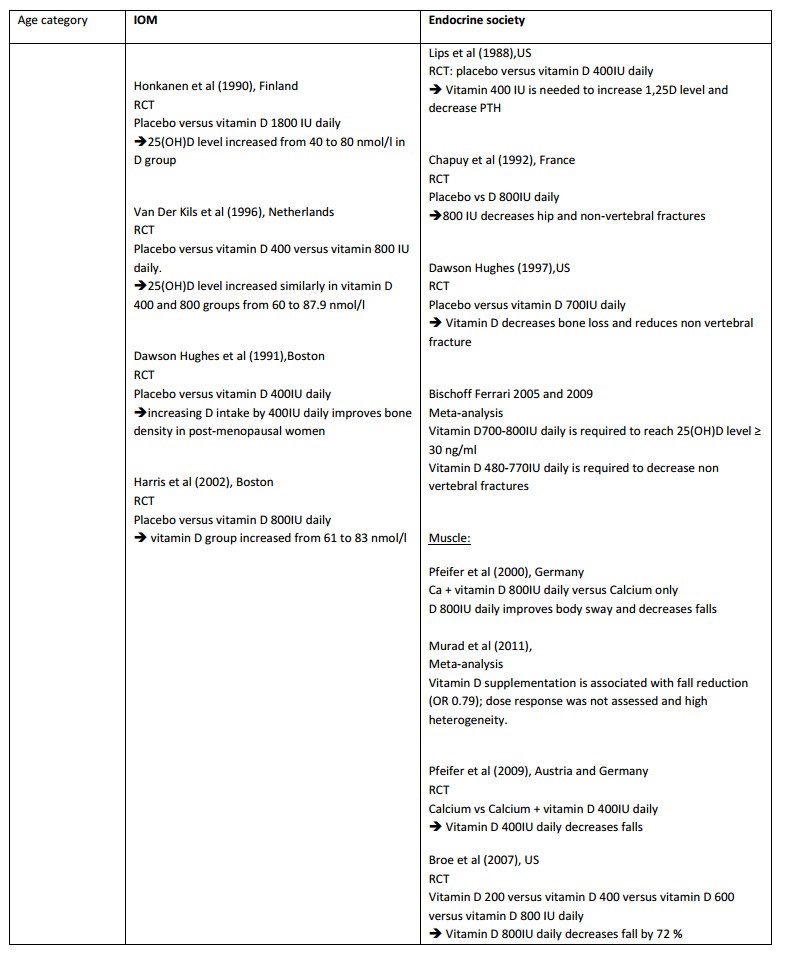
Vitamin D levels vs age: compares references by IOM and Endocine Society – MENA study 2014
Effects of Different Doses of Vitamin D Replacement in Middle Eastern and North African Population: a Systematic Review and Meta-analysis.
Chakhtoura M, Akl EA, Arabi A, El Ghandour S, Shawwa K, El Hajj Fuleihan G.
Background:
Countries in the Middle East and North Africa (MENA) register some of lowest vitamin D levels worldwide. Yet, the optimal dose of vitamin D required to reach desirable serum 25- hydroxyvitamin D (25(OH)D) levels in populations from this region is unknown.
Objectives:
The main objective is to define the mean 25(OH)D level reached with low (<800IU), moderate (800-2,000IU) or high (>2,000 IU) daily dose of vitamin D in subjects in the MENA countries, by age and reproductive status. We will also deduce the mean serum 25(OH)D level reached by 97.5% of individuals in above treatment groups, as well as the proportion of subjects who reach a mean 25(OH) D level >20 ng/ml in the three above treatment groups.
Other outcomes investigated are fracture rate, fall and imbalance rate, kidney stones rate, hypercalcemia-hypercalciuria, hyperparathyroidism, metabolic parameters (diabetes and lipids), bone mineral density, muscle strength, mortality.
Materials and methods:
Data sources:
A search for English and Non-English articles will be done using Medline, PubMed, the Cochrane Controlled Trials Register, EMBASE, Popline and Index Medicus and Global Health Library without any time restriction. We will also search ClinicalTrial.gov and the WHO International Clinical Trials Registry (ICTRP) to try to retrieve unpublished or preliminary data by directly contacting the authors. In addition, references listed in recently published reviews will be screened. Vitamin D experts will be also contacted.
Study selection:
Only randomized controlled trials of oral vitamin D supplementation (cholecalciferol, ergocalciferol) with or without calcium supplementation, versus calcium supplementation or placebo, or those comparing different doses of vitamin D, conducted on community dwelling individuals in MENA countries, will be included.
Data Extraction:
Duplicate and independent data extraction will be done using predefined data fields, including study quality indicators. Discrepancies will be solved by discussion, and when unsuccessful by an expert author.
Risk of bias:
Risk of bias assessment will be done on all included studies, by 2 reviewers in duplicate and independently, using the Cochrane Collaboration's Risk of Bias tool 2011.
Summary measures:
Continuous outcomes will be expressed as mean differences (MD) with 95% confidence interval (CI). Dichotomous outcomes will be expressed as risk ratio (RR) and hazard ratio (HR) with 95% CI.
Primary analysis and additional analysis:
The primary analysis will be done using a random-effects model.
Additional pre-specified subgroup analysis and sensitivity analysis will be done according to gender, type of vitamin D (D2 or D3), vitamin D assay, use or not of calcium supplementation and BMI. Sensitivity analysis, if applicable, will be done, restricting the analysis to published trials, MENA individuals living in MENA countries exclusively and trials with mean baseline 25(OH)D < 20ng/ml.
Risk of bias across the studies:
Publication bias and bias due to selective outcome reporting will be assessed using a funnel plot and Egger's test.
PDF is attached at the bottom of this page