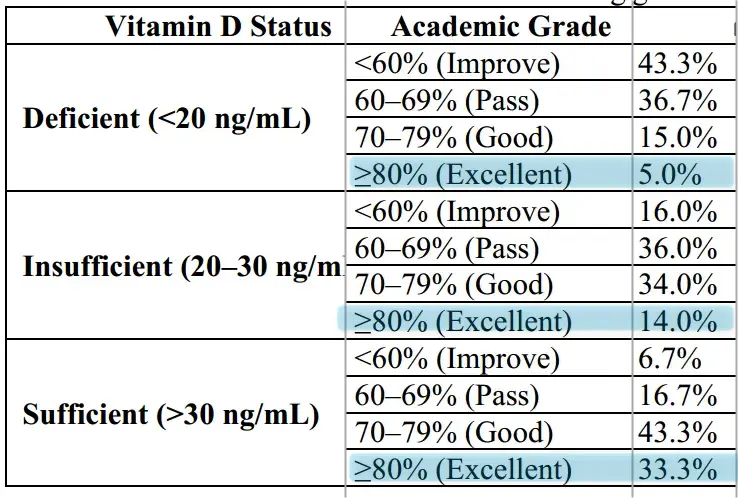
Students with higher Vitamin D earn higher grades
Vitamin D Deficiency and Its Relationship with Academic Performance among Medical Students: A Cross-Sectional Study from Nawabshah (Pakistan)
International J of Pharmacy Research & Technology | JAN -JUNE 2026| Vol 16| Issue 1 DOI: 10.48047/ijprt/16.01.172
Background: Vitamin D deficiency has become a global health concern and is of increasing concern for healthcare providers. The limited knowledge about the importance of vitamin D supplements is one reason why it remains so common. Medical students often prioritize academic and clinical responsibilities during both their early and late years of MBBS, which increases their risk of deficiency due to poor lifestyle choices.
Materials and Methods: This was a cross-sectional study involving 140 medical students aged 19-30, conducted over six months. A structured questionnaire collected data on demographic details, supplement use, physical activity, body mass index (BMI), and sun exposure, including the percentage of body surface area exposed.
Results: 43 percent of participants were found to be vitamin D deficient, and 36 percent had levels below the recommended range. Deficiency was strongly associated with minimal daily sun exposure (less than 15 minutes). Additionally, a significant portion of students who reported adequate vitamin D levels also noted improved academic performance; about 80 percent of them reported better grades.
Conclusion: Vitamin D deficiency is still very widespread among medical students, which is mostly caused by a sedentary lifestyle, unhealthy eating habits, insufficient intake of supplements, and a lack of sun exposure. Early intervention through dietary modification, increased awareness, supplementation, and food fortification strategies is essential to reduce long-term health risks in this population.
Observation seems plausible: no long-term trials that confirm nor deny it
Suspect that vitamin D levels must be high since birth or since starting school
Vitamin D and academic performance: biologically plausible but epidemiologically unproven (Claude AI)
Low vitamin D consistently tracks with poorer academic outcomes in observational studies — but the causal case remains weak. Cross-sectional studies from regions with high deficiency prevalence (Middle East, Africa, South Asia) frequently link insufficient 25(OH)D to lower grades and test scores, with adjusted odds ratios reaching 2.18 in one well-controlled study. However, large prospective cohorts in Western populations find these associations vanish after adjusting for socioeconomic status and ethnicity. No randomized trial has yet demonstrated that vitamin D supplementation improves academic grades. The biological rationale is strong — vitamin D receptors saturate the hippocampus and prefrontal cortex, (pubMed central) (Nature) and the vitamin regulates BDNF, dopamine, and serotonin (PubMed central+3) — but translating this neuroscience into classroom outcomes remains an open question.
Observational studies paint a geographically split picture
The most striking pattern in the observational literature is geographic: studies from high-deficiency regions find positive associations, while large Western cohorts do not.
Positive findings cluster in the Middle East, Africa, and South Asia. Elbashir et al. (2023) studied 241 Sudanese adolescents (PubMed central) and found vitamin D deficiency (<20 ng/mL) doubled the odds of poor academic performance (AOR = 2.18,95% Cl 1.20-3.96), surviving multivariate adjustment for gender, BMI, and parental education. (PubMed central) In Saudi Arabia, Almuqbil et al. (2023) reported that 59.8% of480 university students were vitamin D deficient, with a significant association between deficiency and lower GPA (p = 0.048). (coLab) AlZahrani and Oommen (2023) found vitamin D levels predicted GPA and self-efficacy among 213 female health science students at Northern Border University, Saudi Arabia, (Emerald) (Emerald insight) with the strongest effects in second- and third-year students experiencing peak academic stress. (Emerald insight) In India, Nair and Devika (2017) documented high deficiency prevalence among 62 Kerala adolescents presenting with recent-onset scholastic decline.
The 2026 Nawabshah study referenced in the query — reporting that 33% of vitamin D-sufificient medical students scored ^80% versus only 5% of deficient students — fits this pattern precisely. Though I was unable to locate its indexed citation (it may be in press or recently published), its findings align with the broader South Asian and Middle Eastern literature where baseline deficiency rates often exceed 50-60%.
Large Western studies consistently report null results. The ALSPAC birth cohort
(Tolppanen et aL, 2012) followed 3,171 UK children with vitamin D measured at age 9.8 years and found no association between vitamin D3 and academic performance at ages 13-16 in English, math, science, or GCSE grades. (PubMed) Paradoxically, higher vitamin D2 predicted worse performance, likely reflecting socioeconomic confounding (D2 was more common in disadvantaged backgrounds), (university of Bristol) The NHANES III analysis (Tolppanen et al., 2011) of several thousand US adolescents aged 12-17 found positive raw associations between 25(OH)D and all four cognitive tests (digit span: p = 0.10 SD per SD increase in vitamin D), but these were completely attenuated to null after adjusting for race/ethnicity and test language, (wiiey online Library) (ovid)In Kuwait, Al-Taiar et al. (2018) found no association between vitamin D and either Raven's Progressive Matrices scores or academic achievement among 1,370 adolescents after confounder adjustment. (PubMed)
This divergence likely reflects confounding rather than true geographic heterogeneity. Vitamin D status covaries with poverty, diet quality, outdoor activity, and educational resources — precisely the factors that independently drive academic performance.
The neuroscience case is compelling but does not prove causation
The biological rationale for vitamin D affecting cognition rests on three pillars, all well-documented in animal and cell studies.
Vitamin D receptors blanket the cognitive brain. Eyles et al. (2005) mapped VDR and la-hydroxylase (CYP27B1) expression throughout the human brain, finding dense concentrations in the hippocampus (all CA1-CA4 pyramidal layers), prefrontal cortex, cingulate gyrus, thalamus, and cerebellum — regions governing memory, executive function, and learning. VDR appears as early as embryonic day 12 in rodents, coinciding with peak dopaminergic neurogenesis. (PubMed Central) (PubMed Central)
Vitamin D regulates key neurotrophic factors. The vitamin upregulates BDNF (brain-derived neurotrophic factor), the dominant neurotrophin in the hippocampus and a critical driver of long-term potentiation — the cellular mechanism of learning, (intechopen) (ResearchGate) Supplementation of >2,000 IU/day for 12 weeks increases BDNF levels by approximately 7%. (PubMed) (mdpi) Vitamin D also promotes nerve growth factor (NGF) and glial-derived neurotrophic factor (GDNF) production. (PubMed central) In rat models, vitamin D3 administration prevented stress-induced BDNF reductions and amyloid-beta accumulation in the hippocampus.(Nature)
Neurotransmitter synthesis depends on vitamin D. The vitamin activates tryptophan hydroxylase 2 (TPH2), channeling tryptophan toward serotonin rather than kynurenine — directly affecting mood, neural plasticity, and sensory processing. (Nature) Developmental vitamin D deficiency reduces Nurrl and p57kip2a (dopaminergic specification factors), alters dopamine neuron positioning, and elevates dopamine turnover in the neonatal forebrain. (pubMed central+2) Vitamin D also modulates GABAergic and glutamatergic signaling through effects on glutamate decarboxylase and NMDA receptor expression.
These mechanisms make it plausible that severe deficiency could impair learning. But plausibility is not proof, and the gap between hippocampal VDR expression and final-exam grades spans an enormous causal chain.
Intervention trials mostly disappoint — with notable exceptions
The critical test of causation is whether supplementation improves outcomes. Here, the evidence is thin and largely negative for healthy students.
The only fully controlled RCT in healthy young adults found nothing. Dean et al. (2011) randomized 128 University of Queensland students to 5,000 IU/day cholecalciferol versus placebo for 6 weeks and found no significant effects on working memory (plos) (F = 1.09, p = 0.30), response inhibition (F = 0.82, p = 0.37), or cognitive flexibility (F = 1.37, p = 0.24). (PubMed central) (pios) The short duration and likely adequate baseline status limit interpretation, but this remains the best-controlled evidence in the target population.
Benefits emerge in deficient populations and with higher doses. Pettersen (2017) randomized 82 adults in northern British Columbia to 4,000 versus 400 IU/day for 18 weeks and found significant improvement in visual memory in the high-dose group (Pattern Recognition Memory: d = 0.3; Paired Associates Learning: d = 0.5). Among participants with baseline insufficiency (<75 nmol/L), the effect was large (d = 0.7, p = 0.005). (PubMed) (PubMed Central) A 2025 UAE study combined 5,000 IU/day with exercise in 32 deficient/insufficient university students over 10 weeks, finding significant improvements in working memory, verbal memory, and cognitive flexibility — though only in the vitamin D + exercise group, not exercise alone. (PubMed) Bahrami et al. (2021) gave 940 Iranian adolescent girls 50,000 IU/week for 9 weeks and reported improvements across all cognitive domains (p < 0.001), (iums) though the absence of a placebo control severely limits causal inference. (PubMed central)
No trial has measured academic grades as an outcome. This is perhaps the most critical gap. All intervention studies use laboratory cognitive tests, not GPA, exam scores, or real-world academic performance. The translation from improved Pattern Recognition Memory (effect size d = 0.3-0.7) to better grades is assumed, not demonstrated.
Prenatal vitamin D may matter more than postnatal. The Finnish VIDI trial (Tuovinen et al., 2025) randomized 398 children to 400 versus 1,200 IU/day for their first two years of life and found no IQ or executive function differences at ages 6-9. (springer)However, an inverted U-shaped relationship between maternal 25(OH)D and child IQ emerged (vertex at 76.6 nmol/L, -30.6 ng/mL), suggesting an optimal prenatal window, (springer) Rodgers et al. (2023) found children of mothers supplemented with 2,000 IU/day during pregnancy had significantly higher language scores than standard-dose offspring (B = 4.667, p = 0.044). (PubMed Central)
ADHD research offers the strongest cognitive link
The most consistent evidence connecting vitamin D to attention and learning comes from the ADHD literature — a condition defined by impaired attention, executive function, and academic underperformance.
• Khoshbakht et al. (2019) meta-analyzed 13 studies (10,334 children) and found ADHD children had 6.93 ng/mL lower vitamin D on average, (springer) with 2.57 times higher odds of ADHD in deficient children (OR 2.57,95% Cl 1.58-4.18) (PubMed central)
• Gan et al. (2019) pooled 8 studies (2,655 ADHD patients vs. 8,669 controls) finding a medium-to-large effect (SMD = -0.73,95% Cl -1.00 to -0.46) (PubMed)
• Ismail et al. (2025) conducted the largest review to date — 37 studies, 24,336 participants — confirming a pooled mean difference of -6.55 ng/mL (95% Cl -8.06 to -5.03) and OR of 1.97 for ADHD in deficiency (springer)
• Arnold et al. (2021) found that among 38 ADHD children supplemented with 1,0002,000 IU/day, inattention improvement correlated with vitamin D increase (rho = 0.41, p = 0.012) (PubMed Central) (ScienceDirect)
However, 4 of 7 RCTs in the Ismail meta-analysis were rated high risk of bias, (springer) and concurrent methylphenidate use in most trials confounds interpretation. (PubMed central) The ADHD-vitamin D link is real but may not generalize to typically developing students.
How strong is the overall evidence?
The evidence falls into a familiar pattern in nutritional epidemiology: strong observational associations, robust biological mechanisms, and disappointing intervention results. A structured assessment:
• Farhangi et al. (2023) meta-analyzed 24 RCTs with 7,557 participants and found vitamin D supplementation significantly influenced global cognition (Hedges' g = 0.128, p = 0.008) — a small but statistically significant effect. Critically, the effect was nearly four times larger in deficient populations (Hedges' g = 0.480) and in cognitively vulnerable groups (Hedges' g = 0.414) (PubMed) (springer)
• Goodwill and Szoeke (2017) found observational studies supported the association (OR = 1.24,95% Cl 1.14-1.35 for cognitive impairment with low vitamin D) but supplementation trials showed no significant benefit (SMD = 0.21,95% Cl -0.05 to 0.46) (PubMed)
• Mutua et al. (2020) systematically reviewed 32 studies (31,445 children) and found evidence too inconsistent to meta-analyze, (ox) noting that positive associations appeared more often in infancy-period assessments (springer) (pubMed central)
• No Cochrane review exists specifically for vitamin D and cognitive function, reflecting insufficient evidence for formal systematic evaluation
• No narrative review by Oommen and AlZahrani (2022) found a "paucity of literature" specifically on vitamin D and medical student academic performance
The bottom line is nuanced. Correcting frank vitamin D deficiency likely provides modest cognitive benefits — particularly in attention and visual memory domains (Frontiers) — with effect sizes of 0.3-0.7 SD in deficient populations. But the evidence that supplementation improves academic grades in students does not yet exist. The observational association between vitamin D and academic performance, while repeatedly documented in high-deficiency settings, cannot be separated from socioeconomic confounding with current evidence.
Conclusion
The Nawabshah finding — that sufficient students dramatically outperform deficient ones — is consistent with a growing body of cross-sectional evidence from the Middle East, Africa, and South Asia, where baseline deficiency rates are high and the vitamin D-achievement gradient appears steep (ORs of 1.97-2.18). Biological mechanisms firmly support a role for vitamin D in memory, attention, and executive function through hippocampal BDNF regulation, (PubMed) (Taylor & Francis online) dopaminergic signaling, (pubMed central) and synaptic plasticity. (PubMed central+3) The ADHD literature provides the strongest evidence that low vitamin D impairs attention in children (Designs for Health) (SMD = -0.73 across meta-analyses). (PubMed central)
Yet the field lacks three critical elements. First, no RCT has used academic grades as an outcome — all trials measure laboratory cognitive proxies. Second, large prospective Western cohorts find null associations after confounder adjustment, (wiiey online Library) (ovid) suggesting that at least some of the observational signal reflects poverty and lifestyle factors rather than vitamin D per se. (university of Bristol) (PubMed) Third, the only placebocontrolled trial in healthy young adults (Dean et al., 2011) found no cognitive benefit, (plos) (pios) though it was short and likely enrolled vitamin D-sufficient participants. (pubMed central) The Farhangi meta-analysis offers a reconciliation: supplementation benefits appear concentrated in those who are truly deficient (Hedges' g = 0.48), (PubMed) (springer) suggesting that in populations like Nawabshah medical students — where deficiency prevalence can exceed 60% — correcting deficiency might genuinely improve cognitive function and, by extension, academic performance. This hypothesis is
biologically grounded and epidemiologically plausible, but remains unproven by rigorous intervention data.
Related in VitaminDwiki
- Brain health improved by Vitamin D - review of 90 studies
- Cognitive problems in young adults increased 9.1X in a decade - Nov 2025
- Senior cognition improved in 4 ways by Vitamin D (50,000 IU weekly for 8 weeks)
- Better visual memory if more vitamin D
- Smaller brains associated with low vitamin D (again)
- Inhaling Vitamin D nanoemulsion through nose gets lots more to the brain (mice)
- IQ levels around the world are falling (perhaps lower Vitamin D, Iodine, or Omega-3)
- Sustained brain attention appears to vary with vitamin D levels