Preterm birth 9 X more likely if fetus had a poor Vitamin D Receptor and previous miscarriage
Maternal-fetal vitamin D receptor polymorphisms significantly associated with preterm birth.
Arch Gynecol Obstet. 2017 Aug;296(2):215-222. doi: 10.1007/s00404-017-4412-y
Study PDF can be viewed on Deepdyve
Rosenfeld T1,2, Salem H1, Altarescu G2, Grisaru-Granovsky S2, Tevet A2, Birk R3.
1 Department of Nutrition, School of Health Sciences, Ariel University, Ariel, Israel.
2 Genetics Unit and Department of Obstetrics and Gynecology, Shaare Zedek Medical Center, Jerusalem, Israel.
3 Department of Nutrition, School of Health Sciences, Ariel University, Ariel, Israel. ruthb@ariel.ac.il.
PURPOSE:
Preterm birth (PTB) is a complex trait with strong genetic background, whose etiology is not fully understood. It was recently suggested that pregnancy duration is affected by fetal genetic variation even more than by the maternal genome. Vitamin D receptor (VDR) is involved in embryonic implantation and fertility. We studied the association between both maternal and neonatal vitamin D receptor (VDR) genetic variation and PTB.
METHODS:
Maternal and fetal (umbilical cord) DNA was isolated from Jewish Israeli idiopathic preterm newborns (24-36 weeks, n = 146) and control term newborns (>37 weeks, n = 229). Maternal and fetal VDR polymorphisms (FokI, ApaI, BsmI, TaqI) were analyzed by restriction fragment length polymorphism analysis. Using SPSS analysis to correlate VDR genotypes with phenotypic variation: pregnancy duration, preterm birth and spontaneous miscarriages, adjusted for gravidity, parity and gender of newborn.
RESULTS:
Women homozygous to VDR ApaI (AA) genotype had significant twofold increase risk for PTB [OR 1.973, (CI) 1.183-3.289, p = 0.009] compared to heterozygous women. Male newborns had significant (p < 0.05) 1.73-fold increase of PTB.
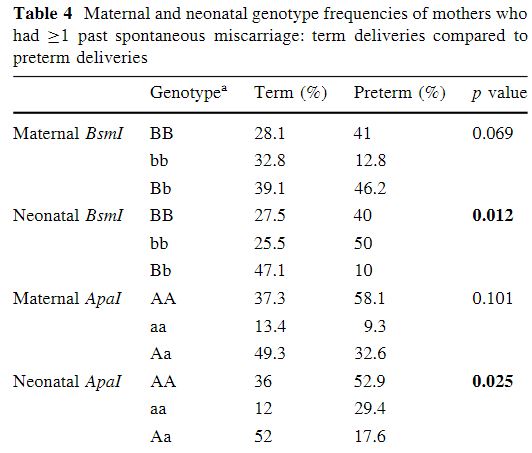
Women with history of previous (≥1) spontaneous miscarriage had a significant increased risk for PTB if their newborn carried either of the
VDR BsmI homozygous (BB or bb) genotypes compared to the heterozygous (Bb) genotype [OR 6.857, (CI) 1.273-36.934, p = 0.018 and
OR 9.231 , (CI) 1.753-48.618, p = 0.008, respectively],
or VDR ApaI homozygous (AA or aa) genotype compared to heterozygous (Aa) genotype [OR 4.33, (CI) 1.029-18.257, p = 0.046 and OR 7.2, (CI) 1.34-38.917, p = 0.021, respectively].
CONCLUSIONS:
We show association between maternal and fetal VDR genotype variants with PTB.