Allergic Rhinitis fought by Vitamin D Army - video
Allergic Rhinitis Treatment: Game Changer Approach That Works
YouTube Cure4Health 42 minutes
Summary by Glasp and Claude AI
(00:35–02:41) The chronic burden of allergic rhinitis: Opens with the daily reality of living with allergic rhinitis—morning sneezing, congestion, brain fog—and the question patients stop asking: why does the immune system behave this way, and why hasn't a decade of antihistamines fixed it?
(03:05–08:20) Why prior remedies fell short: Acknowledges efforts with turmeric (poor bioavailability), tulsi, steam inhalation, jalneti (cleans surface but doesn't address immunity), Ayurveda (philosophically sound but lacks biochemical measurement), and homeopathy (no reproducible change in Th2 cytokines, IgE, or eosinophils). The core issue: tools weren't matched to the depth of the problem.
(08:20–09:49) The atopic march: Untreated Th2 dominance progresses predictably—atopic dermatitis → allergic rhinitis → asthma. Antihistamines manage output while the upstream process deepens.
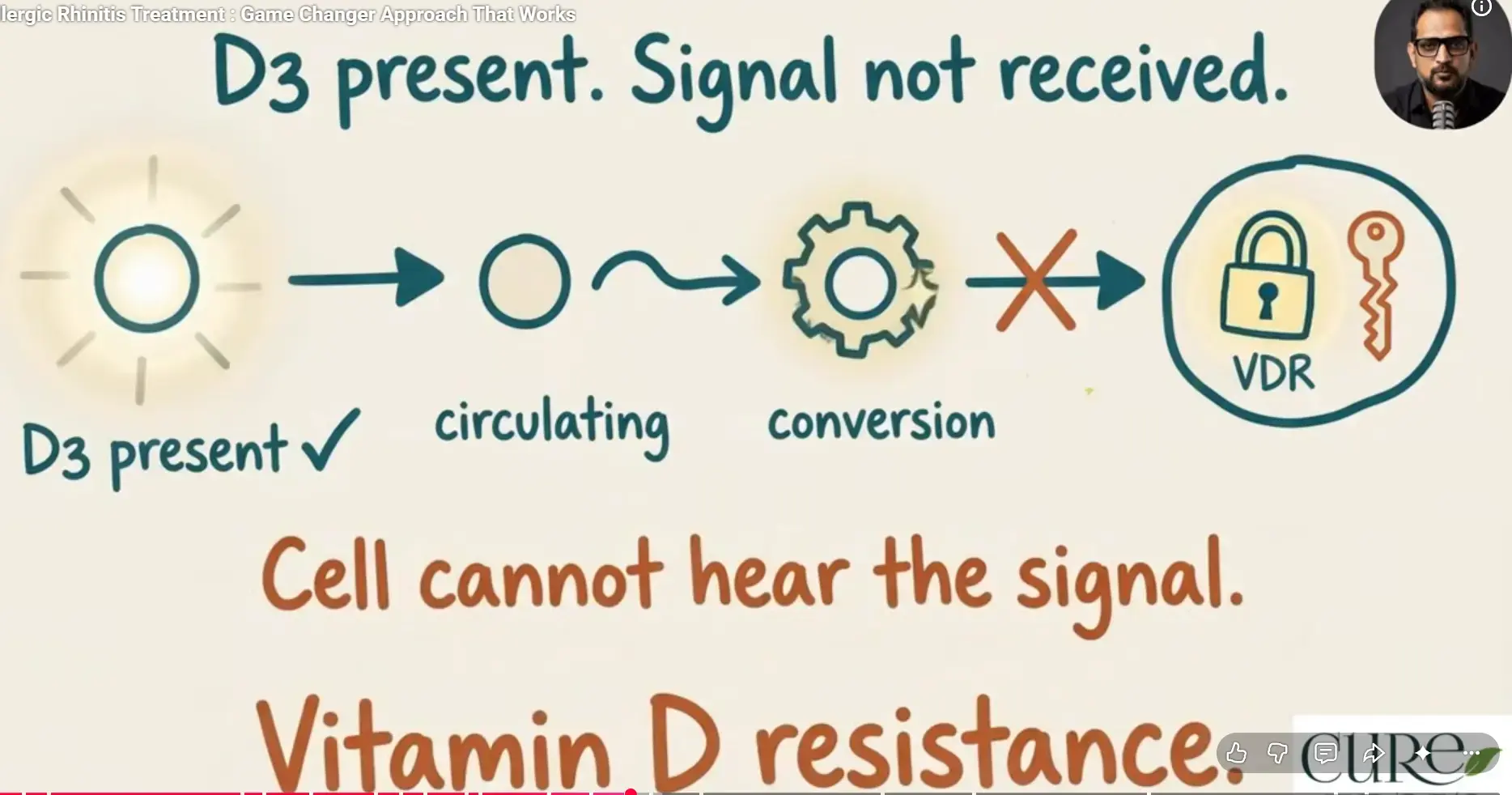
(09:49–12:29) Th1 vs. Th2 immune imbalance explained: In allergic rhinitis, T-regulatory command authority has collapsed and the Th2 arm misidentifies harmless particles (dust, pollen) as parasites. Cetirizine blocks the histamine receptor but doesn't stop mast cell activation or IgE production upstream.
(12:29–20:18) Three converging root drivers: (1) Gut dysbiosis—70% of immune system lives in the gut; probiotic intake showed 72% relative risk reduction in studies. (2) Vitamin D3 deficiency—a steroid hormone regulating 2,700+ genes and Th2 modulation; urban Indian populations show 47% deficiency vs. 7% rural, with atopy following the same gradient. (3) Chronic subclinical infection burden (parasitic, fungal, viral) that keeps Th2 chronically primed.
(20:18–25:24) Reading blood work through a systems lens: Most chronic patients have D3 below 25 ng/mL. Key markers include D3 + PTH (detects vitamin D resistance), total IgE (Th2 load), eosinophils (drivers of overactivation), fasting insulin (metabolic terrain), and free T3 (often ignored, but affects immune cell metabolism).
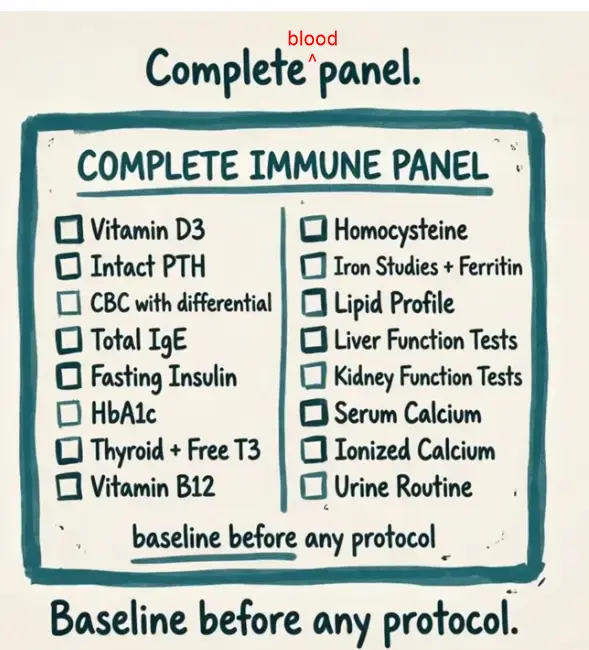
(25:24–27:16) Recommended testing panel: Speaker recommends Redcliffe Labs (in India) for cost and reach. Full panel: Vitamin D3, intact PTH, CBC with differential, total IgE, fasting insulin, HbA1c, thyroid with free T3, B12, homocysteine, iron/ferritin, lipids, LFT, KFT, calcium, ionized calcium, urine routine.
(27:16–32:25) Four-pronged therapeutic framework (requires clinical supervision): (1) Systematic gut rehabilitation—address infections, then spore-based probiotics + prebiotics + barrier repair. (2) D3 repletion with bile salt and digestive enzyme support, plus magnesium and K2 cofactors. (3) Targeted immune modulation with quercetin (mast cell stabilization), omega-3s, and vitamin C. (4) Metabolic and thyroid optimization.
(32:25–34:51) One terrain, many expressions: Eczema, food sensitivities, fatigue, morning stiffness, and reflux often accompany chronic rhinitis—they're not separate problems but one dysregulated immune-metabolic terrain.
(36:22–42:03) The window matters & closing message: Immune tolerance capacity is higher earlier in disease progression—the recoverable window narrows over time. Compliant integrative protocols typically show measurable improvement in 6–12 months. The channel does clinical practice (not comment-thread advice); first step is always blood work.
Related in VitaminDWiki
- Hay fever (Allergic Rhinitis) and Vitamin D - many studies
- Hay Fever treated by Vitamin D (50,000 IU weekly) – RCT
- Best supplements for hay fever (Quercetin, which activates the Vitamin D receptor)
Cofactors = Vitamin D Army