Non-Alcoholic Fatty Liver Disease (NAFLD) treated by Vitamin D (20,000 IU weekly after loading dose) – RCT
Effect of Short-Term Vitamin D Correction on Hepatic Steatosis as Quantified by Controlled Attenuation Parameter (CAP).
J Gastrointestin Liver Dis. 2016 Jun;25(2):175-81. doi: 10.15403/jgld.2014.1121.252.cap.
Papapostoli I1, Lammert F1, Stokes CS2.
1Department of Medicine II, Saarland University Medical Center, Homburg, Germany.
2Department of Medicine II, Saarland University Medical Center, Homburg, Germany. caroline.stokes@uks.eu.
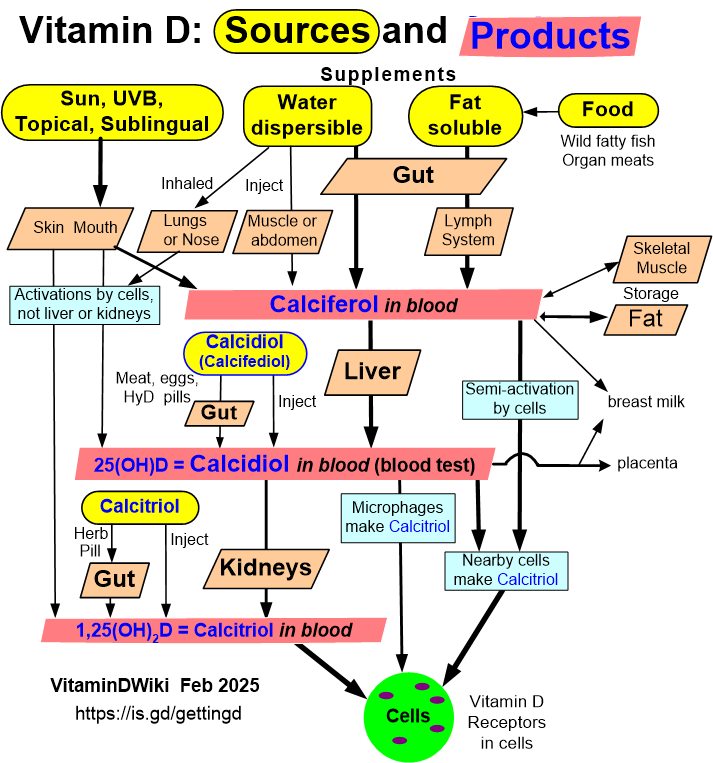 Click on image for Calcidiol information
See also web
* Vitamin D-induced autophagy prevents steatosis Feb 2017
* underlying mechanism: " 1,25(OH)2D3 is shown to protect against hepatic steatosis by inducing autophagy " Publisher wants $8 for the PDF
* Vitamin D and histologic severity of nonalcoholic fatty liver disease: A systematic review and meta-analysis Feb 2017, unsure
* Is Vitamin D an Independent Risk Factor of Nonalcoholic Fatty Liver Disease?: a Cross-Sectional Study of the Healthy Population Jan 2017, 30% more likely in men if < 20 ng of vitamin D - Free PDF online
* Low vitamin D status is associated with advanced liver fibrosis in patients with nonalcoholic fatty liver disease. Feb 2017, PDF costs $40
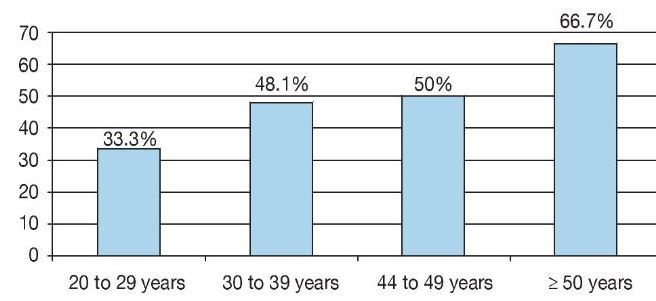
* NAFLD among Obese 2016 has the following chart
*
Click on image for Calcidiol information
See also web
* Vitamin D-induced autophagy prevents steatosis Feb 2017
* underlying mechanism: " 1,25(OH)2D3 is shown to protect against hepatic steatosis by inducing autophagy " Publisher wants $8 for the PDF
* Vitamin D and histologic severity of nonalcoholic fatty liver disease: A systematic review and meta-analysis Feb 2017, unsure
* Is Vitamin D an Independent Risk Factor of Nonalcoholic Fatty Liver Disease?: a Cross-Sectional Study of the Healthy Population Jan 2017, 30% more likely in men if < 20 ng of vitamin D - Free PDF online
* Low vitamin D status is associated with advanced liver fibrosis in patients with nonalcoholic fatty liver disease. Feb 2017, PDF costs $40
* NAFLD among Obese 2016 has the following chart
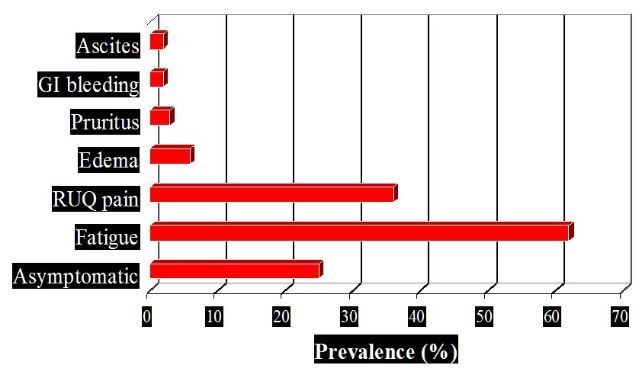
*  * Nonalcoholic Fatty Liver Disease (NAFLD)
* SYMPTOMS : HowMed - before 2017
*
* Nonalcoholic Fatty Liver Disease (NAFLD)
* SYMPTOMS : HowMed - before 2017
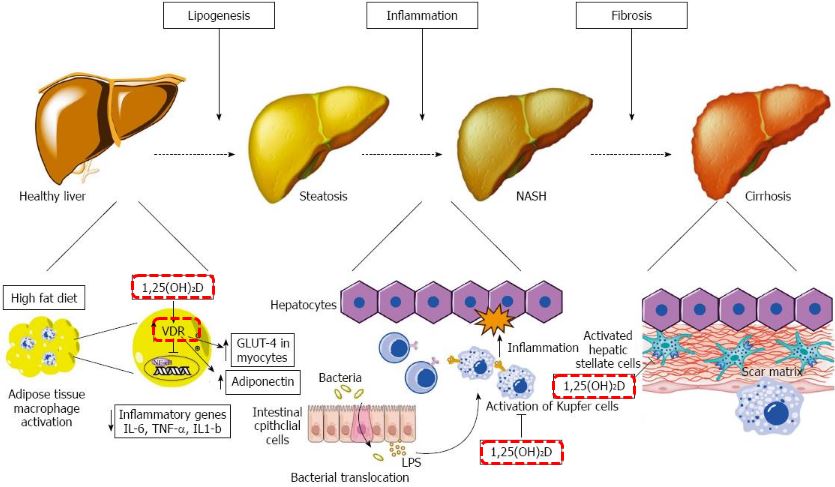
*  * Vitamin D: A new player in non-alcoholic fatty liver disease? Feb 2015
* Vitamin D: A new player in non-alcoholic fatty liver disease? Feb 2015
 * Special Nutrients issue on NAFLD 2017
* 22 items includes:
* * *📄 Vitamin D Supplementation and Non-Alcoholic Fatty Liver Disease: Present and Future,* *
* does not appear to be aware of other forms or types of Vitamin D needed for NAFLD
* Poor Vitamin A,
* Insuline resistance,
* 32% of population now have metabolic syndrome,
* Iron problems with NAFLD,
* Special Nutrients issue on NAFLD 2017
* 22 items includes:
* * *📄 Vitamin D Supplementation and Non-Alcoholic Fatty Liver Disease: Present and Future,* *
* does not appear to be aware of other forms or types of Vitamin D needed for NAFLD
* Poor Vitamin A,
* Insuline resistance,
* 32% of population now have metabolic syndrome,
* Iron problems with NAFLD,
📄 Download the PDF from VitaminDWiki
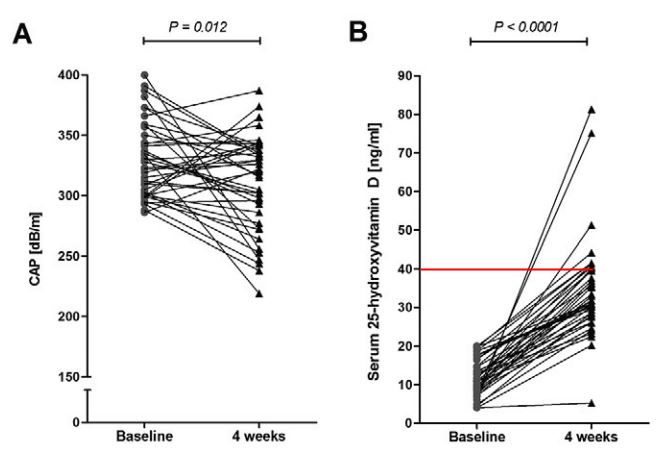
Note poor vitamin D response in first month, and Controlled Attenuation Parameter actually increased for a fraction of the people
INTRODUCTION:
Non-alcoholic fatty liver disease (NAFLD) is the most common cause of chronic liver disease in Western countries. A meta-analysis has confirmed decreased serum 25-hydroxyvitamin D levels in NAFLD patients. This intervention study investigates whether vitamin D correction ameliorates hepatic steatosis.
METHODS:
We prospectively recruited 40 patients from an outpatient liver clinic with vitamin D deficiency (serum 25-hydroxyvitamin D < 20 ng/ml). Controlled attenuation parameter (CAP) during transient elastography quantified hepatic steatosis. Patients with significant liver fat accumulation were included, which was defined by a CAP value >/= 280 dB/m. Patients received 20,000 IU vitamin D/week for six months, while vitamin D status, liver function tests (LFTs), CAP and body composition were monitored.
RESULTS:
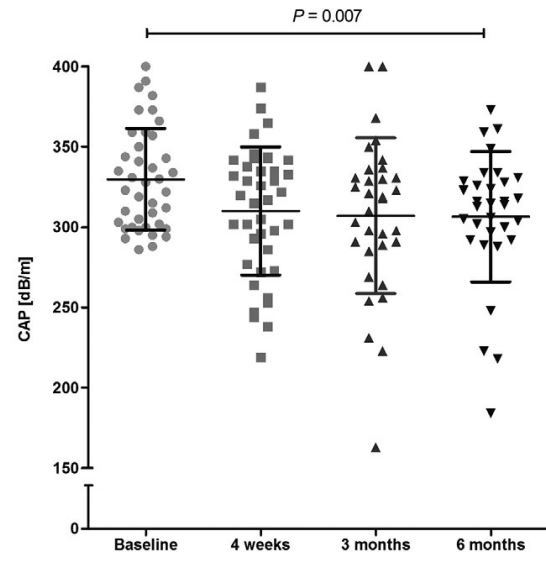
The cohort comprised 47.5% women (age 54.9 +/- 12.1 years; BMI 29.5 +/- 3.0 kg/m2). Mean serum vitamin D level was 11.8 +/- 4.8 ng/ml. CAP decreased significantly from baseline (330 +/- 32 vs. 307 +/- 41 dB/m) during supplementation (P = 0.007). A mean CAP reduction relative to baseline was demonstrated at four weeks and three and six months: -5.3 +/- 13.8%; -6.0 +/- 14.6% and -6.4 +/- 13.0%, respectively. During these time points, restoration of serum vitamin D levels was observed (34.6 +/- 12.9, 36.3 +/- 10.2, 34.8 +/- 9.8 ng/ml; P < 0.0001). Liver function tests and body composition remained unchanged.
CONCLUSIONS:
Hepatic steatosis, as assessed by CAP, significantly improves after only 4 weeks of vitamin D correction. Hepatic steatosis is a dynamic process, that can be monitored in the short-term using such non-invasive methods.
PMID: 27308648