First trimester problems 5X more likely if start supplemention with 4,000 of Vitamin D only AFTER becoming pregnant
25-hydroxyvitamin D [25(OH)D₃] deficiency in the first trimester is associated with increased obstetric complications despite standard supplementation during pregnancy
Gynecol Obstet Invest. 2025 Nov 25:1-17. doi: 10.1159/000549513 PDF behind paywall
Maria Fernanda Lozano-Martínez, Rafael Soto Gámez, Dalia Gutierrez-González, Iván Francisco Fernández-Chau, Arnulfo Garza-Silva, Ana Sofía Sánchez-García, Maria Elena Romero-Ibarguengoitia
Background: Vitamin D deficiency during pregnancy has been linked to adverse maternal-fetal outcomes. However, it remains unclear whether standard supplementation mitigates risks equally in patients with differing baseline 25-hydroxyvitamin D [25(OH)D₃] levels.
Objectives: Determine whether differences exist in obstetric outcomes and pregnancy-related disorders among patients with different levels of 25(OH)D₃ in the first trimester who receive standard supplementation.
Design: This retrospective comparative cohort study involves pregnant women aged 16-50 years who received prenatal care at a semi-private hospital in Northeastern México between January 2022 and December 2024.
Participants/materials, setting, methods: Participants were grouped based on first trimester serum 25(OH)D₃ levels (≥30 ng/mL vs. <30 ng/mL), all receiving standard 25(OH)D₃ supplementation (4000 IU/day). For comparisons between groups, we performed independent samples t-tests or Mann-Whitney U tests for quantitative variables and chi-square tests for qualitative variables. A multivariate logistic regression analysis was conducted to identify predictors of adverse obstetric outcomes.
Results A total of 303 women [mean (SD) age 29.3 (5.4) years] were analyzed, divided almost equally between first trimester 25(OH)D₃ deficient group (n=151) and the sufficient group (n=152), with similar baseline characteristics. Although insufficient 25(OH)D₃ women reached sufficiency during the second and third trimesters, sufficient women maintained significantly higher serum 25(OH)D₃ levels throughout pregnancy (p<0.001) and had lower rates of
preeclampsia (1.3% vs. 10.6%, p<0.001),
gestational diabetes (8.6% vs. 24.5%, p<0.001),
preterm labor (0% vs. 5.3%, p=0.003),
urinary tract infections (4.6% vs. 14.6%, p=0.003), and
bacterial vaginosis (3.9% vs. 13.2%, p=0.004).
Logistic regression confirmed first-trimester 25(OH)D₃ sufficiency as independently protective against adverse outcomes (OR=0.21, 95% CI: 0.10-0.43, p<0.001).
Conclusions First-trimester 25(OH)D₃ sufficiency was associated with reduced risk of obstetric complications, compared with women with insufficiency, even when the last achieved sufficiency in the second and third-trimester. These findings highlight the importance of early screening and support the need for personalized supplementation strategies before conception to optimize maternal-fetal outcomes.
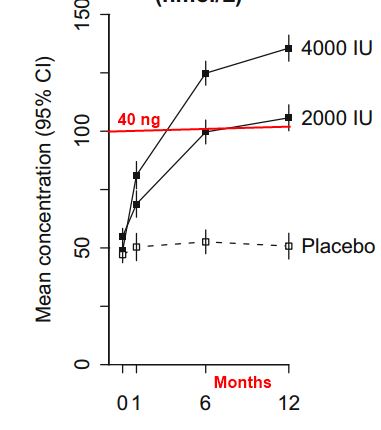
Response to 4,000 IU daily takes about 2 months, need to start before conception or start with a loading dose