Vitamin D – individual responses to 100,000 IU
Impact of a single oral dose of 100,000 IU vitamin D3 on profiles of serum 25(OH)D3 and its metabolites 24,25(OH)2D3, 3-epi-25(OH)D3, and 1,25(OH)2D3 in adults with vitamin D insufficiency
Clinical Chemistry and Laboratory Medicine (CCLM) .Online: 2017-03-22 |
DOI: https://doi.org/10.1515/cclm-2016-1129
Blood level Vitamin D - before and 4 weeks after oral dose
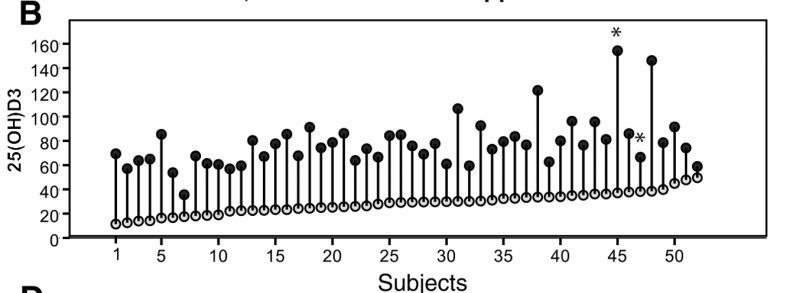
52% achieved levels > 30 ng; approximate 20 ng increase - with lots of variability
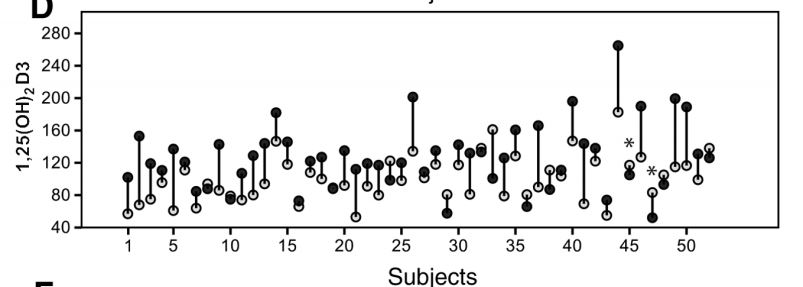
Active Vitamin D - before and 4 weeks after oral dose
 Reasons for low response to vitamin D ~40 reasons
Overview Loading of vitamin D has the following
Response to a single dose of 100,000 IU starting at 27 ng/ml, half life is about 50 days
Reasons for low response to vitamin D ~40 reasons
Overview Loading of vitamin D has the following
Response to a single dose of 100,000 IU starting at 27 ng/ml, half life is about 50 days
 People in this study were not obese - obese would have has lower responses
{include}
Click here for 2014 study
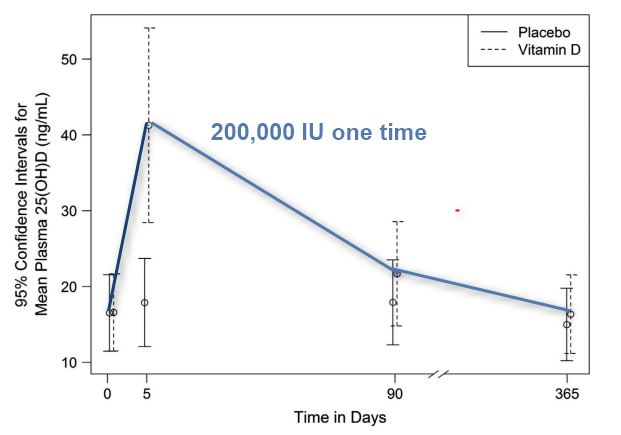
1. Large dose of vitamin D (200,000 IU) lasts for less than 90 days – Feb 2015
200,000 IU
People in this study were not obese - obese would have has lower responses
{include}
Click here for 2014 study
1. Large dose of vitamin D (200,000 IU) lasts for less than 90 days – Feb 2015
200,000 IU
📄 Download the PDF from VitaminDWiki
Background:
We investigate the effect of a high dose of vitamin D3 on circulating concentrations of 25(OH)D3 and its metabolites 24,25(OH)2D3, 3-epi-25(OH)D3, and 1,25(OH)2D3 in healthy individuals with self-perceived fatigue and vitamin D insufficiency [25(OH)D3<50 nmol/L].
Methods:
One hundred and seven study participants (age 20–50 years) were randomized to receive a single 100,000 IU dose of vitamin D3 (n=52) or placebo (n=55). Vitamin D metabolite concentrations in serum were measured before, and 4 weeks after, supplementation.
Results:
Overall, 52% of participants receiving vitamin D3 attained a serum 25(OH)D3 level >75 nmol/L. Among individuals who received vitamin D3, there were significant increases in serum concentrations of 25(OH)D3 and its metabolites 24,25(OH)2D3, 3-epi-25(OH)D3, and 1,25(OH)2D3 at 4 weeks; however, inter-individual variability in these changes was substantial. Positive correlations between serum 25(OH)D3 and 24,25(OH)2D3 and 3-epi-25(OH)D3, and a significant negative correlation between serum 1,25(OH)2D3 and 3-epi-25(OH)D3, were found 4 weeks after supplementation. The 24,25(OH)2D3/25(OH)D3 and 24,25(OH)2D3/1,25(OH)2D3 ratios were significantly increased, compared with baseline, in participants receiving vitamin D3. Baseline 25(OH)D3 concentration was the only factor predictive of the change in 25(OH)D3 after supplementation.
Conclusions:
Administration of a single high dose of vitamin D3 leads to a significant increase in concentrations of 25(OH)D3, 24,25(OH)2D3, 3-epi-25(OH)D3 and 1,25(OH)2D3; induction of the catabolic pathway predominates over the production of 1,25(OH)2D3. Due to the high inter-individual variation in the 25(OH)D3 response to supplementation, any given dose of vitamin D is unlikely to achieve optimal vitamin D status in all treated individuals