Some food preservatives increase hypertension by ~30% (Vitamin D might reduce the %)
Summary. A large French prospective cohort (NutriNet-Santé, 112,395 adults) found that higher intake of common food preservatives tracked with ~29% higher new-onset hypertension and ~16% higher cardiovascular disease (CVD). The study did not measure vitamin D. This page lays out the finding and then proposes — as a testable hypothesis, not as a result of this study — that good vitamin D status may blunt the blood-pressure portion of that harm through suppression of the renin-angiotensin system, while being explicit about why vitamin D cannot reduce the preservatives a food actually needs to stay safe.
Key points
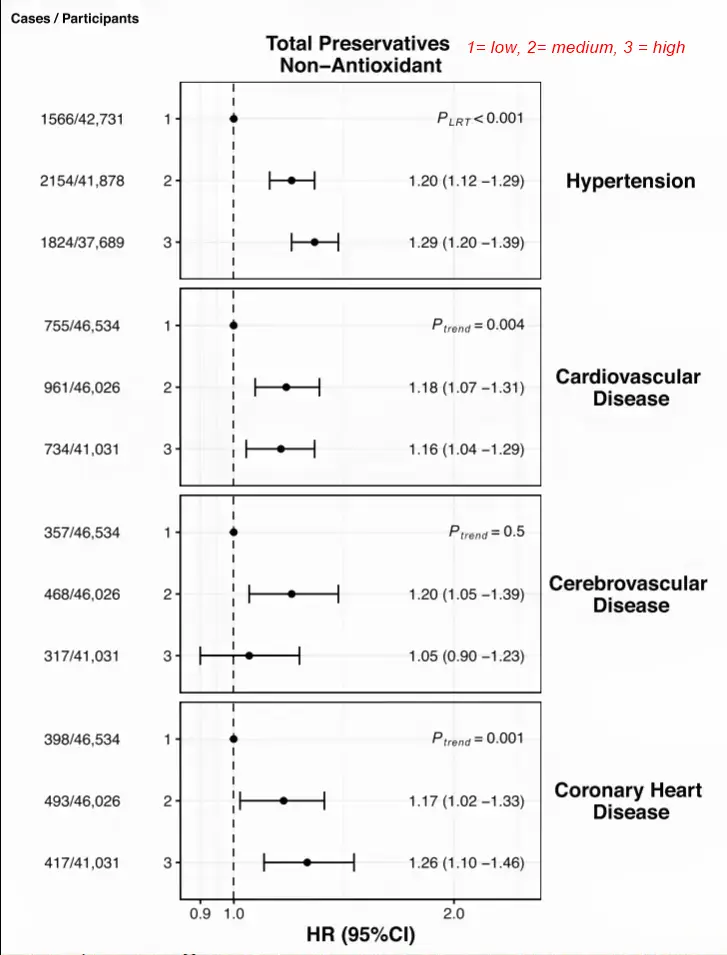
- The 30% figure is a hazard ratio of 1.29 for hypertension (not heart rate, and not CVD).
- The CVD signal was smaller: hazard ratio ~1.16 (about 16% higher incidence).
- The study is observational — association, not proven causation.
- Vitamin D was not a variable in this study. Any vitamin D effect here is inferred mechanism, not measured.
- A food's preservative requirement is set by microbiology and shelf life, not by the eater. Vitamin D cannot lower the dose a product needs.
- Best current framing: vitamin D status and preservative reduction are most likely two independent, additive levers on blood pressure and CVD risk, possibly sharing a final common pathway (renin / endothelium / inflammation) — not substitutes for each other.
- Separate phosphate mechanism: inorganic phosphate additives (very widely consumed here) raise FGF23, which suppresses CYP27B1 and induces CYP24A1, lowering active vitamin D — a reason to limit them, but not a case where more vitamin D is cleanly protective (calcitriol raises phosphate absorption).
What the study found
The French NutriNet-Santé cohort followed 112,395 adults (mean age ~43, about 79% women, none with hypertension or CVD at baseline) from 2009 to 2024, with repeated 24-hour dietary records every six months that captured commercial brand information and laboratory assays of food matrices. Preservative exposure was essentially universal: ~99.5% of participants consumed at least one. The sum of total preservatives covered 58 substances; 17 were common enough (eaten by at least 10% of the cohort) to study individually.
Main associations (multivariable-adjusted Cox models, highest vs. lowest consumers):
| Exposure | Outcome | Hazard ratio (95% CI) | Approx. risk increase |
|---|---|---|---|
| Total non-antioxidant preservatives | Hypertension | 1.29 (1.20–1.39) | ~29% |
| Total non-antioxidant preservatives | CVD | 1.16 (1.04–1.29) | ~16% |
| Total antioxidant preservatives | Hypertension | 1.22 (1.13–1.31) | ~22% |
Of the 17 individually examined additives, 8 were associated with higher hypertension incidence and 1 with higher CVD incidence after multiple-test correction. The named individual offenders for hypertension include potassium sorbate (E202, ~+39%), citric acid (E330, ~+25%), and sodium nitrite. At the chemical-group level, nitrites (used mainly in processed meats) were associated with higher hypertension, while nitrates showed no association.
The authors also extracted preservative mixtures. None of the mixtures reached significance for CVD, but two were associated with higher hypertension incidence — including Mixture 3, characterized mainly by citric and phosphoric acids, sodium nitrite, sodium erythorbate, and potassium sorbate. This is the entry point for the phosphate-axis discussion below.
Limitations stated by the authors / reviewers. The design is observational and cannot establish cause and effect; the cohort skews female and higher-education; there was roughly 12% dropout; and some additive exposures may be misclassified. Higher-preservative consumers may differ systematically from lower consumers in ways that themselves raise cardiovascular risk.
Why preservatives might raise blood pressure and CVD risk
Several non-exclusive mechanisms are plausible:
- Sodium load. Many implicated preservatives are sodium salts (e.g., sodium nitrite, sodium benzoate). Sodium independently raises blood pressure.
- Renin-angiotensin (RAAS) activation and impaired vascular tone.
- Oxidative stress and low-grade inflammation.
- Endothelial dysfunction.
- Gut-microbiome disruption (relevant for emulsifier- and additive-rich diets).
Note that high preservative intake is, in practice, a marker of ultra-processed food (UPF) consumption, so part of the signal may reflect the broader UPF diet pattern rather than the additives in isolation.
Where vitamin D plausibly intersects — hypothesis, not finding
The overlap is strongest for the hypertension arm, and specifically for the sodium/RAAS-mediated portion of it:
- Renin suppression (the strongest link). Calcitriol [1,25(OH)2D] is a direct negative transcriptional regulator of the renin gene. A vitamin D-sufficient person therefore runs a structurally down-tuned renin-angiotensin axis — the same axis that sodium-bearing preservatives tend to push upward. This is a blood-pressure-specific point of leverage.
- Endothelial and anti-inflammatory effects. VDR is expressed in endothelium, vascular smooth muscle, and cardiomyocytes; vitamin D signaling supports endothelial function and dampens inflammatory tone.
- Gut-barrier integrity. If part of the additive harm is microbiome- or barrier-permeability-mediated, vitamin D's support of intestinal barrier function is a candidate buffer.
For the non-sodium, non-RAAS mechanisms (specific additive toxicity, particular microbiome shifts), the vitamin D overlap is weak or simply unknown — not established as protective.
The phosphate-additive link — a different vitamin D mechanism (FGF23 / CYP24A1)
Phosphoric acid (E338) appears in the hypertension-associated Mixture 3 above, and inorganic phosphate additives are among the most consumed substances in this cohort (phosphoric acid plus di-, tri- and polyphosphates [E450–E452] reach roughly 70% of participants). In the same group's companion diabetes analysis, phosphoric acid was one of the individual preservatives associated with higher diabetes incidence. So phosphate additives are a real, high-prevalence exposure in this population — and they connect to vitamin D through a mechanism entirely separate from the renin story.
The key biology:
- Additive phosphate is unusually bioavailable. Phosphate naturally bound in whole foods is only partly absorbed (~40–60%), but the inorganic phosphate added as a preservative/stabilizer is absorbed at ~90%+. A processed-food diet therefore delivers a large, "hidden" phosphate load that intake estimates based on whole-food phosphorus badly underestimate.
- High phosphate load raises FGF23. Osteocyte-derived fibroblast growth factor 23 rises in response to a phosphate challenge.
- FGF23 actively lowers active vitamin D. It suppresses renal CYP27B1 (1α-hydroxylase), cutting calcitriol production, and induces CYP24A1 (24-hydroxylase), accelerating calcitriol catabolism. Net effect: less 1,25(OH)2D. (This is the same CYP24A1 up-regulation step relevant to the curcumin/CYP24A1 work.)
- Elevated FGF23 is independently cardiotoxic. Higher FGF23 is associated with left ventricular hypertrophy (and can induce it directly, via FGF23 signaling in cardiomyocytes independent of Klotho), with vascular calcification, and with cardiovascular events and mortality across CKD and general-population cohorts.
Why this cuts differently from the renin story. In the sodium/RAAS arm, good vitamin D status is plausibly protective (it down-tunes renin). In the phosphate arm, the additive itself may be suppressing the active vitamin D pathway via FGF23 — so the harm and low active vitamin D move together, and the cleaner lever is reducing inorganic phosphate-additive intake, not raising vitamin D.
An important caution against over-claiming vitamin D here. Calcitriol increases intestinal phosphate absorption (via NaPi-IIb). So on the phosphate arm specifically, high vitamin D is not unambiguously protective and could, in principle, add to phosphate load. The phosphate–FGF23–vitamin D loop is bidirectional, and this page should not be read as claiming that more vitamin D offsets phosphate-additive harm. The defensible statement is narrower: phosphate additives may erode the active vitamin D pathway through FGF23/CYP24A1, which is one more reason to limit them — distinct from, and not symmetric with, the renin-mediated hypertension hypothesis.
Three reasons this is a hypothesis, not a conclusion
- Vitamin D was never measured or stratified in NutriNet-Santé's preservative analysis. Any interaction is inferred from mechanism, not observed.
- The confounding runs the wrong way for "tolerance." High preservative intake is a UPF marker, and heavy UPF consumers tend to be vitamin D deficient (less sun exposure, poorer diet quality). In the population the two exposures travel together — the opposite of "more vitamin D lets you tolerate more preservative."
- Food still needs its preservatives. How much preservative a product requires is fixed by water activity, pH, fat content, packaging, and target shelf life — i.e., by microbiology, not by who eats it. A vitamin D-replete person does not change a product's spoilage curve, so vitamin D cannot reduce the preservative load a food needs to remain safe.
The testable claim (research gap)
The defensible, falsifiable version of this page's thesis:
In a cohort with both detailed additive-exposure data and serum 25(OH)D — NutriNet-Santé itself, or a comparable cohort — an effect-modification (interaction) analysis would test whether the preservative–hypertension association is attenuated in vitamin D-sufficient participants relative to deficient ones. A significant interaction on the blood-pressure outcome (and a null or weaker one on non-RAAS endpoints) would support partial mitigation via the renin pathway.
Until such an analysis exists, the honest position is: plausible for the blood-pressure arm, mechanistically grounded in renin suppression, but unproven.
Bottom line
Reducing preservative/UPF intake and maintaining good vitamin D status are best understood as independent, additive ways to lower blood-pressure and CVD risk. Vitamin D may sit on a shared final pathway (renin, endothelium, inflammation) such that a replete person absorbs somewhat less of the damage from an exposure they cannot fully avoid — but good vitamin D does not license a higher preservative intake, and it does not reduce the preservatives a food itself requires.
References
Hasenböhler A, Javaux G, Payen de la Garanderie M, et al. Preservative food additives, hypertension, and cardiovascular diseases: the NutriNet-Santé study. European Heart Journal, May 2026. doi:10.1093/eurheartj/ehag308
Supporting mechanism (vitamin D and renin): Li YC, Kong J, Wei M, et al. 1,25-Dihydroxyvitamin D3 is a negative endocrine regulator of the renin-angiotensin system. J Clin Invest. 2002;110(2):229-238.
Supporting mechanism (phosphate / FGF23 / vitamin D catabolism): Shimada T, Hasegawa H, Yamazaki Y, et al. FGF-23 is a potent regulator of vitamin D metabolism and phosphate homeostasis. J Bone Miner Res. 2004;19(3):429-435.
Supporting mechanism (FGF23 and cardiac hypertrophy): Faul C, Amaral AP, Oskouei B, et al. FGF23 induces left ventricular hypertrophy. J Clin Invest. 2011;121(11):4393-4408.
Supporting context (bioavailability and public-health impact of phosphate additives): Calvo MS, Uribarri J. Public health impact of dietary phosphorus excess on bone and cardiovascular health in the general population. Am J Clin Nutr. 2013;98(1):6-15.
Companion analysis (phosphoric acid and diabetes): NutriNet-Santé preservative–type 2 diabetes analysis, Hasenböhler/Touvier group (Diabetes Care / European Journal of Epidemiology, 2025–2026) doi: 10.1038/s41467-025-67360-w. PDF
Related in VitaminDWiki
- Ultra-Processed Food problems are fought by Vitamin D, Berberine, and Glutathione
- Ultra-processed food health problems reduced by Liposomal Glutathione
- If you eat ultra-processed foods, you need Vitamin D
- Phosphate, Phosphatonins reduce active Vitamin D - many studies
- Cola Soft Drinks reduce Calcium, Vitamin D, and Magnesium - many studies