COVID-19 antibodies 2.6 X more likely if had symptoms and low vitamin D (UK hospital staff)
Vitamin D status and seroconversion for COVID-19 in UK healthcare workers who isolated for COVID-19 like symptoms during the 2020 pandemic.
Aduragbemi A Faniyi, Sebastian T Lugg, Sian E Faustini, Craig Webster, Joanne E Duffy, Martin Hewison,4 Adrian Shields,2 3 Peter Nightingale,3 Alex G Richter,23* David R Thickett.13*
Correspondence to Prof David R Thickett, Institute of Inflammation and Ageing, University of Birmingham, Birmingham B15 2TH, UK; d.thickett@bham.ac.uk
📄 Download the preprint PDF from VitaminDWiki
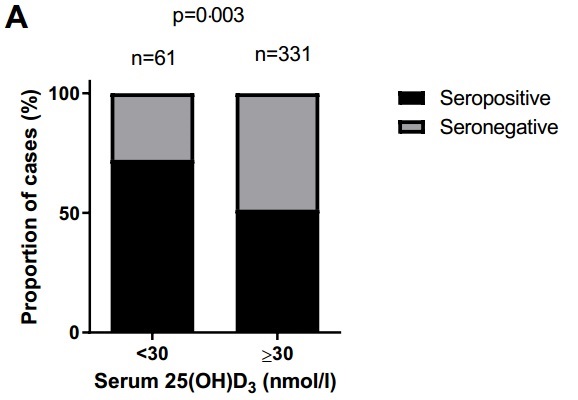
Higher D: Fewer people made antibodies
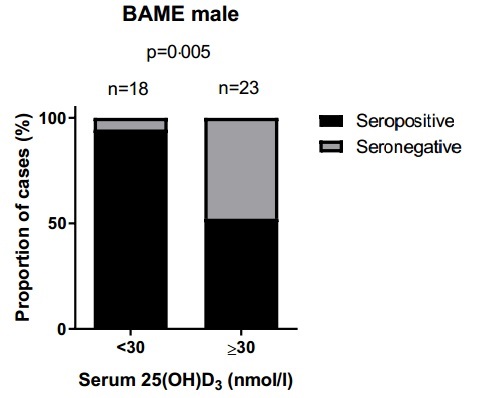
Higher D: Fewer male BAME made antibodies
Note: BAME were 8.9X more likely to have <30 nmol of VItamin D
Higher D: Less fever

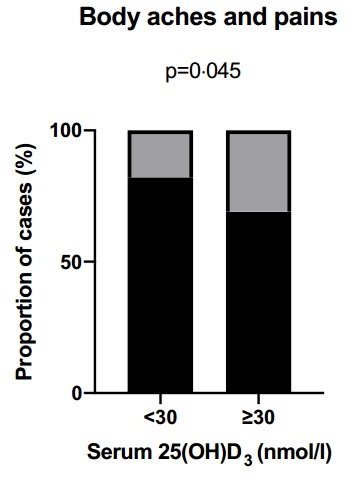
Higher D: Fewer aches and pains
Summary
Background: It is clear that in UK healthcare workers, COVID-19 infections and deaths were more likely to be in staff who were of BAME origin. This has led to much speculation about the role of vitamin D in healthcare worker COVID-19 infections. We aimed to determine the prevalence of vitamin D deficiency in NHS staff who have isolated with symptoms suggestive of COVID-19 and relate this to vitamin D status.
Methods: We recruited NHS healthcare workers between 12th to 22nd May 2020 as part of the COVID-19 convalescent immunity study (COCO). We measured anti-SARS-Cov-2 antibodies using a combined IgG, IgA and IgM ELISA (The Binding Site). Vitamin D status was determined by measurement of serum 25(OH)D3 using the AB SCIEX Triple Quad 4500 mass spectrometry system.
Findings: Of the 392 NHS healthcare workers, 214 (55%) had seroconverted for COVID-19. A total of 61 (15.6%) members of staff were vitamin D deficient (<30 nmol/l) with significantly more staff from BAME backgrounds or in a junior doctor role being deficient. Vitamin D levels were lower in those who were younger, had a higher BMI (>30 kg/m2), and were male. Multivariate analysis revealed that BAME and COVID-19 seroconversion were independent predictors of vitamin D deficiency. Staff who were vitamin D deficient were more likely to self-report symptoms of body aches and pains but importantly not the respiratory symptoms of cough and breathlessness. Vitamin D levels were lower in those COVID-19 positive staff who reported fever, but this did not reach statistical significance. Within the whole cohort there was an increase in seroconversion in staff with vitamin D deficiency compared to those without vitamin D deficiency (n=44/61, 72% vs n=170/331, 51%; p=0003); this was particularly marked in the proportion of BAME males who were vitamin D deficient compared to non-vitamin D deficient BAME males (n=17/18, 94% vs n=12/23, 52%; p=0005). Multivariate analysis revealed that vitamin D deficiency was an independent risk factor for seroconversion ( OR 2.6 , 95%CI 1.41-4.80; p=0.002).
Interpretation: In those healthcare workers who have isolated due to symptoms of COVID-19, those of BAME ethnicity are at the highest risk of vitamin D deficiency. Vitamin D deficiency is a risk factor for COVID-19 seroconversion for NHS healthcare workers especially in BAME male staff.
See also VitaminDWiki
COVID-19 treated by Vitamin D - studies, reports, videos
{include}
{include}
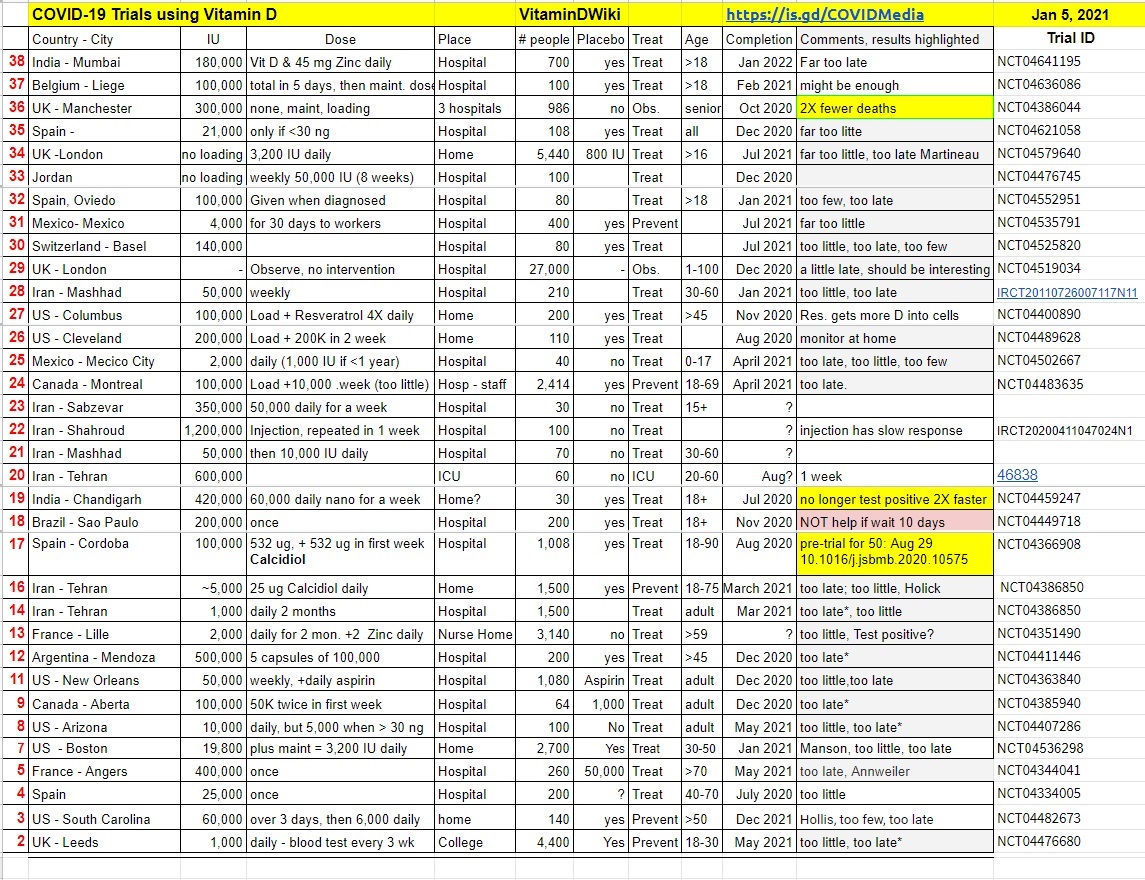
Many clinical trials are underway which are testing Vitamin D to fight COVID-19
See also web
Having a vitamin D deficiency could make you more likely to catch Covid-19, another study claims reporting on this study
COVID-19 Serology Testing Explained May 2020