Overweight elderly respond well to 3600 IU Vitamin D daily for a year – RCT
Vitamin D3 Dose Requirement that Raises 25-Hydroxyvitamin D to Desirable Level in Overweight and Obese Elderly
The Journal of Clinical Endocrinology & Metabolism, https://doi.org/10.1210/clinem/dgab296
Dania S Bacha, Maya Rahme, Laila Al-Shaar, Rafic Baddoura, Georges Halaby, Ravinder J Singh, Ziyad R Mahfoud, Robert Habib, Asma Arabi, Ghada El-Hajj Fuleihan

72% of obese seniors got >30 ng after 12 months of daily 3750 IU Vitamin D + Calcium
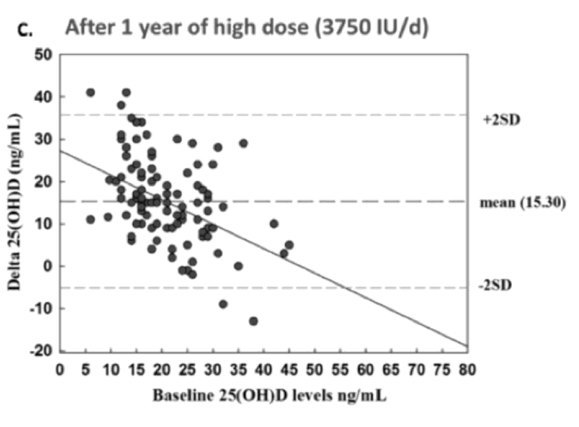

Note: Some vitamin D levels DECREASED
📄 Download the PDF from VitaminDWiki
Purpose
To investigate the impact of two vitamin D doses, bracketed between the IOM recommended dietary allowance (RDA) and the upper tolerable limit, on vitamin D nutritional status in elderly individuals.
Methods
This is a post-hoc analysis on data collected from a 12-month, double-blinded, randomized control trial. 221 ambulatory participants (≥ 65 years), with a mean BMI of 30.2 kg/m 2, and a mean baseline serum 25-hydroxyvitamin D [25(OH)D] level of 20.4 ± 7.4 ng/ml, were recruited from 3 out-patient centers in Lebanon. They all received 1,000 mg of elemental calcium from calcium citrate daily, and the daily equivalent of 600 IU or 3,750 IU, of vitamin D3.
Results
Mean 25-hydroxyvitamin D [25(OH)D] level at 12 months was 26.0 ng/ml with low dose and 36.0 ng/ml with high dose, of vitamin D3. The proportion of participants reaching a value ≥ 20 ng/ml was 86% in the low dose, and 99% in the high-dose arms, with no differences between genders. The increment of 25(OH)D per 100 IU/day was 1ng/ml with the low dose, and 0.41 ng/ml with the high dose. Serum 25 (OH)D levels at 1 year were highly variable in both treatment arms. Baseline 25(OH)D level and vitamin D dose, but not age, BMI, gender, nor season, were significant predictors of serum 25(OH)D level post-intervention.
Conclusion
The IOM RDA of 600 IU/day does not bring 97.5% of ambulatory elderly individuals above the desirable threshold of 20 ng/ml. Country-specific RDAs are best derived taking into account the observed variability and predictors of achieved 25(OH)D levels.