Obese need more Vitamin D - Feb 2026
Vitamin D in Obesity: Mechanisms and Clinical Impact
Obesities Feb 2026 https://doi.org/10.3390/obesities6010012
Jitka Jirku 1/2'* , Zuzana Krsakova 1© and Jarmila Krizova h* 3rd Department of Internal Medicine, Department of Endocrinology and Metabolism, General University Hospital in Prague—VFN, First Faculty of Medicine, Charles University, 12808 Prague, Czech Republic Nutrition Outpatient Clinic, 14000 Prague, Czech Republic * Correspondence: info@nutricniambulance.cz (J.J.); jarmila.krizova@vfn.cz (J.K.
Abstract
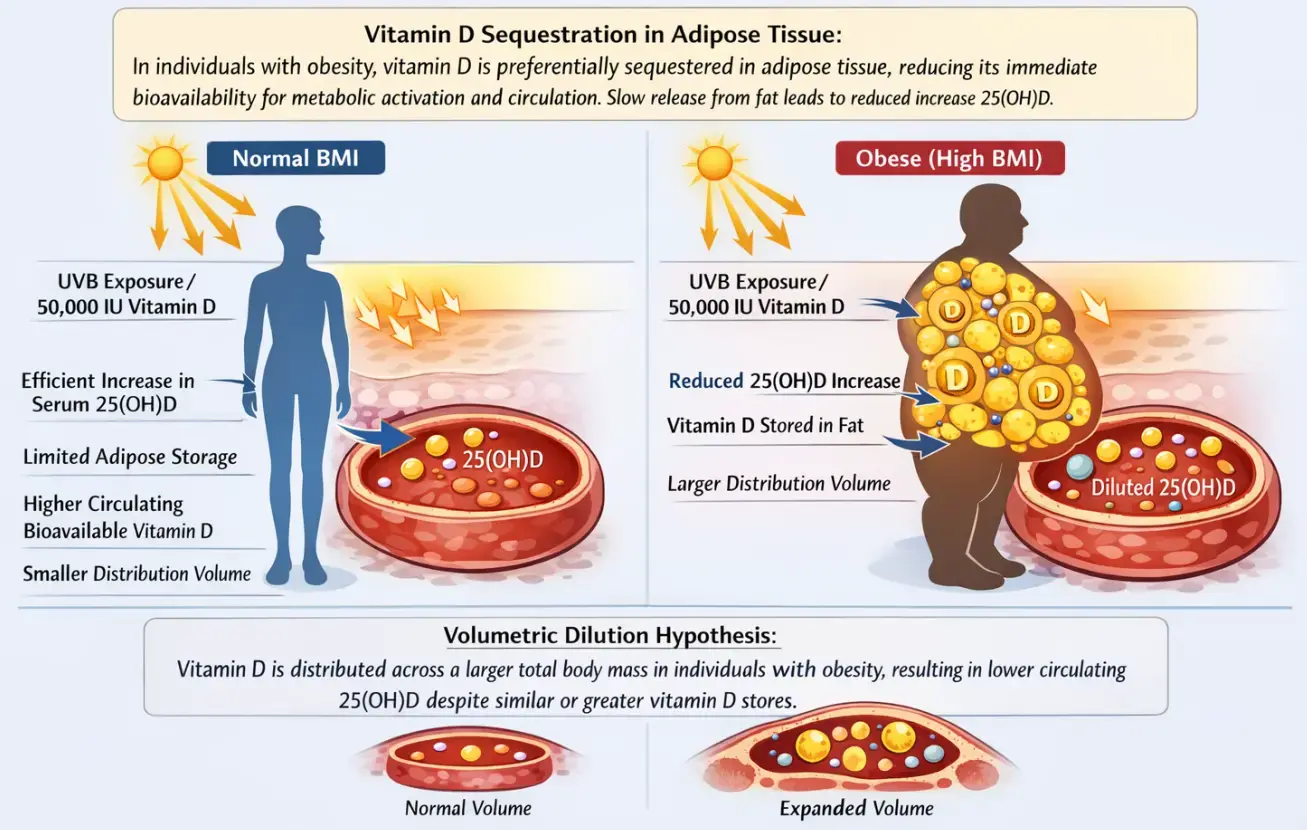
Obesity is a major global health challenge that substantially affects vitamin D metabolism and status. Numerous studies have consistently demonstrated an inverse relationship between body fat and serum 25-hydroxyvitamin D [25(OH)D] concentrations. Emerging evidence suggests that lower serum 25(OH)D in obesity largely reflects altered distribution and metabolism rather than a uniform state of true functional deficiency.
Adipose tissue functions both as a storage compartment and as a metabolically active organ capable of modulating vitamin D handling.
Mechanisms include the
- sequestration of vitamin D in fat,
- volumetric dilution across a larger body mass, and the
- local expression of enzymes involved in vitamin D metabolism.
As a result, obese individuals typically exhibit a blunted increase in serum 25(OH)D in response to supplementation, consistent with altered pharmacokinetics and increased distribution volume. Weight loss, particularly the reduction in visceral fat, is associated with modest increases in circulating 25(OH)D, further supporting a distribution-based mechanism. Although low 25(OH)D levels in obesity have been linked to insulin resistance, inflammation, and metabolic syndrome, randomized controlled trials have not consistently demonstrated that supplementation improves clinically relevant outcomes in this population. Meta-analyses confirm that the increase in serum 25(OH)D after supplementation is smaller in obese individuals, indicating that higher doses are often required to achieve comparable levels to those in normal-weight subjects.
Obesity thus represents a major determinant of vitamin D deficiency, highlighting the need for individualized supplementation strategies alongside weight management. Understanding the mechanistic basis for low 25(OH)D in obesity is essential for distinguishing true deficiency from altered distribution, informing clinical decisions, and optimizing interventions to maintain adequate vitamin D status and support metabolic health.
Conclusions from the PDF
Obesity represents an important risk factor for low circulating concentrations of 25-hydroxyvitamin D, reflecting a combination of increased sequestration in adipose tissue, expanded distribution volume, and altered vitamin D pharmacokinetics. Consequently, individuals with obesity commonly exhibit lower serum 25(OH)D concentrations and a reduced biochemical response to standard supplementation. Increasing evidence suggests that these findings predominantly reflect altered distribution, binding, and dilutional effects rather than a uniform functional vitamin D deficiency at the tissue level. Although low circulating 25(OH)D concentrations in obesity have been associated with disturbances in bone metabolism, insulin resistance, metabolic syndrome, and cardiovascular disease, the causal nature of these associations remains incompletely established. Emerging data on free and bioavailable vitamin D further indicate that total serum 25(OH)D may not fully reflect vitamin D availability to target tissues in obesity, although methodological heterogeneity currently limits definitive conclusions and routine clinical implementation. Future interventional studies should focus on vitamin D-deficient obese populations and use weight-adjusted dosing strategies to clarify potential clinical benefits.
Taken together, current evidence supports a cautious and individualized clinical approach. Assessment of vitamin D status and supplementation may be appropriate, particularly in the presence of established indications, skeletal involvement, or confirmed deficiency; however, routine high-dose supplementation solely on the basis of obesity is not supported by robust evidence for clinical benefit. In this context, careful interpretation of 25(OH)D concentrations is warranted, taking into account body composition, distribution volume, and clinical context rather than relying on uniform threshold-based definitions.
From both clinical and public health perspectives, prevention and effective management of obesity remain central strategies—not only for optimizing vitamin D bioavailability to target tissues, but also for improving overall metabolic health and reducing obesity- related morbidity. Addressing excess adiposity therefore represents a more fundamental intervention than vitamin D supplementation alone in mitigating the endocrine and metabolic consequences associated with obesity.
Related in VitaminDWiki
- Weight loss and Vitamin D - many studies
- Vitamin D Receptor and Obesity – many studies
- Child Obesity and Vitamin D - many studies
- Top 10 Chronic Health Problems Associated with Obesity all associated with low Vitamin D
FACT: People who are obese have less vitamin D in their blood
FACT: Obese need a higher dose of vitamin D to get to the same level of vit D
FACT: When obese people lose weight the vitamin D level in their blood increases
FACT: Adding Calcium, perhaps in the form of fortified milk, often reduces weight
FACT: 204 trials for vitamin D intervention of obesity as of April 2025
FACT: Less weight gain by senior women with > 30 ng of vitamin D
FACT: Dieters lost additional 5 lbs if vitamin D supplementation got them above 32 ng - RCT
FACT: Those with darker skins were more likely to be obese Sept 2014
OBSERVATION: Low Vitamin D while pregnancy ==> more obese child and adult
OBSERVATION: Many mammals had evolved to add fat and vitamin D in the autumn
Obese need 2X to 3X more vitamin D
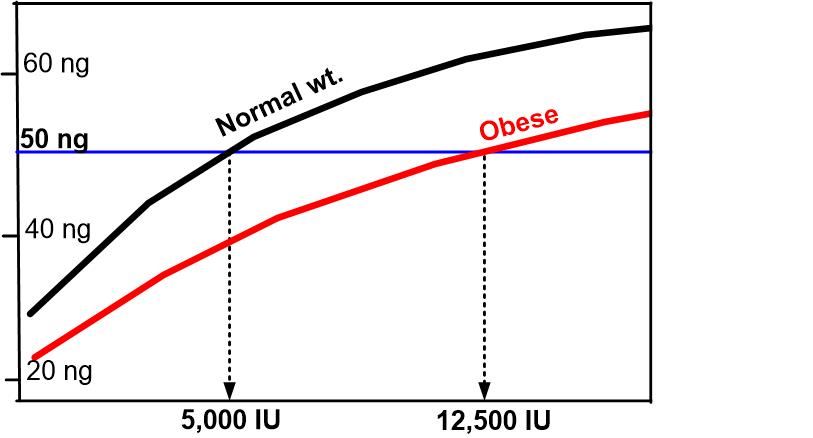
Normal weight Obese (50 ng = 125 nanomole)
How Much More Vitamin D Do Obese People Need? Perplexity AI - Feb 2026
The Short Answer: 2 to 3 Times More
The Endocrine Society's Clinical Practice Guidelines explicitly recommend that obese adults take two to three times more vitamin D than normal-weight adults of the same age to satisfy their body's vitamin D requirement. Overweight individuals (BMI 25–29.9) need roughly 1.5 times more.[^1][^2][^3]
Specific Dosing Estimates by BMI
Large observational dose-response studies have quantified these multipliers with precision. A study led by Veugelers et al. (University of Alberta) using data from the GrassrootsHealth cohort found:[^4][^3]
| BMI Category | Multiplier vs. Normal Weight | Estimated IU/day to Reach 40 ng/mL (100 nmol/L) |
|---|---|---|
| Normal weight (≤25) | 1× (baseline) | ~2,000 IU/day |
| Overweight (25–30) | ~1.5× | ~3,000 IU/day |
| Obese (≥30) | ~2.5–3× | ~5,500 IU/day |
These numbers were derived from dose-response modeling in a population of healthy volunteers. The GrassrootsHealth project independently confirmed that approximately three times more supplemental vitamin D was needed for those with a BMI above 30 compared to those with a BMI at 25 or lower to achieve a serum 25(OH)D of 40 ng/mL.[^3][^4]
Endocrine Society Guidelines
The 2011 Endocrine Society guidelines (Holick et al.) provide the following recommendations for obese individuals:[^1]
- Treatment of deficiency: 6,000–10,000 IU/day of vitamin D₃ (two to three times the standard treatment dose) to achieve a 25(OH)D level above 30 ng/mL
- Maintenance after correction: 3,000–6,000 IU/day
A 2021 systematic review of dosing studies in obese patients concluded that the cholecalciferol treatment dose in patients with obesity may need to triple the requirements of non-obese individuals.[^5]
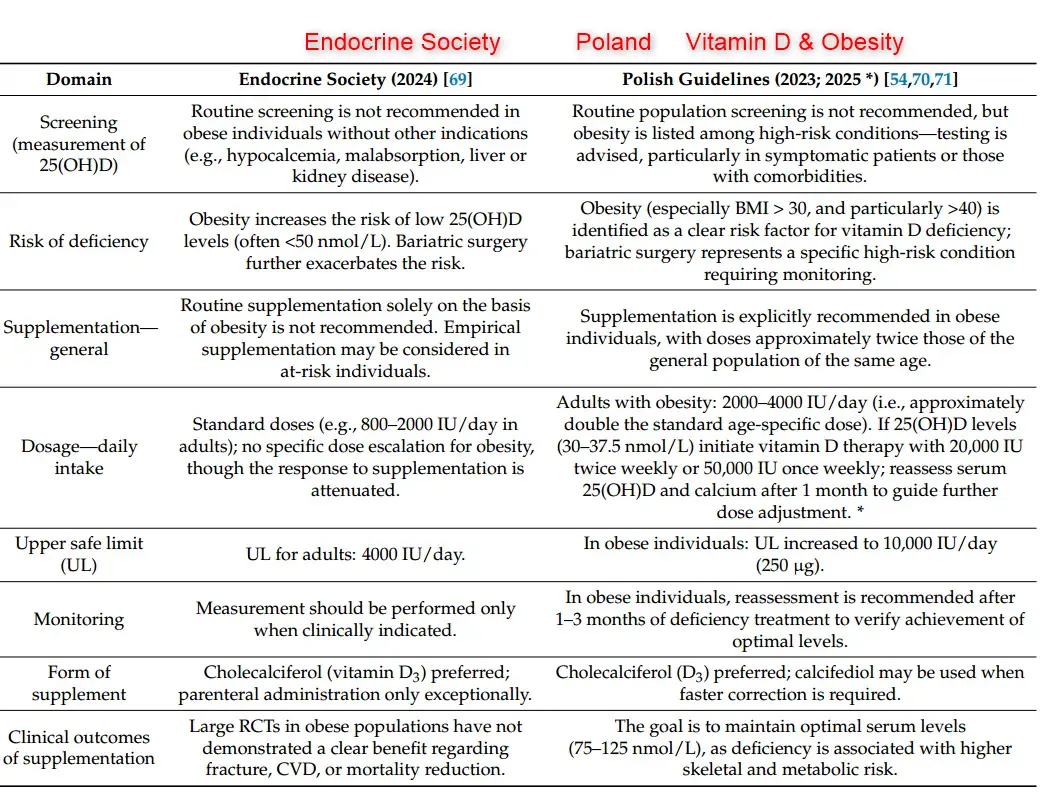
It is worth noting that the 2024 Endocrine Society guideline update took a different approach for the general healthy population, de-emphasizing routine testing and specific serum targets. However, obesity remains a recognized modifier of vitamin D requirements.[^6]
Why Obese People Need More: The Mechanisms
Two primary hypotheses explain why higher body weight leads to lower circulating vitamin D levels:
Volumetric Dilution
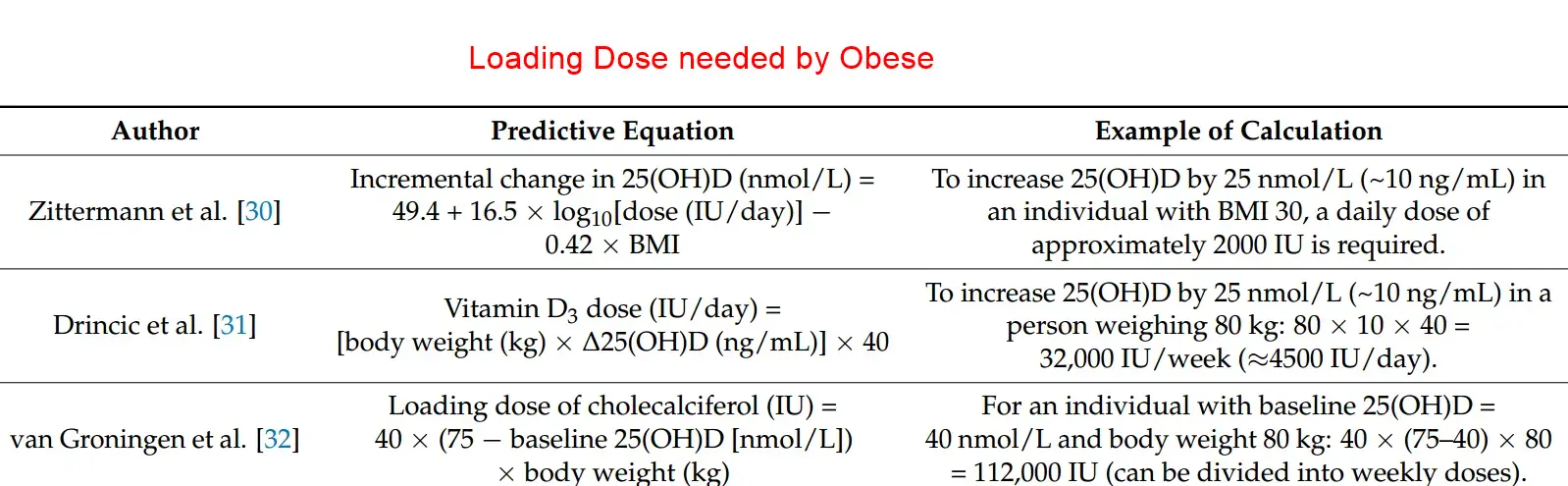
Drincic et al. (2012) at Creighton University analyzed 686 adults and demonstrated that a hyperbolic model of 25(OH)D against body weight fully removed the obesity-related variability in serum vitamin D levels. Their conclusion was that simple volumetric dilution—the spreading of the same amount of vitamin D across a larger body mass—is the most parsimonious explanation for low vitamin D status in obesity. In their follow-up dosing study, they found obese subjects required approximately 2.5 IU per kilogram of body weight for every 1 ng/mL increment in serum 25(OH)D.[^7][^8][^9]
Adipose Tissue Sequestration and Impaired Release
A 2017 study in The Journal of Clinical Endocrinology & Metabolism provided direct experimental evidence that the problem goes beyond simple dilution. Key findings include:[^10]
- Obese adipose tissue has reduced adrenaline-stimulated lipolytic release of both vitamin D₃ and 25(OH)D
- Insulin-resistant adipocytes show reduced expression of the 25-hydroxylating enzyme CYP27A1, meaning adipose tissue in obesity converts less vitamin D to its active form
- Vitamin D becomes effectively "trapped" in dysfunctional adipose tissue due to lipolytic resistance
Additional research suggests that exercise may help mobilize vitamin D from adipose tissue even without weight loss, though this is still being investigated.[^11]
Hepatic Impairment
A third hypothesis, supported by JAMA Network Open data from the VITAL trial, suggests that obesity-induced hepatic dysfunction may impair vitamin D metabolism. Oral vitamin D requires hepatic CYP enzymes for conversion to 25(OH)D, and animal models have shown downregulation of CYP2R1 in obesity and diabetes.[^12]
Evidence from the VITAL Trial (2023)
The largest and most recent data come from a 2023 JAMA Network Open study analyzing 16,515 participants from the VITAL trial, which used 2,000 IU/day of vitamin D₃:[^12]
- Baseline 25(OH)D levels were incrementally lower at higher BMI: 32.3 ng/mL (normal weight) vs. 28.0 ng/mL (obesity class II)
- Response to supplementation was blunted at higher BMI: After 2 years, the increase in 25(OH)D from supplementation was 13.5 ng/mL for BMI <25 vs. 10.0 ng/mL for BMI ≥35
- This blunted response extended to free vitamin D and bioavailable vitamin D, not just total 25(OH)D
- Critically, vitamin D supplementation reduced cancer incidence by 24% in normal-weight participants but showed no benefit in those with overweight or obesity—suggesting the standard 2,000 IU dose was insufficient for larger bodies
A 2025 study from Tufts University further found that obesity may extend the time required to reach a steady-state 25(OH)D level after initiating supplementation.[^13]
Dose-Response by Body Weight
The dose-response relationship is not binary. Research shows a continuous inverse relationship between BMI and serum 25(OH)D response per 1,000 IU of supplementation:[^3]
| BMI Category | 25(OH)D Increase per 1,000 IU/day |
|---|---|
| Normal weight | ~13.1 nmol/L |
| Overweight | ~11.5 nmol/L |
| Obese (≥30) | ~8.6 nmol/L |
This means obese individuals get about 35% less vitamin D response per unit dose compared to normal-weight individuals. Another study calculated the dose-response slope in obese subjects (BMI ≥35) at 0.398 nmol/L per μg/day, compared to 0.66 nmol/L per μg/day in healthy non-obese subjects—a 40% reduction.[^14][^3]
Practical Recommendations
- Obese individuals (BMI ≥30) should take 2–3× the standard dose for their age group[^1][^3]
- Overweight individuals (BMI 25–30) should take approximately 1.5× the standard dose[^2][^3]
- Blood testing is the only reliable way to determine individual needs, since response varies considerably even within BMI categories[^4]
- Weight-based dosing (approximately 2.5 IU per kg body weight per desired 1 ng/mL increase) may be more precise than BMI-category multipliers[^7]
- Weight loss itself raises circulating 25(OH)D levels without changes in supplementation[^12]
- Supplementation with 25-hydroxyvitamin D₃ (calcifediol) rather than standard vitamin D₃ may be more effective in achieving sufficiency in obese patients because it bypasses the hepatic conversion step[^10]
Mendelian Randomization: Obesity Causes Low Vitamin D, Not Vice Versa
A bi-directional Mendelian randomization study using data from 42,024 participants confirmed that higher BMI causally leads to lower 25(OH)D levels (a 10% higher genetically instrumented BMI was associated with 4.2% lower 25(OH)D). Genetically instrumented lower vitamin D did not cause higher BMI, confirming that the direction of causation is from obesity to vitamin D insufficiency, not the reverse.[^15]
References
Evaluation, Treatment, and Prevention of Vitamin D Deficiency - 3.4 We suggest that all adults who are vitamin D deficient be treated with 50,000 IU of vitamin D2 o...
Myth or reality: Vitamin D and dosing by body weight - If your BMI is 25-29.9, you are considered overweight for your height. If your BMI is 30 or higher y...
The Importance of Body Weight for the Dose Response Relationship ... - BMI, relative to absolute body weight, was found to be the better determinant of 25(OH)D. Relative t...
Your Weight Influences Your Need for Vitamin D - GrassrootsHealth - Evidence shows that vitamin D levels are affected by obesity. In fact, the more fat a person has on ...
Optimal dosage of vitamin D supplementation in obese patients with ... - Cholecalciferol 'treatment dose in patients with obesity might triple the requirements of non-obese ...
Endocrine Society Guideline recommends healthy adults under the ... - Endocrine Society Guideline recommends healthy adults under the age of 75 take the recommended daily...
25-Hydroxyvitamin D Response to Graded Vitamin D3 ... - Guidelines have suggested that obese adults need 2 to 3 times more vitamin D than lean adults to tre...
Volumetric Dilution, Rather Than Sequestration Best Explains the ... - We suggest that simple volumetric dilution is the most parsimonious explanation for the low vitamin ...
Volumetric dilution, rather than sequestration best explains the low ... - Dilution of ingested or cutaneously synthesized vitamin D in the large fat mass of obese patients fu...
Impaired Release of Vitamin D in Dysfunctional Adipose Tissue ... - Supplementation with 25-hydroxyvitamin-D3 was more effective in achieving vitamin D sufficiency in o...
Mobilising vitamin D from adipose tissue: The potential impact of ... - Emerging evidence suggests that exercise may mobilise vitamin D from adipose (even in the absence of...
Association of Body Weight With Response to Vitamin D ... - In VITAL, mean serum total 25-OHD levels with active supplementation at 1 year follow-up were signif...
Obesity may extend the time required to reach a steady-state 25(OH ... - This observational study was done to investigate whether BMI modified the time required to reach a s...
The vitamin D dose response in obesity - Conclusion: The dose response of vitamin D3 (slope) in obese subjects was significantly lower (P<. 0...
Causal Relationship between Obesity and Vitamin D Status - Drincic AT, Armas LA, Van Diest EE, Heaney RP (2012) Volumetric dilution, rather than sequestration ...